You might also like
- Kriya Reiki Lesson 4Document6 pagesKriya Reiki Lesson 4shivarnoNo ratings yet
- Introduction To ImmunologyDocument21 pagesIntroduction To Immunologysaeed5220020% (1)
- SpleenDocument69 pagesSpleenprabowoaji12No ratings yet
- Liver DiseasesDocument29 pagesLiver DiseasesRicaneth TaanNo ratings yet
- Abnormal LFTsDocument2 pagesAbnormal LFTsRenu RosyNo ratings yet
- Anti Diabetic DrugsDocument58 pagesAnti Diabetic DrugsDaniel WangNo ratings yet
- Prostaglandin Drugs 1Document19 pagesProstaglandin Drugs 1darkmagicdrakeNo ratings yet
- HypertensionDocument85 pagesHypertensionmelkamu AssefaNo ratings yet
- Philippines: Food Product and Safety RegulationDocument24 pagesPhilippines: Food Product and Safety RegulationCelrose FernandezNo ratings yet
- 02 HemoglobinDocument78 pages02 HemoglobinpixiedustNo ratings yet
- Ultimate MJDF Part 1Document89 pagesUltimate MJDF Part 1SueChen Tan75% (4)
- Atherosclerosis PresentationDocument90 pagesAtherosclerosis PresentationAbu SaifNo ratings yet
- AnticancerDocument27 pagesAnticancerLoreine Jane ClaritoNo ratings yet
- 11444.muscle Injuries in Sport Medicine by Gian Nicola BisciottiDocument331 pages11444.muscle Injuries in Sport Medicine by Gian Nicola BisciottiPaisan Ngerndee100% (1)
- Pancreatic Hormone & Antidiabetic Drugs: Renato I. Dalmacio, RPH Pharmacology 414 College of PharmacyDocument69 pagesPancreatic Hormone & Antidiabetic Drugs: Renato I. Dalmacio, RPH Pharmacology 414 College of PharmacyRalf EmoteroNo ratings yet
- Thyroid Disease: Presentation By: Pimundu Vicent Audo Ritah Tutor: Dr. Fualal JaneDocument41 pagesThyroid Disease: Presentation By: Pimundu Vicent Audo Ritah Tutor: Dr. Fualal JaneEsther AumaNo ratings yet
- Pathology of SpleenDocument23 pagesPathology of SpleenKaarthigan RamaiahNo ratings yet
- Adjuvant Systemic Therapy in EarlyDocument3 pagesAdjuvant Systemic Therapy in EarlyGem BulaongNo ratings yet
- Hemoglobin: Hemoglobin Is The Protein Molecule in Red Blood CellsDocument21 pagesHemoglobin: Hemoglobin Is The Protein Molecule in Red Blood CellsQasim NaeemNo ratings yet
- Acute PancreatitisDocument46 pagesAcute PancreatitisLew NianNo ratings yet
- The Spleen - A Surgical Perspective: by Col. Abrar Hussain ZaidiDocument43 pagesThe Spleen - A Surgical Perspective: by Col. Abrar Hussain Zaidiabrar_zaidiNo ratings yet
- Palliative EnciesDocument96 pagesPalliative EnciesnandanNo ratings yet
- Lung Cancer Presentation FinalDocument48 pagesLung Cancer Presentation Finalراس زهد ارفنندNo ratings yet
- CEP BPSD Discussion Guide ENG RFCG Updated2019 PDFDocument8 pagesCEP BPSD Discussion Guide ENG RFCG Updated2019 PDFM.DalaniNo ratings yet
- Carbohydrate MetabolismDocument77 pagesCarbohydrate MetabolismdarkmagicdrakeNo ratings yet
- Quiz Ch. 1Document2 pagesQuiz Ch. 1Gema RojasNo ratings yet
- Pancreas As An Endocrine GlandDocument19 pagesPancreas As An Endocrine GlandKadenceFreya-Charisse G PosadasBulintao0% (1)
- NCP of Impaired MobilityDocument3 pagesNCP of Impaired MobilityHazel Cabrera0% (1)
- Understanding BrachytherapyDocument28 pagesUnderstanding Brachytherapyqwertu132No ratings yet
- Pancreas Neoplasms SyllabusDocument55 pagesPancreas Neoplasms SyllabuscuribenNo ratings yet
- Lecture: Adrenal DisordersDocument78 pagesLecture: Adrenal DisordersOchendo KingxNo ratings yet
- PancreasDocument35 pagesPancreasPaskalisNo ratings yet
- Lung CancerDocument118 pagesLung CancerTati MasatiNo ratings yet
- 1 11857 AnatomyDocument5 pages1 11857 Anatomykalyan2k5No ratings yet
