You might also like
- The Structure of PoetryDocument3 pagesThe Structure of PoetryRose Razo100% (1)
- Rebels - in - Frills - A - Literature - Review - On 4Document93 pagesRebels - in - Frills - A - Literature - Review - On 4mariobogarinNo ratings yet
- Biraogo vs. Philippine Truth CommissionDocument3 pagesBiraogo vs. Philippine Truth CommissionJulesMillanarNo ratings yet
- 16-Ergonomics Manual (Dan MacLeod) - English OnlyDocument28 pages16-Ergonomics Manual (Dan MacLeod) - English OnlyAnonymous tDZTSs100% (1)
- 16-Ergonomics Manual (Dan MacLeod) - English OnlyDocument28 pages16-Ergonomics Manual (Dan MacLeod) - English OnlyAnonymous tDZTSs100% (1)
- Democracy Against Domination PDFDocument257 pagesDemocracy Against Domination PDFvmcosNo ratings yet
- Manual - Nokia - AirScale - System Module - Presentation NokiaDocument29 pagesManual - Nokia - AirScale - System Module - Presentation NokiaAndres Obando100% (1)
- Jane Austen's Literary StyleDocument4 pagesJane Austen's Literary StyleGulfam RashidNo ratings yet
- Anthropometry As A Readily Accessible Health Assessment of Older AdultsDocument9 pagesAnthropometry As A Readily Accessible Health Assessment of Older AdultsFrancisco NascimentoNo ratings yet
- 2019 - Skeletal Muscle Mass As A Mortality PredictorDocument7 pages2019 - Skeletal Muscle Mass As A Mortality PredictorDiego Duarte CavalcanteNo ratings yet
- Mpi Geri PDFDocument6 pagesMpi Geri PDFJaka SusilaNo ratings yet
- Reliabilitas Pengukuran Inter Dan Intraobserver AntropometriDocument7 pagesReliabilitas Pengukuran Inter Dan Intraobserver AntropometriRifka Laily MafazaNo ratings yet
- A23 AJCN Weight, Shape, and Mortality Risk in Older PersonsDocument12 pagesA23 AJCN Weight, Shape, and Mortality Risk in Older PersonsGabriel CampolinaNo ratings yet
- Body Mass Index in The Elderly and Its Correlation With Anthropometric Parameters Evaluated by Body ImpedanceDocument6 pagesBody Mass Index in The Elderly and Its Correlation With Anthropometric Parameters Evaluated by Body ImpedanceHerald Scholarly Open AccessNo ratings yet
- Gemeos Derma ToDocument6 pagesGemeos Derma ToFranco CastroNo ratings yet
- Assessing The Relationship BetweenDocument6 pagesAssessing The Relationship BetweenTri Eka JuliantoNo ratings yet
- Antropometria y BIADocument6 pagesAntropometria y BIAnicolas ramirezNo ratings yet
- KJFM 34 281Document8 pagesKJFM 34 281Dian AuliaNo ratings yet
- A Special Literature Review On Anthropometry: (MATRIC NO: 178321043)Document13 pagesA Special Literature Review On Anthropometry: (MATRIC NO: 178321043)OWOLABINo ratings yet
- Perception of Body Image As Indicator of Weight Status in The European UnionDocument10 pagesPerception of Body Image As Indicator of Weight Status in The European UnionJuanPauloMúneraRuedaNo ratings yet
- Predictive Validity of Handgrip Strength Vertical Jump Power and Plank Time in The Identification of Pediatric SarcopeniaDocument11 pagesPredictive Validity of Handgrip Strength Vertical Jump Power and Plank Time in The Identification of Pediatric SarcopeniaMessias FilhoNo ratings yet
- Medidas AntropométricasDocument8 pagesMedidas AntropométricasCarolina JaramilloNo ratings yet
