You might also like
- Meso Endomorph Workout PlanDocument8 pagesMeso Endomorph Workout Planrtkiyous2947No ratings yet
- Shoulder Impingement RehabilitationDocument3 pagesShoulder Impingement RehabilitationHamzh Sallam100% (2)
- Achilles Tendon Rupture 0Document15 pagesAchilles Tendon Rupture 0Usman JabbarNo ratings yet
- Shoulder Dislocation: Nguyen Phuoc Thanh - MDDocument71 pagesShoulder Dislocation: Nguyen Phuoc Thanh - MDThành NPNo ratings yet
- BP Guidelines Safe Working at Height in Logistics and Allied SectorsDocument24 pagesBP Guidelines Safe Working at Height in Logistics and Allied Sectorsnqh2009No ratings yet
- 16 PDFDocument23 pages16 PDFSunilkumar ReddyNo ratings yet
- Shoulder Range of Motion Exercises PDFDocument4 pagesShoulder Range of Motion Exercises PDFGade JyNo ratings yet
- Home Instruct Reverse Total ShoulderDocument7 pagesHome Instruct Reverse Total Shoulderrahul89No ratings yet
- Postnatal Exercises and Advice PDFDocument16 pagesPostnatal Exercises and Advice PDFARCHANA SNo ratings yet
- ACL Reconstruction Rehabilitation ProtocolDocument11 pagesACL Reconstruction Rehabilitation ProtocolNijin XmxNo ratings yet
- Unlocked GuideDocument18 pagesUnlocked Guideveronikabutorina91No ratings yet
- As Exercise Sheet Final PDFDocument4 pagesAs Exercise Sheet Final PDFGopi Krishnan100% (1)
- Medical EmergenciesDocument38 pagesMedical EmergenciesTaleb Redha100% (1)
- Warm Up: Wrist PrepDocument2 pagesWarm Up: Wrist PrephatemfaroukNo ratings yet
- Generic Shoulder Physiotherapy Exercises Sheet: Information For Patients Orthopaedic Shoulder ServiceDocument16 pagesGeneric Shoulder Physiotherapy Exercises Sheet: Information For Patients Orthopaedic Shoulder ServiceBence KlusóczkiNo ratings yet
- Basic and Special Suturing Techniques in Surgery. Honlap 2Document57 pagesBasic and Special Suturing Techniques in Surgery. Honlap 2Arif Nurhidayat PrawirohardjoNo ratings yet
- 2007 Honda Civic Hatchback Owners Manual (Australian, Type R)Document509 pages2007 Honda Civic Hatchback Owners Manual (Australian, Type R)pblazevski_1100% (3)
- MFA - Course Outline and Training SyllabusDocument4 pagesMFA - Course Outline and Training SyllabusFaizal ENRANo ratings yet
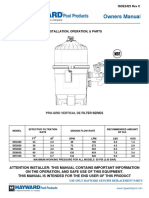
- Manual3620 Pro-Grid DE Filter HaywardDocument12 pagesManual3620 Pro-Grid DE Filter HaywardAries Roxas Enriquez AntonioNo ratings yet
- AC Dislocation RehabDocument8 pagesAC Dislocation Rehabandrea.miruna1999No ratings yet
- E3 - Tennis Elbow OPDocument3 pagesE3 - Tennis Elbow OPAnonymous qX3Ktq6No ratings yet
- Your Functional Rehabilitation After Breast Surgery PDFDocument21 pagesYour Functional Rehabilitation After Breast Surgery PDFTsz Kwan CheungNo ratings yet
- 6857 1 Clavicle Open Reduction Internal Fixation ORIF Physiotherapy AdviceDocument7 pages6857 1 Clavicle Open Reduction Internal Fixation ORIF Physiotherapy AdviceJaneNo ratings yet
- National Hospital (Shoulder-Arthroplasty Rehab-Protocol)Document14 pagesNational Hospital (Shoulder-Arthroplasty Rehab-Protocol)muhammad umarNo ratings yet
- Spread To The Surrounding Tissues in The Breast or Other Parts of The BodyDocument6 pagesSpread To The Surrounding Tissues in The Breast or Other Parts of The BodyEmJay BalansagNo ratings yet
- Total-Shoulder ExercicesDocument9 pagesTotal-Shoulder ExercicesAmalia MihaiNo ratings yet
- Post SPINAL - FUSION GuidelinesDocument7 pagesPost SPINAL - FUSION GuidelineskapilphysioNo ratings yet