- PancreasDocument11 pagesPancreasCheng XinvennNo ratings yet
- Pancreas 2017Document53 pagesPancreas 2017yasrul izadNo ratings yet
- Anatomy SpleenDocument32 pagesAnatomy SpleenBijo K BennyNo ratings yet
- Transport of Oxygen and Carbon DioxideDocument22 pagesTransport of Oxygen and Carbon DioxideAiza AyazNo ratings yet
- Pseudocyst PancreasDocument17 pagesPseudocyst PancreasShashidhara PuttarajNo ratings yet
- Central Nervous System Pharmacology: Elly Nurus SakinahDocument64 pagesCentral Nervous System Pharmacology: Elly Nurus Sakinahkareem92No ratings yet
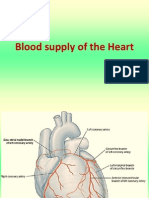
- Blood Supply of HeartDocument7 pagesBlood Supply of Heartmariposa_0612No ratings yet
- Suprarenal (Adrenal) Gland: Dr. R. SanthakumarDocument33 pagesSuprarenal (Adrenal) Gland: Dr. R. SanthakumardrsubanNo ratings yet
- Chronic Kidney DiseaseDocument8 pagesChronic Kidney DiseaseAyiessa_AJNo ratings yet
- Bone and JointDocument43 pagesBone and Jointjheannie02No ratings yet
- Pancreas: Laker Linnet Aimee MBCHB Year 4Document91 pagesPancreas: Laker Linnet Aimee MBCHB Year 4isabellaNo ratings yet
- Breast Pathology Fumc 2022Document145 pagesBreast Pathology Fumc 2022Bahzad AkramNo ratings yet
- Describe The Principles of Blood Cell MaturationDocument11 pagesDescribe The Principles of Blood Cell MaturationnotsoninjaninjaNo ratings yet
- Anti-Parkinsonism Drugs PDFDocument75 pagesAnti-Parkinsonism Drugs PDFSayan NagNo ratings yet
- Lung Cancer and Lung Nodules - An IntroductionDocument5 pagesLung Cancer and Lung Nodules - An Introductionpurushothaman sinivasan100% (1)
- Semester 3 Week 1: Funtion of SpleenDocument2 pagesSemester 3 Week 1: Funtion of SpleenRidzuanNo ratings yet
- Acute Kidney InjuryDocument37 pagesAcute Kidney InjuryLani BuenaventuraNo ratings yet
- Telomere Length The Biological Clock ReviewedDocument3 pagesTelomere Length The Biological Clock ReviewedDavid LaPointNo ratings yet
- 4 Lung-CancerDocument72 pages4 Lung-CancerTaima FayezNo ratings yet
- Types of CancerDocument7 pagesTypes of CancerRegina SABSNo ratings yet
- Liver Function Testing PDFDocument2 pagesLiver Function Testing PDFRajesh KumarNo ratings yet
- The Adrenal GlandsDocument34 pagesThe Adrenal Glandsashgee1No ratings yet
- Pulmonary VentilationDocument35 pagesPulmonary Ventilationnirilib100% (1)
- GastrointestinalDocument104 pagesGastrointestinalNugroho AnisNo ratings yet
- General Principles of Malignant Tumor TreatmentDocument33 pagesGeneral Principles of Malignant Tumor TreatmentТанмай Аасрітх Варма АйенампудіNo ratings yet
- Thyroid CancerDocument39 pagesThyroid CancerFaheem SarwarNo ratings yet
- Pathogenesis of Hashimoto's Thyroiditis (Chronic Autoimmune Thyroiditis) - UpToDateDocument22 pagesPathogenesis of Hashimoto's Thyroiditis (Chronic Autoimmune Thyroiditis) - UpToDaterazvanNo ratings yet
- Colon CancerDocument7 pagesColon CancerKen Ancheta LagayadaNo ratings yet
- MEN1 PPDocument15 pagesMEN1 PPAaron D. PhoenixNo ratings yet
- Endocrine - PancreasDocument39 pagesEndocrine - PancreasAaron D. PhoenixNo ratings yet
- Antibiotic Resistant Bacteria in Eco-EnvironmentDocument33 pagesAntibiotic Resistant Bacteria in Eco-Environmentkedar karkiNo ratings yet
- HDL Classification SlidesDocument20 pagesHDL Classification SlidesRainolNo ratings yet
- Liver Function TestDocument40 pagesLiver Function TestanojNo ratings yet
