You might also like
- Chronic Lymphocytic LeukemiaFrom EverandChronic Lymphocytic LeukemiaMichael HallekNo ratings yet
- Advances in Immunology: I D C D PDocument12 pagesAdvances in Immunology: I D C D PDatulna Benito Mamaluba Jr.No ratings yet
- Neutrophils: in Health and DiseaseDocument65 pagesNeutrophils: in Health and DiseaseKush Pathak100% (1)
- Ni Hms 465710Document38 pagesNi Hms 465710AmelyalesmanaNo ratings yet
- Out 7Document8 pagesOut 7Musthafa Afif WardhanaNo ratings yet
- Extraarticular Features of Rheumatoid ArthritisDocument13 pagesExtraarticular Features of Rheumatoid ArthritisHebert Aldo SalazarNo ratings yet
- Perioral Dermatitis: Acta Dermatovenerologica Croatica: ADC / Hrvatsko Dermatolosko Drustvo February 2008Document6 pagesPerioral Dermatitis: Acta Dermatovenerologica Croatica: ADC / Hrvatsko Dermatolosko Drustvo February 2008Firdani MutiaraNo ratings yet
- Ocular Manifestations of SLEDocument9 pagesOcular Manifestations of SLEChiquitaPutriVaniaRauNo ratings yet
- Aetiology & Pathogenesis of Periodontal Disease: DR Luan NgoDocument73 pagesAetiology & Pathogenesis of Periodontal Disease: DR Luan NgoPolo RalfNo ratings yet
- Statins and Chameleon-Like'' Cutaneous Eruptions: Simvastatin-Induced Acral Cutaneous Vesiculobullous and Pustular Eruption in A 70-Year-Old ManDocument5 pagesStatins and Chameleon-Like'' Cutaneous Eruptions: Simvastatin-Induced Acral Cutaneous Vesiculobullous and Pustular Eruption in A 70-Year-Old ManBeatriz VásquezNo ratings yet
- Presentation 2Document32 pagesPresentation 2Dr. Bashir MehrNo ratings yet
- Perioral DermatitisDocument6 pagesPerioral DermatitisYeni OktaviaNo ratings yet
- PeriodontitisDocument32 pagesPeriodontitisDimitrios PapadopoulosNo ratings yet
- Seminars in Diagnostic Pathology: Mark R. WickDocument11 pagesSeminars in Diagnostic Pathology: Mark R. WickAbdillah AkbarNo ratings yet
- Seminars in Diagnostic Pathology: Bullous, Pseudobullous, & Pustular DermatosesDocument11 pagesSeminars in Diagnostic Pathology: Bullous, Pseudobullous, & Pustular DermatosesCynthia OktariszaNo ratings yet
- Salivary Gland DiseaseDocument18 pagesSalivary Gland DiseaseEkky Rizky MaulanaNo ratings yet
- Drug Induced Drug PathologyDocument13 pagesDrug Induced Drug PathologyBagus Putra KurniawanNo ratings yet
- Desquamative Gingivitis: A Sign of Mucocutaneous Disorders - A ReviewDocument6 pagesDesquamative Gingivitis: A Sign of Mucocutaneous Disorders - A Reviewsidra malikNo ratings yet
- Leukocyte Adhesion Deficiency SyndromeDocument25 pagesLeukocyte Adhesion Deficiency SyndromeperioassNo ratings yet
- 2021 Nail and Systemic DiseasesDocument21 pages2021 Nail and Systemic Diseaseshaytham aliNo ratings yet
- Etiology and Pathogenesis: Nonepithelial White-Yellow LesionsDocument6 pagesEtiology and Pathogenesis: Nonepithelial White-Yellow LesionsXavier AltamiranoNo ratings yet
- Immune 2Document5 pagesImmune 2Patricia DagantaNo ratings yet
- Reactive Changes in Blood Film: Integrated Module Phase 1 Third StageDocument24 pagesReactive Changes in Blood Film: Integrated Module Phase 1 Third Stagerezataheri749No ratings yet
- Chédiak Higashi SyndromeDocument18 pagesChédiak Higashi SyndromePurwana NasirNo ratings yet
- Artigo Periodontia 2Document13 pagesArtigo Periodontia 2DANIELA MARTINS LEITENo ratings yet
- Gene Related DiseaseDocument3 pagesGene Related Diseasevivek govardhanamNo ratings yet
- E Scleroderma Ye Scleroderma LikeDocument31 pagesE Scleroderma Ye Scleroderma LikeHmn07No ratings yet
- Linfadenitis GranulomatosaDocument16 pagesLinfadenitis GranulomatosaIlse Lucero RodriguezNo ratings yet
- Pustular Diseases: Laboratory Findings, DiagnosisDocument4 pagesPustular Diseases: Laboratory Findings, DiagnosisPutra ImanullahNo ratings yet
- Immunodeficiency Disease: Primary ImmunodeficienciesDocument8 pagesImmunodeficiency Disease: Primary ImmunodeficienciesAbo AmgadNo ratings yet
- Ghid Oftalmologic Preview PlusDocument6 pagesGhid Oftalmologic Preview PlusIoana ElenaNo ratings yet