- Ortho Services Sports Rehab Clavicle Fracture Protocol Non SurgicalDocument17 pagesOrtho Services Sports Rehab Clavicle Fracture Protocol Non SurgicalKattamedhi Krishnachaitanya KumarreddyNo ratings yet
- Acl Post Op ProtocolDocument7 pagesAcl Post Op Protocolashrafhusein7220No ratings yet
- Exercises Following Latarjet Repair Jan22Document4 pagesExercises Following Latarjet Repair Jan22alizzxNo ratings yet
- Your Functional Rehabilitation After Breast SurgeryDocument20 pagesYour Functional Rehabilitation After Breast SurgeryGeorgeKielingNo ratings yet
- E1 - Elbow ArthrosDocument2 pagesE1 - Elbow ArthrosAnonymous nJ5xtHHNo ratings yet
- Exercises After Breast ReconstructionDocument5 pagesExercises After Breast Reconstructioncbh94455ycNo ratings yet
- Post-Operative Activity Guidelines and Exercises: For EveryoneDocument3 pagesPost-Operative Activity Guidelines and Exercises: For EveryonefuntikarNo ratings yet
- Arthroscopic Bankart Repair1Document14 pagesArthroscopic Bankart Repair1Rinkle KateNo ratings yet
- Physio After SurgeryDocument2 pagesPhysio After SurgeryGursangeet KaurNo ratings yet
- Hip Arthroscopy Clinical Practice Guideline: Phase I - Initial ExerciseDocument9 pagesHip Arthroscopy Clinical Practice Guideline: Phase I - Initial ExerciseRibeiro FtNo ratings yet
- Shoulder Pain Patient InformationDocument7 pagesShoulder Pain Patient Informationas asNo ratings yet
- Lumbar Spinal Fusion Exercises - Jan20Document4 pagesLumbar Spinal Fusion Exercises - Jan20TrisnadewiNo ratings yet
- PL 1083.1 Thyroid Surgery Your Recovery JourneyDocument16 pagesPL 1083.1 Thyroid Surgery Your Recovery JourneyPsycheNo ratings yet
- Revision Knee Repl PDF 230512064435 C3ed421cDocument8 pagesRevision Knee Repl PDF 230512064435 C3ed421cXimena RodriguezNo ratings yet
- Hip Lab Ral Tear Post RegenDocument2 pagesHip Lab Ral Tear Post Regenpara275No ratings yet
- TKR PDFDocument6 pagesTKR PDFKaribeños San JavierNo ratings yet
- Fisioterapia en Prótesis de CaderaDocument24 pagesFisioterapia en Prótesis de CaderaGiusePpe MeatzaNo ratings yet
- Treatment Plan 3Document2 pagesTreatment Plan 3api-456594967No ratings yet
- ACL Reconstruction Physiotherapy Advice For PatientsDocument14 pagesACL Reconstruction Physiotherapy Advice For PatientsIftekharul HaqueNo ratings yet
- ACL Postoperative PeriodDocument5 pagesACL Postoperative PeriodMartin Carlo MartinezNo ratings yet
- Dynamic Hip Screw - Apr20Document10 pagesDynamic Hip Screw - Apr20sanjibannathNo ratings yet
- E5 - Ulnar NerveDocument2 pagesE5 - Ulnar NerveAnonymous aeXhh3Ba17No ratings yet
- ACHQC Abdominal Core Surgery Rehabilitation Protocol Patient Guide 6.17.20Document43 pagesACHQC Abdominal Core Surgery Rehabilitation Protocol Patient Guide 6.17.20Brka223No ratings yet
- Posterior Labral RepairDocument5 pagesPosterior Labral Repairvamshi reddyNo ratings yet
- Total Hip ExercisesDocument28 pagesTotal Hip ExercisesJasmine Joy PalayNo ratings yet
- Shoulder Anterior Labral Repair Rehab ProtocolDocument1 pageShoulder Anterior Labral Repair Rehab ProtocoljohariemergencynumberNo ratings yet
- H20 Ant Shoulder ReconDocument6 pagesH20 Ant Shoulder RecontoaldoNo ratings yet
- THR RestrictedDocument25 pagesTHR RestrictedYadareli DothéNo ratings yet
- Reverse Total Shoulder ArthroplastyDocument3 pagesReverse Total Shoulder ArthroplastyTiberiu BondreaNo ratings yet
- Exercise After Breast SurgeryDocument5 pagesExercise After Breast Surgerysohini bhattacharyaNo ratings yet
- To Proceed To Full WB As Tolerated. in Cases of MeniscalDocument3 pagesTo Proceed To Full WB As Tolerated. in Cases of MeniscalHariNo ratings yet
