You might also like
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5813)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Emergency Medical Responder - First On Scene (PDFDrive)Document656 pagesEmergency Medical Responder - First On Scene (PDFDrive)Diego Armando Castro100% (4)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Sickle Cell AnemiaDocument37 pagesSickle Cell Anemiahazelposis75% (4)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Medical Abbreviations GlossaryDocument15 pagesMedical Abbreviations Glossarydbryant0101100% (9)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Adult Advanced Life SupportDocument14 pagesAdult Advanced Life SupportAnonymous TT7aEIjhuhNo ratings yet
- Pediatric Hospital Care Ethiopia - 2016Document526 pagesPediatric Hospital Care Ethiopia - 2016Tony Tefera100% (5)
- Illu Ababor MatuuDocument46 pagesIllu Ababor MatuuTesfaye DegefaNo ratings yet
- Acls Version B QuizDocument9 pagesAcls Version B QuizRokunuz Jahan Rudro0% (1)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- Prehospital Anesthesia HandbookDocument46 pagesPrehospital Anesthesia HandbookoscarNo ratings yet
- PDF - VeinsDocument3 pagesPDF - VeinsjulialeoNo ratings yet
- PDF - VeinsDocument3 pagesPDF - VeinsjulialeoNo ratings yet
- Description of Equipment MIN Unit Cost Total Cost X - Ray: Medical Equipment List For Typical District HospitalDocument60 pagesDescription of Equipment MIN Unit Cost Total Cost X - Ray: Medical Equipment List For Typical District Hospitalramesh100% (1)
- Oxygen TherapyDocument44 pagesOxygen TherapyChhabilal BastolaNo ratings yet
- Oxygen TherapyDocument46 pagesOxygen Therapyoxidalaj100% (4)
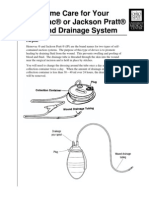
- Jackson PrattDocument7 pagesJackson PrattjulialeoNo ratings yet
- Sickle Cell AnemiaDocument10 pagesSickle Cell AnemiaNader Smadi100% (1)
- NGT InsertionDocument10 pagesNGT Insertionapi-3722454100% (3)
- CPRDocument41 pagesCPRKusumNo ratings yet
- Oxygen Therapy AdministrationDocument15 pagesOxygen Therapy AdministrationMike Faustino Solangon100% (1)
- Neonatal BLSDocument18 pagesNeonatal BLSPatrickNichols0% (1)
- Neonatal ResuscitationDocument16 pagesNeonatal ResuscitationPrecilla C. Stephen100% (3)
- Mechanical Ventilation SeminarDocument82 pagesMechanical Ventilation Seminarrajan kumar91% (22)
- Treatment of Cardiac Arrest in The Hyperbaric Environment - Key Steps On The Sequence of Care - Case ReportsDocument8 pagesTreatment of Cardiac Arrest in The Hyperbaric Environment - Key Steps On The Sequence of Care - Case Reportstonylee24No ratings yet
- SNHD Protocol ManualDocument128 pagesSNHD Protocol ManualMedic03431100% (6)
- Nursing Test Taking SkillsDocument6 pagesNursing Test Taking SkillsNurseStuffNo ratings yet
- Basic Airway ManagementDocument24 pagesBasic Airway ManagementFELIPE MEDINANo ratings yet
- Resuscitation Council (UK)Document18 pagesResuscitation Council (UK)Abdelfattah RashwanNo ratings yet
- Emt Skill SheetsDocument39 pagesEmt Skill SheetsPatriciaChRistiani100% (1)
- TCCC Cls Course Map - 29 Jun 20Document8 pagesTCCC Cls Course Map - 29 Jun 20Giovanni RossiNo ratings yet
- Harriet Lane Handbook 21st Ed 2018-1-200Document200 pagesHarriet Lane Handbook 21st Ed 2018-1-200nguyễn vjNo ratings yet