- Hereditary Spherocytosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHereditary Spherocytosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Bayesian Calculation Application To Medical Genetics: Dr. Larsen Session Id LarsenDocument23 pagesBayesian Calculation Application To Medical Genetics: Dr. Larsen Session Id LarsendarkmagicdrakeNo ratings yet
- Nutritional DiabeteesDocument22 pagesNutritional DiabeteesdarkmagicdrakeNo ratings yet
- Sites of Hormone ProductionDocument2 pagesSites of Hormone ProductiondarkmagicdrakeNo ratings yet
- Gene Expression 2 Regulation: Slide 1Document20 pagesGene Expression 2 Regulation: Slide 1darkmagicdrakeNo ratings yet
- Question 1hDocument3 pagesQuestion 1hItharshan IndreswaranNo ratings yet
- Nursing Case of AmalieDocument5 pagesNursing Case of AmalieRamah MisikoNo ratings yet
- The Role of Yoga in Stress ManagementDocument30 pagesThe Role of Yoga in Stress ManagementKhabirul Alam0% (1)
- Pamplet - English PDFDocument4 pagesPamplet - English PDF9884288233100% (1)
- QUIZ 2 in M.A.P.E.H. 9 Physical Education and Health: Al Dura International SchoolDocument3 pagesQUIZ 2 in M.A.P.E.H. 9 Physical Education and Health: Al Dura International SchoolJhen MendozaNo ratings yet
- Rabicip I V PDFDocument51 pagesRabicip I V PDFdhananjayNo ratings yet
- Algorithms For IV Fluid Therapy in Children and Young People in Hospital Iv Fluid Therapy in ChildrenDocument12 pagesAlgorithms For IV Fluid Therapy in Children and Young People in Hospital Iv Fluid Therapy in ChildrenSREEDEVI T SURESH0% (1)
- 04 - Marile Taine Ale Pamantului RomanescDocument116 pages04 - Marile Taine Ale Pamantului RomanescCorina VavaNo ratings yet
- Perianal Surgical Conditions: Fitsum ArgawDocument51 pagesPerianal Surgical Conditions: Fitsum ArgawWorku KifleNo ratings yet
- MobilityDocument46 pagesMobilityDipen SoniNo ratings yet
- Mid Term Examination Papaer PEDSDocument15 pagesMid Term Examination Papaer PEDSHaslinNo ratings yet
- Special Circumstances Guidelines ALSDocument19 pagesSpecial Circumstances Guidelines ALSHamzaMasoodNo ratings yet
- Powerbuilding 101 Biceps Triceps Explosive Arm GrowthDocument3 pagesPowerbuilding 101 Biceps Triceps Explosive Arm GrowthDeepesh SoniNo ratings yet
- Psychiatric Drug Book - 1Document204 pagesPsychiatric Drug Book - 1Anushri ManeNo ratings yet
- Nursing Care in Plastic SurgeryDocument36 pagesNursing Care in Plastic Surgeryjengyee7186No ratings yet
- Post-Operative Instructions: Hip Hemiarthroplasty: Wound CareDocument3 pagesPost-Operative Instructions: Hip Hemiarthroplasty: Wound CareAbdullah AzmyNo ratings yet
- TpsaDocument14 pagesTpsawahyuNo ratings yet
- Adherence QuestionnaireDocument8 pagesAdherence QuestionnaireDhila FayaNo ratings yet
- A Solution-Focused Approach To Rational-Emotive Behavior Therapy - Toward A Theoretical IntegrationDocument22 pagesA Solution-Focused Approach To Rational-Emotive Behavior Therapy - Toward A Theoretical Integrationsolutions4familyNo ratings yet
- Ketorolaco PDFDocument8 pagesKetorolaco PDFCristhian Cuentas ObandoNo ratings yet
- Notice: Draft Guidance For Industry: Validation of Growth-Based Rapid Microbiological Methods For Sterility Testing of Cellular and Gene Therapy Products AvailabilityDocument2 pagesNotice: Draft Guidance For Industry: Validation of Growth-Based Rapid Microbiological Methods For Sterility Testing of Cellular and Gene Therapy Products AvailabilityJustia.com100% (4)
- Radiotherapy Physics and Principles of Radiotherapy: Q.P. Code: 801908Document12 pagesRadiotherapy Physics and Principles of Radiotherapy: Q.P. Code: 801908Sandhiya KNo ratings yet
- Dead Space ManagementDocument26 pagesDead Space ManagementIgnasNo ratings yet