- 6 Year Changes in Body Composition in Women at Mid-Life Ovarian and Chronological AgingDocument15 pages6 Year Changes in Body Composition in Women at Mid-Life Ovarian and Chronological AgingConstanza MillánNo ratings yet
- Serum Leptin Levels Are Associated With Bone Mass in Nonobese WomenDocument4 pagesSerum Leptin Levels Are Associated With Bone Mass in Nonobese WomenTemtem HmNo ratings yet
- Frisancho1984 1Document12 pagesFrisancho1984 1AdelaNo ratings yet
- Height, Weight, and Body Mass Index of Elderly Persons in TaiwanDocument7 pagesHeight, Weight, and Body Mass Index of Elderly Persons in TaiwanSamuel XiaoNo ratings yet
- JGK-vol.11, No. 26 Juli 2019: Jurnal Gizi Dan Kesehatan 132Document7 pagesJGK-vol.11, No. 26 Juli 2019: Jurnal Gizi Dan Kesehatan 132Wanda Novia P SNo ratings yet
- Maturitas: SciencedirectDocument6 pagesMaturitas: Sciencedirectaeroforce20No ratings yet
- Hemoglobin Levels and Skeletal Muscle Results From The InCHIANTI StudyDocument6 pagesHemoglobin Levels and Skeletal Muscle Results From The InCHIANTI Studysantiago carrillo medinaNo ratings yet
- Epid 1Document4 pagesEpid 1Annafiatu zakiahNo ratings yet
- MC Dowell 2008 NHSR 010Document46 pagesMC Dowell 2008 NHSR 010fgeafadaedNo ratings yet
- Gao Et Al.Document6 pagesGao Et Al.Dries Van ThielenNo ratings yet
- AnthropometricDocument6 pagesAnthropometricCelline PangestiNo ratings yet
- Self-Reported and Measured Weight, Height and Body Mass Index (BMI) in Italy, The Netherlands and North AmericaDocument6 pagesSelf-Reported and Measured Weight, Height and Body Mass Index (BMI) in Italy, The Netherlands and North AmericaVeton HaliliNo ratings yet
- Prevalencia Sarcopenia en ChileDocument6 pagesPrevalencia Sarcopenia en ChileFrancisco Mancilla LobosNo ratings yet
- Appetite: Michael Chourdakis, Thrasivoulos Tzellos, Georgios Papazisis, Konstantinos Toulis, Dimitrios KouvelasDocument4 pagesAppetite: Michael Chourdakis, Thrasivoulos Tzellos, Georgios Papazisis, Konstantinos Toulis, Dimitrios KouvelasHarwinNo ratings yet
- The Prevalence of in The Knee Osteoarthritis ElderlyDocument5 pagesThe Prevalence of in The Knee Osteoarthritis Elderlyqurrat ul ann haiderNo ratings yet
- The Estimation of Body Height From Ulna Length in Healthy Adults From Different Ethnic GroupsDocument8 pagesThe Estimation of Body Height From Ulna Length in Healthy Adults From Different Ethnic GroupsRodríguez Brown FrancoNo ratings yet
- Gastritis 1Document5 pagesGastritis 1IttyNo ratings yet
- Insight On Pathogenesis of Lifelong Premature Ejaculation: Inverse Relationship Between Lifelong Premature Ejaculation and ObesityDocument4 pagesInsight On Pathogenesis of Lifelong Premature Ejaculation: Inverse Relationship Between Lifelong Premature Ejaculation and ObesitymaithamNo ratings yet
- 3.@20stamatakis Etal09 BJNDocument9 pages3.@20stamatakis Etal09 BJNjrodascNo ratings yet
- Body Mass Index and Susceptibility To Knee Osteoarthritis: A Systematic Review and Meta-AnalysisDocument7 pagesBody Mass Index and Susceptibility To Knee Osteoarthritis: A Systematic Review and Meta-AnalysisAmalia RosaNo ratings yet