- Psych NSG Sample QuestionsDocument7 pagesPsych NSG Sample Questionspaul100% (9)
- Vancomycin Dosing and Monitoring in AdultsDocument1 pageVancomycin Dosing and Monitoring in AdultsjulialeoNo ratings yet
- Parsing Nursing NotesDocument28 pagesParsing Nursing NotesjulialeoNo ratings yet
- Article Wound DrainsDocument8 pagesArticle Wound DrainsZeynab AbokarNo ratings yet
- Article Wound DrainsDocument8 pagesArticle Wound DrainsZeynab AbokarNo ratings yet
- US Army Medical Course MD0918-100 - Nursing Care Related To The Gastrointestinal and Urinary SystemsDocument137 pagesUS Army Medical Course MD0918-100 - Nursing Care Related To The Gastrointestinal and Urinary SystemsGeorges100% (1)
- Parsing Nursing NotesDocument28 pagesParsing Nursing NotesjulialeoNo ratings yet
- Review Notes For NCLEX CGFNS - Aortic AneurysmsDocument2 pagesReview Notes For NCLEX CGFNS - Aortic Aneurysmswyndz100% (3)
- Nurse Patient ShipDocument97 pagesNurse Patient Shipcharby12108272100% (2)
- Review Notes For NCLEX CGFNS - Aortic AneurysmsDocument2 pagesReview Notes For NCLEX CGFNS - Aortic Aneurysmswyndz100% (3)
- Triage and Response: Quick LookDocument16 pagesTriage and Response: Quick LookjulialeoNo ratings yet
- Sickle Cell AnemiaDocument23 pagesSickle Cell AnemiaJesmin_36No ratings yet
- Triage and Response: Quick LookDocument16 pagesTriage and Response: Quick LookjulialeoNo ratings yet
- Handbook of MedicationsDocument163 pagesHandbook of MedicationsjulialeoNo ratings yet
- IV ComplicationsDocument76 pagesIV Complicationsmara5140100% (5)
- Oxygenation and Airway Management: Quick LookDocument24 pagesOxygenation and Airway Management: Quick LookNining Komala SariNo ratings yet
- The Urinary SystemDocument66 pagesThe Urinary Systemapi-26587879No ratings yet
- IV ComplicationsDocument76 pagesIV Complicationsmara5140100% (5)
- Airway Assessment and Management ToolsDocument4 pagesAirway Assessment and Management ToolsMudia DwiNo ratings yet
- Hopper Et Al-2018-Frontiers in Veterinary ScienceDocument8 pagesHopper Et Al-2018-Frontiers in Veterinary Sciencecamila uribeNo ratings yet
- Cardiopulmonary RESUSCITATION (CPR) & Critical in Medicine: Dr. Sameer Shaikh M.D. Medicine Asist. Prof. Dept of MedicineDocument84 pagesCardiopulmonary RESUSCITATION (CPR) & Critical in Medicine: Dr. Sameer Shaikh M.D. Medicine Asist. Prof. Dept of MedicineMedicine DepartmentNo ratings yet
- Neonatal Resuscitation Power PointDocument29 pagesNeonatal Resuscitation Power PointsameerarswNo ratings yet
- 9 - ACLS - Part 1Document50 pages9 - ACLS - Part 1Mohnmad ZaitoonNo ratings yet
- Ambu BagDocument12 pagesAmbu BagAejaz Ahmad100% (1)
- Background + RefDocument40 pagesBackground + Refبشير حيدرNo ratings yet
- Simultaneous Breathing and Pulse Check: - Basic Life Support LQDocument4 pagesSimultaneous Breathing and Pulse Check: - Basic Life Support LQDeo Sivan PacificoNo ratings yet
- ACLS Course SyllabusDocument68 pagesACLS Course Syllabusa kNo ratings yet
- Covid 19 Emergency VentilatorDocument46 pagesCovid 19 Emergency VentilatorMahesh KalivarapuNo ratings yet
- Shaun's Guide To Basic NRP: Equipment CheckDocument7 pagesShaun's Guide To Basic NRP: Equipment CheckLori BeckNo ratings yet