You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5807)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (346)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Fanbeam 4.2 Manual Issue 09Document92 pagesFanbeam 4.2 Manual Issue 09Mohamad HapizNo ratings yet
- Calculation Note For Tank Foundation (Recovered)Document8 pagesCalculation Note For Tank Foundation (Recovered)metoo215100% (1)
- Automotive Air Conditioning Training Manual 1Document49 pagesAutomotive Air Conditioning Training Manual 1Intan Risky100% (1)
- Reconditioning of ValvesDocument6 pagesReconditioning of ValvesPaul PhiliphsNo ratings yet
- Rhinoplasty Dissection ManualDocument185 pagesRhinoplasty Dissection ManualVikas Vats100% (3)
- The Design of Vertical Pressure Vessels Subjected To Applied ForcesDocument3 pagesThe Design of Vertical Pressure Vessels Subjected To Applied ForcesMANOJ M100% (1)
- John Kelsey JK QX Conf08 IssueADocument216 pagesJohn Kelsey JK QX Conf08 IssueAnamkay_tenzynNo ratings yet
- Mukhanbetova Nazira Experimental Laborat PDFDocument196 pagesMukhanbetova Nazira Experimental Laborat PDFPankaj RathoreNo ratings yet
- API - RP-571 - Damage Mech. SummaryDocument28 pagesAPI - RP-571 - Damage Mech. SummaryglazetmNo ratings yet
- Generator Erection Manual THW 210 2A 2BDocument213 pagesGenerator Erection Manual THW 210 2A 2Bkrishkar2010100% (1)
- Acute Effects of Radiation InjuryDocument8 pagesAcute Effects of Radiation InjuryVikas VatsNo ratings yet
- Alternative Method For Fabrication of Power ArmDocument2 pagesAlternative Method For Fabrication of Power ArmVikas VatsNo ratings yet
- Facial AnatomyDocument11 pagesFacial AnatomySneha SthaNo ratings yet
- Evoked PotentialDocument6 pagesEvoked PotentialVikas VatsNo ratings yet
- The Anatomical Basis For Surgical Preservation of Temporal MuscleDocument6 pagesThe Anatomical Basis For Surgical Preservation of Temporal Musclekurtwaldhaim22No ratings yet
- Vestibuloplasty With Skin Grafting and Lowering of The-HandoutDocument6 pagesVestibuloplasty With Skin Grafting and Lowering of The-HandoutVikas VatsNo ratings yet
- Pikos-Mandibluar Block Autografts For Alveolar Ridge AugmentationDocument17 pagesPikos-Mandibluar Block Autografts For Alveolar Ridge AugmentationVikas VatsNo ratings yet
- HN 03-2011 Submadibular Salivary Gland Transfer PDFDocument7 pagesHN 03-2011 Submadibular Salivary Gland Transfer PDFVikas VatsNo ratings yet
- BJOMS 2011. Technical Note. Use of Methylene Blue For Precise Peripheral Ostectomy of Keratocystic Odontogenic TumourDocument2 pagesBJOMS 2011. Technical Note. Use of Methylene Blue For Precise Peripheral Ostectomy of Keratocystic Odontogenic TumourVikas Vats100% (1)
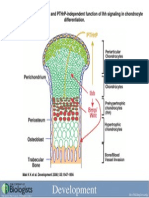
- Development 2008 Jun 135 (11) 1947-56, Fig. 7.Document1 pageDevelopment 2008 Jun 135 (11) 1947-56, Fig. 7.Vikas VatsNo ratings yet
- Computer-Assisted Navigational Surgery in Oral and Maxillofacial SurgeryDocument9 pagesComputer-Assisted Navigational Surgery in Oral and Maxillofacial SurgeryVikas VatsNo ratings yet
- 1545 1569 (2000) 037 0243:amouof 2.3.co 2Document5 pages1545 1569 (2000) 037 0243:amouof 2.3.co 2Vikas VatsNo ratings yet
- JS1020 X P07 1501Document26 pagesJS1020 X P07 1501Anonymous tWOsIcNo ratings yet
- Biofarmasetika BCSDocument19 pagesBiofarmasetika BCSReno SaputraNo ratings yet
- Pahs in Toys and Childcare Products: Survey of Chemical Substances in Consumer Products No. 114 2011Document41 pagesPahs in Toys and Childcare Products: Survey of Chemical Substances in Consumer Products No. 114 2011lthyaguNo ratings yet
- Plate and Frame Filter Press: Instruction ManualDocument8 pagesPlate and Frame Filter Press: Instruction ManualYatharth SahuNo ratings yet
- Blood Bank Refrigerator Technical & Performance Specification CriteriaDocument2 pagesBlood Bank Refrigerator Technical & Performance Specification CriteriaEhsan alwafaaNo ratings yet
- Expt 1 - 2022-2023Document4 pagesExpt 1 - 2022-2023MAYRELL PUN-ANNo ratings yet
- Assignment 3 DmeDocument3 pagesAssignment 3 DmeSubash DgłNo ratings yet
- Chemistry PBLDocument27 pagesChemistry PBLZLLL0930No ratings yet
- Speciality Performance PackingsDocument16 pagesSpeciality Performance Packingsdona_001No ratings yet
- 10 Sumitomo FFCDocument6 pages10 Sumitomo FFCTom Sawyer CruiNo ratings yet
- Commercial Kitchen VentilationDocument59 pagesCommercial Kitchen VentilationSMBEAUTYNo ratings yet
- Bio Transformation of Vanillin From IsoeugenolDocument7 pagesBio Transformation of Vanillin From IsoeugenolcharlesNo ratings yet
- HAZOP Study Part IIDocument18 pagesHAZOP Study Part IIBoy farhanNo ratings yet
- Extract EnglishDocument30 pagesExtract EnglishivanNo ratings yet
- Vitamins A and E by Uplc-Uv or FLD: InstructionsDocument16 pagesVitamins A and E by Uplc-Uv or FLD: InstructionsSreejith SreekumarNo ratings yet
- Fernando C. de Guzman: Contact No.: 09051031714 / 09325773550 E-Mail AddressDocument6 pagesFernando C. de Guzman: Contact No.: 09051031714 / 09325773550 E-Mail AddressGold LeonardoNo ratings yet
- Protein-Protein Interaction and System BiologyDocument14 pagesProtein-Protein Interaction and System Biologyamitbhimani100% (2)
- Bd260678 Gaspak EzDocument6 pagesBd260678 Gaspak Ezhca_120% (1)
- Engineering Materials: by RangwalaDocument5 pagesEngineering Materials: by RangwalabalaNo ratings yet
- EDI FilterDocument6 pagesEDI FiltersuparjoNo ratings yet
- HIT-RE 500 - Long-Term-Behaviour1Document16 pagesHIT-RE 500 - Long-Term-Behaviour1Marco Antonio TeranNo ratings yet