- A Case of Ulcerative Livedoid Vasculopathy Treated Successfully With Pentoxifylline and ColchicineDocument4 pagesA Case of Ulcerative Livedoid Vasculopathy Treated Successfully With Pentoxifylline and Colchicinekahkashanahmed065No ratings yet
- Sarcoma de Kaposi PDFDocument4 pagesSarcoma de Kaposi PDFXavier AltamiranoNo ratings yet
- Gefs Etiologia Agatti Conh 12Document8 pagesGefs Etiologia Agatti Conh 12Leoncio SerranoNo ratings yet
- Perioral Dermatitis PDFDocument6 pagesPerioral Dermatitis PDFanissa fitriNo ratings yet
- Sindrom Chediak HigashiDocument8 pagesSindrom Chediak HigashiDiana AstriaNo ratings yet
- Differential Diagnosis of Leprosy: Samuel L MoschellaDocument25 pagesDifferential Diagnosis of Leprosy: Samuel L Moschellama hNo ratings yet
- Disorders of LeukocytesDocument30 pagesDisorders of LeukocytesLaura Daniela MurilloNo ratings yet
- 13 CR Lethal MidlineDocument3 pages13 CR Lethal MidlineSudhir BayyaNo ratings yet
- 20140622164942507Document2 pages20140622164942507meddyaaNo ratings yet
- Periradicular Lesions (Chapter 5)Document28 pagesPeriradicular Lesions (Chapter 5)revlieeNo ratings yet
- AVIAN - Diseases of The Avian SpleenDocument7 pagesAVIAN - Diseases of The Avian Spleentaner_soysuren100% (1)
- Morphological Anomalies of Circulating Blood CellsDocument3 pagesMorphological Anomalies of Circulating Blood CellsAmanda OliveiraNo ratings yet
- Dermatologia: Anais Brasileiros deDocument3 pagesDermatologia: Anais Brasileiros deSango AyraNo ratings yet
- Autoimmune DisordersDocument33 pagesAutoimmune DisordersSuhas IngaleNo ratings yet
- 494 PDFDocument6 pages494 PDFranz ibonkNo ratings yet
- Perioral DermatitisDocument5 pagesPerioral DermatitisAstriana IndrawatiNo ratings yet
- Psoriasis: Common DermatosesDocument7 pagesPsoriasis: Common DermatoseslaluneNo ratings yet
- Lee 2001Document9 pagesLee 2001Astop WarijoNo ratings yet
- Esquemas OclusalesDocument18 pagesEsquemas OclusalesKarla AlanisNo ratings yet
- Approach To Reticulate Hyperpigmentation: Clinical Dermatology - Review ArticleDocument8 pagesApproach To Reticulate Hyperpigmentation: Clinical Dermatology - Review ArticledelfiaNo ratings yet
- Materi 1 - Lesi Putih Keratotik, Lesi Praganas Dan GanasDocument76 pagesMateri 1 - Lesi Putih Keratotik, Lesi Praganas Dan Ganasabdul robby farhanNo ratings yet
- Scleroderma - Oral Manifestations and Treatment ChallengesDocument5 pagesScleroderma - Oral Manifestations and Treatment ChallengesLujainNo ratings yet
- Primer: PodocytopathiesDocument24 pagesPrimer: PodocytopathiesMohamad IrwanNo ratings yet
- Lichen Planus/lupus Erythematosus Overlap With Hypothyroidism: A Case ReportDocument3 pagesLichen Planus/lupus Erythematosus Overlap With Hypothyroidism: A Case ReportcuribepNo ratings yet
- Seminars in Diagnostic Pathology: Mark R. WickDocument12 pagesSeminars in Diagnostic Pathology: Mark R. WickNancy ManriqueNo ratings yet
- Inflammatory DermatosesDocument16 pagesInflammatory DermatosesArlen ElisaNo ratings yet
- Ophthalmia neonatorumIIDocument29 pagesOphthalmia neonatorumIIgopscharanNo ratings yet
- Trading To Win - Bryce GilmoreDocument347 pagesTrading To Win - Bryce GilmoreLeszek100% (15)
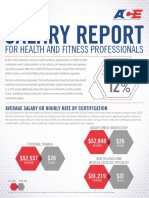
- Salary Report: For Health and Fitness ProfessionalsDocument4 pagesSalary Report: For Health and Fitness ProfessionalsAbhishaik SinghNo ratings yet
- Natal Chart (Data Sheets) : Jul - Day 2447027.611755 TDT, T 55.6 SecDocument2 pagesNatal Chart (Data Sheets) : Jul - Day 2447027.611755 TDT, T 55.6 SecAbhishaik SinghNo ratings yet
- 070 Astangata-AstaDocument20 pages070 Astangata-Astamanojvarrier100% (1)
- Travel PDFDocument1 pageTravel PDFAbhishaik SinghNo ratings yet
- Unilateral Aspects in Vedic AstrologyDocument8 pagesUnilateral Aspects in Vedic AstrologyPalash Roy ChoudhuryNo ratings yet
- Mathematics of AstrologyDocument37 pagesMathematics of Astrologyxkaliberlord100% (15)
