You might also like
- DCHDocument163 pagesDCHLuiza Radulescu100% (2)
- Supliment 3 2014 PDFDocument144 pagesSupliment 3 2014 PDFLuiza RadulescuNo ratings yet
- Pediatric DermatologyDocument568 pagesPediatric DermatologyLuiza Radulescu89% (9)
- Antenatal Sonographic Features of Poland Syndrome On 2-And 3-Dimensional SonographyDocument2 pagesAntenatal Sonographic Features of Poland Syndrome On 2-And 3-Dimensional SonographyLuiza RadulescuNo ratings yet
- Placenta and Fetal Membranes Total Tulane UniversityDocument8 pagesPlacenta and Fetal Membranes Total Tulane UniversityLuiza RadulescuNo ratings yet
- Inherited and Acquired Thrombophilia - Pregnancy Outcome and TreatmentDocument22 pagesInherited and Acquired Thrombophilia - Pregnancy Outcome and TreatmentLuiza RadulescuNo ratings yet
- Doppler Ultrasound in The Assessment of Suspected Intra-Uterine Growth Restriction AL Qahtani N - Ann Afr MedDocument8 pagesDoppler Ultrasound in The Assessment of Suspected Intra-Uterine Growth Restriction AL Qahtani N - Ann Afr MedLuiza RadulescuNo ratings yet
- What's So Bad About Teenage Pregnancy?Document7 pagesWhat's So Bad About Teenage Pregnancy?Luiza RadulescuNo ratings yet
- Mandel PresentationDocument26 pagesMandel PresentationLuiza RadulescuNo ratings yet
- A1 Template V5Document1 pageA1 Template V5Luiza RadulescuNo ratings yet
- Sga/Iugr: Sue Ann Smith, MD Neonatologist Doernbecher Neonatal Care CenterDocument17 pagesSga/Iugr: Sue Ann Smith, MD Neonatologist Doernbecher Neonatal Care CenterLuiza RadulescuNo ratings yet
- Iugr International Journal of Og 2006Document8 pagesIugr International Journal of Og 2006Luiza RadulescuNo ratings yet
- Functions of Iron-Overview: e Donor and AcceptorDocument41 pagesFunctions of Iron-Overview: e Donor and AcceptorLuiza RadulescuNo ratings yet
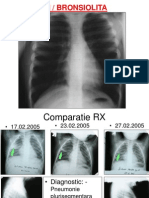
- Astm / BronsiolitaDocument20 pagesAstm / BronsiolitaLuiza RadulescuNo ratings yet
- Durerile Abdominale RecurenteDocument37 pagesDurerile Abdominale RecurenteLuiza RadulescuNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- 2-Acute Abdominal PainDocument24 pages2-Acute Abdominal Painabdalmajeed alshammaryNo ratings yet
- A Theory of The Human Need For OccupationDocument9 pagesA Theory of The Human Need For OccupationNel HinilzaNo ratings yet
- Congestive Heart Failure Pathophysiology Schematic DiagramDocument3 pagesCongestive Heart Failure Pathophysiology Schematic DiagramJasleen KaurNo ratings yet
- X Ray Diffraction Safety InformationDocument48 pagesX Ray Diffraction Safety Informationrenjith2017100% (1)
- Revised Week 3Document61 pagesRevised Week 3John Teo DalisaymoNo ratings yet
- Consumer Behaviour Towards Healtth Care ProductsDocument46 pagesConsumer Behaviour Towards Healtth Care ProductsJayesh Makwana50% (2)
- Fun Games - 1 Min Game 01Document9 pagesFun Games - 1 Min Game 01Purvi ShahNo ratings yet
- IOT Based Health Monitoring SystemDocument3 pagesIOT Based Health Monitoring SystemInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Pelvic Fracture Case StudyDocument48 pagesPelvic Fracture Case StudyYves BasanNo ratings yet
- Communication in Palliative CareDocument7 pagesCommunication in Palliative CareIhsan NudinNo ratings yet
- Gavi - 2015 Country TA RFIDocument20 pagesGavi - 2015 Country TA RFIDeepakSinghNo ratings yet
- Nursing Skills FairDocument4 pagesNursing Skills Fairstuffednurse100% (1)
- 9401-Article Text-17650-1-10-20200718Document5 pages9401-Article Text-17650-1-10-20200718agail balanagNo ratings yet
- IEEE Guide To The Assembly and Erection of Concrete Pole StructuresDocument32 pagesIEEE Guide To The Assembly and Erection of Concrete Pole Structuresalex aedoNo ratings yet
- CFPC SampsDocument39 pagesCFPC SampsSumer Chauhan100% (9)
- Corpus Alienum PneumothoraxDocument3 pagesCorpus Alienum PneumothoraxPratita Jati PermatasariNo ratings yet
- Pediatric Blood PressureDocument28 pagesPediatric Blood PressureGenta Syaifrin Laudza0% (1)
- CSEC Biology June 2012 P2Document17 pagesCSEC Biology June 2012 P2Joy BoehmerNo ratings yet
- Risk Assessment - TemplateDocument10 pagesRisk Assessment - TemplateJohn KalvinNo ratings yet
- India's #1 Nroute Daily Whey Protein Powder Online 2022Document3 pagesIndia's #1 Nroute Daily Whey Protein Powder Online 2022NRoute ProteinNo ratings yet
- Chapter 1: Introduction To Coaching: Confidential Page 1 of 52 5/1/2009Document52 pagesChapter 1: Introduction To Coaching: Confidential Page 1 of 52 5/1/2009James ZacharyNo ratings yet
- Neonatal Thrush of Newborns Oral CandidiasisDocument3 pagesNeonatal Thrush of Newborns Oral CandidiasisYeni PuspitasariNo ratings yet
- PN 1Document1 pagePN 1Florin Eugen ConstantinescuNo ratings yet
- EO Supporting The Immunization Activities - EditedDocument2 pagesEO Supporting The Immunization Activities - EditedDem SalazarNo ratings yet
- Electrical Safety in HealthcareDocument2 pagesElectrical Safety in HealthcareNur Aqilah IsmailNo ratings yet
- Accuracy of The Demirjian and Willems MethodsDocument8 pagesAccuracy of The Demirjian and Willems MethodsProfessor T. A. EsanNo ratings yet
- LlageriDocument8 pagesLlageriBlodin ZylfiuNo ratings yet
- Analysis of Shift in Consumption of Carbonated Beverages To Healthy DrinksDocument26 pagesAnalysis of Shift in Consumption of Carbonated Beverages To Healthy DrinksAntara JasrotiaNo ratings yet
- 9 13 23NCM 111 Nursing Research 1 AY 2023 2024Document19 pages9 13 23NCM 111 Nursing Research 1 AY 2023 2024bhazferrer2No ratings yet
- Cbse Term 1 Final Exam Instructions 2021-21Document9 pagesCbse Term 1 Final Exam Instructions 2021-21Eshaan123thebestNo ratings yet