- 24 1520325260 - 06-03-2018 PDFDocument9 pages24 1520325260 - 06-03-2018 PDFEditor IJRITCCNo ratings yet
- Arth2011 580632Document6 pagesArth2011 580632hylee102594No ratings yet
- Rutherford 1993Document5 pagesRutherford 1993ManuelMartinezMartínezNo ratings yet
- Pereira 2015Document9 pagesPereira 2015Amalia RosaNo ratings yet
- Altura Promedio en México Estudio de CasoDocument8 pagesAltura Promedio en México Estudio de CasoEddy HarosNo ratings yet
- Tinetti Mobility Test Is Related To Muscle Mass and Strength in Non-Institutionalized Elderly PeopleDocument9 pagesTinetti Mobility Test Is Related To Muscle Mass and Strength in Non-Institutionalized Elderly PeopleAlejandro GuzmanNo ratings yet
- 10 1016@j Archger 2020 104106Document5 pages10 1016@j Archger 2020 104106Nissa UlfitriaNo ratings yet
- Physical Characteristicsat Different AgesDocument8 pagesPhysical Characteristicsat Different AgesgizingmhNo ratings yet
- Sedentary Behavior, Physical Inactivity, AbdominalDocument11 pagesSedentary Behavior, Physical Inactivity, AbdominalJose VasquezNo ratings yet
- Normal Sagittal Parameters of Global Spinal Balance in Children and Adolescents - A Prospective Study of 646 Asymptomatic SubjectsDocument8 pagesNormal Sagittal Parameters of Global Spinal Balance in Children and Adolescents - A Prospective Study of 646 Asymptomatic Subjectskartini ciatawiNo ratings yet
- OutDocument7 pagesOutMario AlexanderNo ratings yet
- Balace 2Document7 pagesBalace 2astrinila fauziNo ratings yet
- DownloadDocument7 pagesDownloadcesar8319No ratings yet
- Physiotherapy Management of Hip OsteoarthritisDocument14 pagesPhysiotherapy Management of Hip Osteoarthritisaraaela 25No ratings yet
- Journal of Clinical Gerontology & Geriatrics: Original ArticleDocument6 pagesJournal of Clinical Gerontology & Geriatrics: Original ArticleDeedee RenovaldiNo ratings yet
- Effects of High-Impact Exercise On Ultrasonic and Biochemical Indices of Skeletal Status: A Prospective Study in Young Male GymnastsDocument9 pagesEffects of High-Impact Exercise On Ultrasonic and Biochemical Indices of Skeletal Status: A Prospective Study in Young Male GymnastsCláudio MeirelesNo ratings yet
- 2 Article Summary WordDocument5 pages2 Article Summary Wordapi-253310427No ratings yet
- Nisha - OA 3Document6 pagesNisha - OA 3JeveraNo ratings yet
- European Journal of Theoretical and Applied SciencesDocument9 pagesEuropean Journal of Theoretical and Applied SciencesEJTAS journalNo ratings yet
- Herssens Et Al. 2018 - Do Spatiotemporal Parameters and Gait Variability Differ Across The Lifespan of Healthy Adults A Systematic Review FinalDocument10 pagesHerssens Et Al. 2018 - Do Spatiotemporal Parameters and Gait Variability Differ Across The Lifespan of Healthy Adults A Systematic Review FinalHerr FrauNo ratings yet
- Risk Factors For Pelvic Organ Prolapse: C.M. Kim, M.J. Jeon, D.J. Chung, S.K. Kim, J.W. Kim, S.W. BaiDocument4 pagesRisk Factors For Pelvic Organ Prolapse: C.M. Kim, M.J. Jeon, D.J. Chung, S.K. Kim, J.W. Kim, S.W. BaiAkame No IDNo ratings yet
- Physical Therapy in Sport: Literature ReviewDocument9 pagesPhysical Therapy in Sport: Literature ReviewPrincess Dianna SulitNo ratings yet