- Vedic Astrology and Rasi CharacteristicsDocument60 pagesVedic Astrology and Rasi Characteristicssashikanta96% (47)
- TravelDocument1 pageTravelAbhishaik SinghNo ratings yet
- Pertussis Whooping Cough Letter To ParentsDocument1 pagePertussis Whooping Cough Letter To ParentsPiper Garner RiddleNo ratings yet
- Current Status and Perspective of CAR-T and CAR-NK Cell Therapy Trials in GermanyDocument15 pagesCurrent Status and Perspective of CAR-T and CAR-NK Cell Therapy Trials in GermanyCarlos Meza HernandezNo ratings yet
- Edukasi Perilaku Hidup Sehat Dan Bersih Sebagai Upaya Pencegahan Penularan Virus Covid-19Document18 pagesEdukasi Perilaku Hidup Sehat Dan Bersih Sebagai Upaya Pencegahan Penularan Virus Covid-19Kriz AdinataNo ratings yet
- r142426000 Axel Bolanos CUR142426000Document1 pager142426000 Axel Bolanos CUR142426000Axel BolanosNo ratings yet
- MRSA in Septic ArthritisDocument2 pagesMRSA in Septic ArthritisAmira AlmutairiNo ratings yet
- Concept Map of CellulitisDocument8 pagesConcept Map of CellulitisReese Anne100% (1)
- Handouts CD Prof. RojasDocument6 pagesHandouts CD Prof. RojasChallen CulturaNo ratings yet
- Tuberculosis Thesis TopicsDocument7 pagesTuberculosis Thesis Topicsstacyjohnsonreno100% (2)
- Proceedings of The Southern European Veterinary Conference and Congreso Nacional AVEPADocument9 pagesProceedings of The Southern European Veterinary Conference and Congreso Nacional AVEPAJaviera Paz Rojas ÁlvarezNo ratings yet
- Adult Schedule Easy ReadDocument2 pagesAdult Schedule Easy Read12345zolyNo ratings yet
- Certificate For COVID-19 Vaccination: Beneficiary DetailsDocument1 pageCertificate For COVID-19 Vaccination: Beneficiary DetailsDipak GuptaNo ratings yet
- Chapter 13 Neoplastic Proliferations of White CellsDocument16 pagesChapter 13 Neoplastic Proliferations of White CellsOmar100% (1)
- Narrative Report: Polio Outbreak Response Immunization Bopv Round 2Document4 pagesNarrative Report: Polio Outbreak Response Immunization Bopv Round 2Cristina MelloriaNo ratings yet
- Gape WormDocument4 pagesGape WormNjoku IykeNo ratings yet
- Title Paragraph One:: Sample Five-Paragraph Essay Subject: Should Parents Have Their Children Vaccinated?Document1 pageTitle Paragraph One:: Sample Five-Paragraph Essay Subject: Should Parents Have Their Children Vaccinated?frozenglxNo ratings yet
- Blood Transfusion - Marino - The Icu BookDocument3 pagesBlood Transfusion - Marino - The Icu BookWilliam OmarNo ratings yet
- Arboviral InfectionsDocument15 pagesArboviral InfectionsPatriceNo ratings yet
- General Characteristics and Classification of The Picornavirus Family, Distribution in NatureDocument13 pagesGeneral Characteristics and Classification of The Picornavirus Family, Distribution in NatureSalma Mohamed RezkNo ratings yet
- Questions About Children's Flu VaccinationDocument2 pagesQuestions About Children's Flu VaccinationANNANo ratings yet
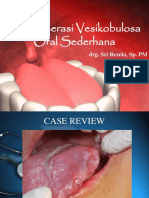
- Ulserasi Vesikobulosa Sederhana-Blok 11 FK 3Document229 pagesUlserasi Vesikobulosa Sederhana-Blok 11 FK 3sitiumaiyahNo ratings yet
- Rheumatic FeverDocument21 pagesRheumatic FeverUmar Azlan50% (2)
- ReferatDocument31 pagesReferatrobby_94No ratings yet
- Microbiology Specimen Collection and TransportDocument1 pageMicrobiology Specimen Collection and TransportUmesha LakshmiNo ratings yet
- ReportDocument1 pageReportAdil ArifNo ratings yet
- Impetigo: Referat Makassar - 2016Document19 pagesImpetigo: Referat Makassar - 2016keluargacendanaNo ratings yet
- Nursing Care PlanDocument3 pagesNursing Care PlanAnnahNo ratings yet
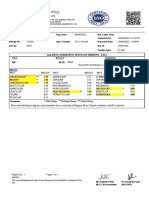
- Allergy Screening Tests (By Immuno - Eia)Document1 pageAllergy Screening Tests (By Immuno - Eia)Patel DhruviNo ratings yet
- 2023 Article 454Document14 pages2023 Article 454bilou hertNo ratings yet
- Drug Study - AmoxicillinDocument2 pagesDrug Study - AmoxicillinVANESSA PAULA ALGADORNo ratings yet
- LeishmaniasisDocument77 pagesLeishmaniasisjaveria choudharyNo ratings yet