You might also like
- Medical EquipmentDocument3 pagesMedical EquipmentasmaraniNo ratings yet
- Tugas Jenis Obat Pak Polma 2Document29 pagesTugas Jenis Obat Pak Polma 2asmaraniNo ratings yet
- Bab IDocument18 pagesBab IasmaraniNo ratings yet
- Asuhan Keperawatan Pada Klien Dengan Ptca: OlehDocument25 pagesAsuhan Keperawatan Pada Klien Dengan Ptca: OlehasmaraniNo ratings yet
- Asuhan Keperawatan Pada Klien Dengan Ptca: OlehDocument25 pagesAsuhan Keperawatan Pada Klien Dengan Ptca: OlehasmaraniNo ratings yet
- I. Tentang Martha E. Rogers 1.1 Latar Belakang Martha E. RogersDocument6 pagesI. Tentang Martha E. Rogers 1.1 Latar Belakang Martha E. RogersasmaraniNo ratings yet
- COVER RaniDocument1 pageCOVER RaniasmaraniNo ratings yet
- Medical EquipmentDocument3 pagesMedical EquipmentasmaraniNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Hallucinations: Clinical Aspects and Management: Industrial Psychiatry Journal February 2020Document10 pagesHallucinations: Clinical Aspects and Management: Industrial Psychiatry Journal February 2020Nyong FenNo ratings yet
- OBGYN Form 3 Qs SearchableDocument50 pagesOBGYN Form 3 Qs SearchableGrace75% (4)
- Lapp Jan2020Document88 pagesLapp Jan2020Siti RojanahNo ratings yet
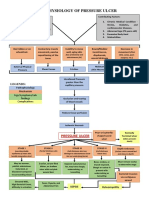
- Pathophysiology of Pressure UlcerDocument1 pagePathophysiology of Pressure UlcerSTORAGE FILENo ratings yet
- SOP Kids Club COVID 19 Measure For GO 2Document2 pagesSOP Kids Club COVID 19 Measure For GO 2adjcdaughtNo ratings yet
- Answers Mock Exam 1Document8 pagesAnswers Mock Exam 1Amin AzadNo ratings yet
- Child Abuse Nursing Care PlansDocument7 pagesChild Abuse Nursing Care PlansMAHESH KOUJALAGINo ratings yet
- Cefuroxime, Celecoxib, ChloridineDocument2 pagesCefuroxime, Celecoxib, ChloridinekrizzywhizzyNo ratings yet
- Pathology of Common Glomerular Syndromes: DR Purushotham KrishnappaDocument34 pagesPathology of Common Glomerular Syndromes: DR Purushotham KrishnappaTarin IslamNo ratings yet
- Acetylcholine Esterase AntibodyDocument2 pagesAcetylcholine Esterase AntibodySrinivasanNo ratings yet
- Dilated CardiomyopathyDocument23 pagesDilated CardiomyopathyYanna Habib-MangotaraNo ratings yet
- Limping Child: Department of Orthopaedics Afmc, PuneDocument101 pagesLimping Child: Department of Orthopaedics Afmc, Punerithesh ramachandranNo ratings yet
- Pediatrics Question PaperDocument21 pagesPediatrics Question Paperprinceej100% (3)
- Epidemiological and Clinical Features of Pediatric COVID-19: Researcharticle Open AccessDocument7 pagesEpidemiological and Clinical Features of Pediatric COVID-19: Researcharticle Open AccessAditha Fitrina AndianiNo ratings yet
- Manual InternDocument136 pagesManual InternalvinatNo ratings yet
- De Quervains TendonitisDocument2 pagesDe Quervains TendonitisisnainiNo ratings yet
- Kaposi SarcomaDocument11 pagesKaposi Sarcomaedgar mandengNo ratings yet
- TB in Special SituationsDocument49 pagesTB in Special SituationsVipul KumarNo ratings yet
- Journal Reading RPL EditDocument30 pagesJournal Reading RPL EditAnonymous l6Q1ROq2No ratings yet
- CV of BaifengZhang.2023Document3 pagesCV of BaifengZhang.2023Baifeng ZhangNo ratings yet
- Evaluation of Macrocytic AnemiasDocument8 pagesEvaluation of Macrocytic Anemiasmy accountNo ratings yet
- Wellen EcgDocument9 pagesWellen EcgElokNo ratings yet
- 1-4, 2016 qhd1Document205 pages1-4, 2016 qhd1waleed.almusharaf100% (1)
- Learning Area Grade Level Quarter Date: English 9 4Document4 pagesLearning Area Grade Level Quarter Date: English 9 4Kim So-Hyun100% (1)
- Influenza: Flu "Influenza" Definition, Symptoms, Causes, Treatment, PreventionDocument3 pagesInfluenza: Flu "Influenza" Definition, Symptoms, Causes, Treatment, PreventionYusuf Rony LosongNo ratings yet
- Magic Surgery NotesDocument54 pagesMagic Surgery NotesChimwemwe TemboNo ratings yet
- Vigabatrin For IsDocument12 pagesVigabatrin For IsAndrew SantosoNo ratings yet
- Kidney DiseasesDocument93 pagesKidney DiseasesDoreen NNo ratings yet
- Annals of Thyroid ResearchDocument2 pagesAnnals of Thyroid ResearchAustin Publishing GroupNo ratings yet