- Relation Sleep Obes and BPDocument18 pagesRelation Sleep Obes and BPMumtaz MaulanaNo ratings yet
- ARTICLEMuscle Mass Measured Using Bioelectrical Impedanceanalysis, Calf Circumference and Grip Strength in OlderadultsDocument5 pagesARTICLEMuscle Mass Measured Using Bioelectrical Impedanceanalysis, Calf Circumference and Grip Strength in OlderadultsPPDS Rehab Medik UnhasNo ratings yet
- Centenarians: An Example of Positive BiologyFrom EverandCentenarians: An Example of Positive BiologyCalogero CarusoNo ratings yet
- TSN Common Clip AngleDocument1 pageTSN Common Clip AngleBien Carlos Esteves ViaNo ratings yet
- Ten Shades of Green by Peter BuchananDocument34 pagesTen Shades of Green by Peter BuchananBien Carlos Esteves ViaNo ratings yet
- 01 Principles of ArchitectureDocument2 pages01 Principles of ArchitectureVail LunorNo ratings yet
- Final Paper 110218Document156 pagesFinal Paper 110218Bien Carlos Esteves ViaNo ratings yet
- Building 1 A3Document1 pageBuilding 1 A3Bien Carlos Esteves ViaNo ratings yet
- Professional Practice 1:: National University College of Architecture and ArtsDocument12 pagesProfessional Practice 1:: National University College of Architecture and ArtsBien Carlos Esteves ViaNo ratings yet
- Tutorial 1: Getting Started Using Ilwis Open & Geonetcast ToolboxDocument10 pagesTutorial 1: Getting Started Using Ilwis Open & Geonetcast ToolboxBien Carlos Esteves ViaNo ratings yet
- CH 1Document22 pagesCH 1Bien Carlos Esteves ViaNo ratings yet
- Behavior GeneticsDocument16 pagesBehavior GeneticsBien Carlos Esteves ViaNo ratings yet
- Tool Impact of Aging 2016Document7 pagesTool Impact of Aging 2016Bien Carlos Esteves ViaNo ratings yet
- Chatterjee - King - Best Cities For Successful AgingDocument66 pagesChatterjee - King - Best Cities For Successful AgingBien Carlos Esteves ViaNo ratings yet
- 2 ConceptualBlockbusting PDFDocument22 pages2 ConceptualBlockbusting PDFBien Carlos Esteves ViaNo ratings yet
- Population LivingArrangementsDocument34 pagesPopulation LivingArrangementsHetty ParsramNo ratings yet
- November 17, 2017Document24 pagesNovember 17, 2017Bien Carlos Esteves ViaNo ratings yet
- CH 1Document22 pagesCH 1Bien Carlos Esteves ViaNo ratings yet
- Designing Homes For The Elderly Based On The Anthropometry of Older MalaysiansDocument9 pagesDesigning Homes For The Elderly Based On The Anthropometry of Older MalaysiansmelpillNo ratings yet
- The Modulor: Le CorbusierDocument12 pagesThe Modulor: Le Corbusiermilena126No ratings yet
- Mental Health and PsychologyDocument6 pagesMental Health and PsychologyBien Carlos Esteves ViaNo ratings yet
- Vitruvian Man Scientific MethodDocument1 pageVitruvian Man Scientific MethodBien Carlos Esteves ViaNo ratings yet
- 1 s2.0 S1877042811026231 MainDocument11 pages1 s2.0 S1877042811026231 MainBien Carlos Esteves ViaNo ratings yet
- PL WL: Positive Bending, Tension at Bottom Max. Positive MomentDocument2 pagesPL WL: Positive Bending, Tension at Bottom Max. Positive MomentBien Carlos Esteves ViaNo ratings yet
- Design of Highrise BuildingsDocument32 pagesDesign of Highrise BuildingsSangita Sangam100% (1)