- D M M A: R Ichael C UliffeDocument11 pagesD M M A: R Ichael C UliffeJaime Oso ThompsonNo ratings yet
- Acl Physio ProtocolDocument6 pagesAcl Physio ProtocolAna MorenoNo ratings yet
- Exer Mastectomy LymphDocument9 pagesExer Mastectomy LymphSharada NayakNo ratings yet
- Physiotherapy Advice After Abdominal SurgeryDocument8 pagesPhysiotherapy Advice After Abdominal SurgeryNewbieNo ratings yet
- C Section ProtocolDocument7 pagesC Section ProtocolAsif KhanNo ratings yet
- Frozen Shoulder Rehab Protocol: 0 2 WeeksDocument8 pagesFrozen Shoulder Rehab Protocol: 0 2 WeekspranjalNo ratings yet
- Anterior Shoulder Stabilization Post Op Protocol - Dec2019Document13 pagesAnterior Shoulder Stabilization Post Op Protocol - Dec2019Yh mynameNo ratings yet
- Take Home QuizDocument4 pagesTake Home QuizZgama AbdulrahmanNo ratings yet
- Freeletics Workout PlanDocument5 pagesFreeletics Workout PlanMiguel OrdoñezNo ratings yet
- Latarjet Shoulder ReconstructionDocument2 pagesLatarjet Shoulder Reconstructionmarcelogascon.oNo ratings yet
- Jakarta School of Prosthetics & Orthotics: Upper Limb Prosthetics Course Work Manual 2010Document84 pagesJakarta School of Prosthetics & Orthotics: Upper Limb Prosthetics Course Work Manual 2010Adinda Dinda100% (1)
- ERO600 ManualDocument1 pageERO600 ManualClaudiu Constantin MandaNo ratings yet
- SEAL 600 ManualDocument32 pagesSEAL 600 ManualChrister NormarkNo ratings yet
- Liv 7Document1 pageLiv 7ray72roNo ratings yet
- Torts Digests Sbca Atty SarmientoDocument301 pagesTorts Digests Sbca Atty SarmientoPaola CayabyabNo ratings yet
- MOYA, John Zeus A. (HUMANA Classwork #3 Prelim)Document41 pagesMOYA, John Zeus A. (HUMANA Classwork #3 Prelim)Suez AyomNo ratings yet
- Incomplete Spinal Cord Injury Nursing Care Plan (ACTUAL) Patient's Name: Alvarez, Marcelo Age: 59y.o. Sex: M Address: Bacolod CityDocument6 pagesIncomplete Spinal Cord Injury Nursing Care Plan (ACTUAL) Patient's Name: Alvarez, Marcelo Age: 59y.o. Sex: M Address: Bacolod CityTherese MargaretNo ratings yet
- Chemical Burns Revisited: What Is The Most Appropriate Method of Decontamination?Document3 pagesChemical Burns Revisited: What Is The Most Appropriate Method of Decontamination?AdharaaNo ratings yet
- Law of Torts SOL5B105 Mids QP 2021-22AYDocument2 pagesLaw of Torts SOL5B105 Mids QP 2021-22AYSaketh RockyNo ratings yet
- Basic Concepts of The Musculoskeletal SystemDocument20 pagesBasic Concepts of The Musculoskeletal SystemTedy FriyadiNo ratings yet
- 6 Hazard AvoidanceDocument22 pages6 Hazard AvoidancefirahliyanaNo ratings yet
- Dystocia - Case ReportDocument51 pagesDystocia - Case ReportPaijo SusenoNo ratings yet
- Autopsy Investigation of DEATHDocument11 pagesAutopsy Investigation of DEATHABC2024No ratings yet
- William Gamba Civil LawsuitDocument17 pagesWilliam Gamba Civil LawsuitThe TribuneNo ratings yet
- Conversion Disorder BrochureDocument2 pagesConversion Disorder BrochurerobktfNo ratings yet
- Stage 1 Design Package: Engineering Foundations - Principles and Communication 100Document31 pagesStage 1 Design Package: Engineering Foundations - Principles and Communication 100api-371900353No ratings yet
- NCP MRMDocument2 pagesNCP MRMKhloe Cristel Llanes Torres100% (1)
- B1233 PDFDocument12 pagesB1233 PDFSooraj Kannan, P.V.No ratings yet
- Mod 1.2 Musculoskeletal System UpdatedDocument26 pagesMod 1.2 Musculoskeletal System UpdatedNandhkishoreNo ratings yet
- MedscapeDocument26 pagesMedscapesiti israwatiNo ratings yet
- Question Chapter 12 ThalamusDocument8 pagesQuestion Chapter 12 ThalamusTrang BuiNo ratings yet