You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- HP Proliant DL380 G6 Server - Step by StepDocument9 pagesHP Proliant DL380 G6 Server - Step by StepBoss100% (1)
- Upcoming: Advisor Webcast: Oracle Database Resource ManagerDocument41 pagesUpcoming: Advisor Webcast: Oracle Database Resource ManagerLayne MoránNo ratings yet
- Dell XPS 17 Quanta GM7 Rev D SchematicsDocument39 pagesDell XPS 17 Quanta GM7 Rev D SchematicsvcompumatikNo ratings yet
- CoolebrookDocument31 pagesCoolebrookloganatahnNo ratings yet
- Study of Educational Aspiration and Socio-Economic Status of Secondary School StudentsDocument11 pagesStudy of Educational Aspiration and Socio-Economic Status of Secondary School StudentsvivekNo ratings yet
- HR Wallingford-009 - Wave - GaugeDocument2 pagesHR Wallingford-009 - Wave - GaugeSutanto HadiNo ratings yet
- Detailedlessonplanintrigonometry 130303203030 Phpapp01Document4 pagesDetailedlessonplanintrigonometry 130303203030 Phpapp01Hazel Clemente CarreonNo ratings yet
- Mechanics of MaterialsDocument11 pagesMechanics of MaterialsMagesh KumarNo ratings yet
- Maharashtra State Board of Technical Education (Autonomous) (ISO/IEC - 27001 - 2005 Certified) Winter - 2022 Examination Model Answer Subject: 22619Document22 pagesMaharashtra State Board of Technical Education (Autonomous) (ISO/IEC - 27001 - 2005 Certified) Winter - 2022 Examination Model Answer Subject: 22619Pratiksha JadhavNo ratings yet
- Programming: Simon ScheideggerDocument90 pagesProgramming: Simon ScheideggerRuben KempterNo ratings yet
- Configuring Routing by Using Routing and Remote AccessDocument31 pagesConfiguring Routing by Using Routing and Remote AccessLacus ClyneNo ratings yet
- Hide Answer Notebook Notebook Discuss: Here Is The Answer and ExplanationDocument16 pagesHide Answer Notebook Notebook Discuss: Here Is The Answer and ExplanationPayashwini KulkarniNo ratings yet
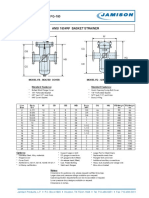
- FB-150 FQ-150 Basket StrainerDocument1 pageFB-150 FQ-150 Basket Strainerklich77No ratings yet
- 7 - Introduction To Intelligent ControlDocument21 pages7 - Introduction To Intelligent ControlIsmael Espinoza100% (1)
- Unit-III - EEFA - CostsDocument70 pagesUnit-III - EEFA - CostsRamalingam ChandrasekharanNo ratings yet
- Manual Dimmer BukeDocument10 pagesManual Dimmer BukeJavi KatzNo ratings yet
- EARTH AND LIFE SCIENCE II Answer KeyDocument4 pagesEARTH AND LIFE SCIENCE II Answer Keyjelena jorgeoNo ratings yet
- Haaland EquationDocument1 pageHaaland EquationAmir AzmiNo ratings yet
- Structure Lab Manual FullDocument318 pagesStructure Lab Manual FullRodrigo Requelme BorjaNo ratings yet
- Physics XIDocument13 pagesPhysics XIArokiaraj RajNo ratings yet
- C 13Document33 pagesC 13rgerwwaaNo ratings yet
- SOPRANO TIM SMTP Interface Developers GuideDocument43 pagesSOPRANO TIM SMTP Interface Developers GuidenettellectNo ratings yet
- Enhancement of IDoc TypeDocument12 pagesEnhancement of IDoc TypeRakesh RaiNo ratings yet
- Rsa Netwitness Logs and Packets: Server, Dac and San HW SpecificationsDocument10 pagesRsa Netwitness Logs and Packets: Server, Dac and San HW SpecificationsfunyiroemberNo ratings yet
- Rpzf2: Product Data SheetDocument4 pagesRpzf2: Product Data SheetJosé RincónNo ratings yet
- Unit Iv Ce 6405Document13 pagesUnit Iv Ce 6405HanafiahHamzahNo ratings yet
- Simple MachinesDocument25 pagesSimple MachinesMay ArispeNo ratings yet
- How Microprocessors Work PDFDocument2 pagesHow Microprocessors Work PDFdanielconstantin4No ratings yet
- What Is Lincdoc?Document2 pagesWhat Is Lincdoc?Daniel O'Leary0% (1)
- MSC Academic Guide - Admission Test PDFDocument13 pagesMSC Academic Guide - Admission Test PDFTonoy Peter CorrayaNo ratings yet