- Design Guide SmallDocument154 pagesDesign Guide Smallfansforever9125No ratings yet
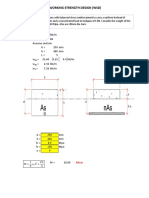
- Working Strength DesignpdfDocument2 pagesWorking Strength DesignpdfBien Carlos Esteves ViaNo ratings yet
- 02 Traditional Design ProceduresDocument2 pages02 Traditional Design ProceduresBien Carlos Esteves ViaNo ratings yet
- Financial Management Notes - Dividend Decision - Dynamic Tutorials and ServicesDocument10 pagesFinancial Management Notes - Dividend Decision - Dynamic Tutorials and Servicessimranarora2007No ratings yet
- Advanced Accounting PDFDocument14 pagesAdvanced Accounting PDFYvette Pauline JovenNo ratings yet
- Sec. Gr. To BT History Temp Panel 2013Document50 pagesSec. Gr. To BT History Temp Panel 2013edwin_prakash75No ratings yet
- Test Bank For Oral Pathology 7th Edition by RegeziDocument11 pagesTest Bank For Oral Pathology 7th Edition by RegeziSteve Isola100% (23)
- Mananquil v. MoicoDocument2 pagesMananquil v. Moicoangelo prietoNo ratings yet
- MTSC QuestionsDocument8 pagesMTSC QuestionsAbhi RamNo ratings yet
- Advanced Engineering Mathematics 10th EditionDocument7 pagesAdvanced Engineering Mathematics 10th EditionsamuelNo ratings yet
- Oscillator Types and CharacteristicsDocument4 pagesOscillator Types and Characteristicspriyadarshini212007No ratings yet
- Neco Catlog 4 FoldDocument2 pagesNeco Catlog 4 FoldSanket PhatangareNo ratings yet
- Summative Test 1Document3 pagesSummative Test 1Glenda AstodilloNo ratings yet
- The Concept of Social Capital: A Critical Review: Sophie Ponthieux ( )Document23 pagesThe Concept of Social Capital: A Critical Review: Sophie Ponthieux ( )Ali Muhtarom LilikNo ratings yet
- 3 Materi 5 TOEFLDocument14 pages3 Materi 5 TOEFL0029 Lona Anggina NstNo ratings yet
- Breakfast For Kirsten GillibrandDocument5 pagesBreakfast For Kirsten GillibrandSunlight FoundationNo ratings yet
- Hatch-Slack PathwayDocument10 pagesHatch-Slack Pathwaychurail khanNo ratings yet
- Current Openings: The Sirpur Paper Mills LTDDocument3 pagesCurrent Openings: The Sirpur Paper Mills LTDMano VardhanNo ratings yet
- Edexcel iGCSE ICT Software MindmapDocument1 pageEdexcel iGCSE ICT Software MindmapPaul ZambonNo ratings yet
- Hydraulic Caliper Service Manual MM0266Document27 pagesHydraulic Caliper Service Manual MM0266LUKASNo ratings yet
- Mathematics Engagement in An Australian Lower Secondary SchoolDocument23 pagesMathematics Engagement in An Australian Lower Secondary SchoolDane SinclairNo ratings yet
- Business Studies Project: Made By: Rahil JainDocument29 pagesBusiness Studies Project: Made By: Rahil JainChirag KothariNo ratings yet
- BeadsDocument8 pagesBeadsMukesh MonuNo ratings yet
- DR Horton Homeowners ManualDocument80 pagesDR Horton Homeowners ManualLynn RaisesNo ratings yet
- Liquichek Specialty Immunoassay Control Levels LTA, 1, 2 and 3Document6 pagesLiquichek Specialty Immunoassay Control Levels LTA, 1, 2 and 3clinicalbiochemistryNo ratings yet
- 285519-35126-30-case-studyDocument12 pages285519-35126-30-case-studyapi-737834018No ratings yet
- 5187 0103Document141 pages5187 0103Aravind ArjunanNo ratings yet