You might also like
- Caring, Curing, Coping: Nurse, Physician, and Patient RelationshipsFrom EverandCaring, Curing, Coping: Nurse, Physician, and Patient RelationshipsNo ratings yet
- Applying The Four Principles of BioEthicsDocument3 pagesApplying The Four Principles of BioEthicsAurelia Pinder100% (1)
- Medical Ethics: A Physician's Guide to Clinical MedicineFrom EverandMedical Ethics: A Physician's Guide to Clinical MedicineNo ratings yet
- 01-EPPT-Course-Unit-2 Ethics and Professionalism in PTDocument13 pages01-EPPT-Course-Unit-2 Ethics and Professionalism in PTMIKEE MEDRANONo ratings yet
- Activity 2Document8 pagesActivity 2Myhen Grace QuebecNo ratings yet
- Principles of Clinical Ethics and Their Application To PracticeDocument12 pagesPrinciples of Clinical Ethics and Their Application To PracticeHarshNo ratings yet
- Obstacles With Ethics in Resuscitation With Several ComorbiditiesDocument12 pagesObstacles With Ethics in Resuscitation With Several ComorbiditiesAbo-ahmed ElmasryNo ratings yet
- Running Head: Applying Ethical Principles 1Document7 pagesRunning Head: Applying Ethical Principles 1Cate siz100% (1)
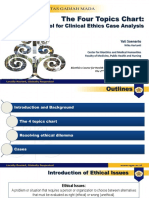
- The Four Topics Chart:: A Tool For Clinical Ethics Case AnalysisDocument25 pagesThe Four Topics Chart:: A Tool For Clinical Ethics Case AnalysisZuzu FinusNo ratings yet
- Papadimos, T. J. (2004) - Stoicism, The Physician, and Care of Medical Outliers.Document7 pagesPapadimos, T. J. (2004) - Stoicism, The Physician, and Care of Medical Outliers.Prof.V. GunaretnamNo ratings yet
- HCE Module 1 - Introduction To Health Care EthicsDocument4 pagesHCE Module 1 - Introduction To Health Care EthicsAlaiza AvergonzadoNo ratings yet
- Ethical Considerations in Emergency Care: Kenneth V. Iserson, MD, MBA, FacepDocument8 pagesEthical Considerations in Emergency Care: Kenneth V. Iserson, MD, MBA, FacepJenry Reyes TrispaNo ratings yet
- Nursing EthicsDocument6 pagesNursing EthicsAliza Bea CastroNo ratings yet
- When Should Conscientious Objection Be Accepted?: Morten MagelssenDocument5 pagesWhen Should Conscientious Objection Be Accepted?: Morten MagelssenFuraya FuisaNo ratings yet
- KD BN Prima Facie 2013Document60 pagesKD BN Prima Facie 2013Aldo HamkaNo ratings yet
- PhilosophyDocument6 pagesPhilosophyjamilasaeed777No ratings yet
- Ethos "A Characteristic Way of Acting".: The Thing Which Action Is Essentially ConcernedDocument2 pagesEthos "A Characteristic Way of Acting".: The Thing Which Action Is Essentially ConcernedCecil Bhang-i Cacay - PabloNo ratings yet
- Notes For ArticleDocument5 pagesNotes For ArticleRamil Andrea BoybantingNo ratings yet
- Chapter 26 Legal and Ethical Issues in Couple TherapyDocument18 pagesChapter 26 Legal and Ethical Issues in Couple TherapyMoises BocanegraNo ratings yet
- Module 5 Ethics OverviewDocument31 pagesModule 5 Ethics OverviewOgie Rose BanasanNo ratings yet
- Beerman 1997Document4 pagesBeerman 1997mariana alvarezNo ratings yet
- Legeal & EthicalDocument6 pagesLegeal & EthicalNaro LemtorNo ratings yet
- The Ethics of Neurologically Complicated PregnanciesDocument16 pagesThe Ethics of Neurologically Complicated PregnanciesmoutranhabibNo ratings yet
- Ethical TheoriesDocument35 pagesEthical TheoriesJenross De LeonNo ratings yet
- Kaidah Dasar Bioetika & Prima FacieDocument60 pagesKaidah Dasar Bioetika & Prima FacieSamdiSutantoNo ratings yet
- Ethical ReasoningDocument3 pagesEthical ReasoningfelamendoNo ratings yet
- ETHICSDocument7 pagesETHICSJani KhanNo ratings yet
- Nur 223 Health Care Ethics (Bioethics)Document42 pagesNur 223 Health Care Ethics (Bioethics)Gemmalene PaclebNo ratings yet
- Professional Practice in Physical TherapyDocument19 pagesProfessional Practice in Physical TherapyRizwan BashirNo ratings yet
- Role of Ethical Principles in Healthcare CodesDocument6 pagesRole of Ethical Principles in Healthcare CodesNewfaceNo ratings yet
- Ethical Dilemmas in Nursing CareDocument50 pagesEthical Dilemmas in Nursing CareZyla De SagunNo ratings yet
- Values and EthicsDocument21 pagesValues and EthicsPaulo Xander Corpin Basa100% (1)
- Clinical Chem Individual AssignmentDocument4 pagesClinical Chem Individual Assignmentcheng eugeneNo ratings yet
- Ethics in MedicineDocument24 pagesEthics in Medicinekavi priyaNo ratings yet
- Executive SummaryDocument9 pagesExecutive SummaryconnieNo ratings yet
- CLinical Ethics and ProfessionalismDocument38 pagesCLinical Ethics and ProfessionalismBerhanuNo ratings yet
- Bioethics DysthanasiaDocument4 pagesBioethics DysthanasiaGerlian Kyle QueridoNo ratings yet
- Social Science & Medicine: Didier FassinDocument9 pagesSocial Science & Medicine: Didier FassinMichelli De Souza RibeiroNo ratings yet
- MedicalEthics PDFDocument25 pagesMedicalEthics PDFmchs_libNo ratings yet
- Ethics Basic Concepts For Professional Nursing PractiDocument44 pagesEthics Basic Concepts For Professional Nursing Practiprema balusamyNo ratings yet
- Legal and Ethical Issues in Couple Therapy: M C. G J L G L. SDocument20 pagesLegal and Ethical Issues in Couple Therapy: M C. G J L G L. SEmiNo ratings yet
- MacKenzie - What Would A Good Doctor Do? Re Ections On The Ethics of MedicineDocument4 pagesMacKenzie - What Would A Good Doctor Do? Re Ections On The Ethics of MedicineCecitorNo ratings yet
- Cardio Ethical Legal IssueDocument56 pagesCardio Ethical Legal IssueDeepika LingamNo ratings yet
- Stoicism, The Physician, and Care of Medical Outliers: BMC Medical Ethics January 2005Document8 pagesStoicism, The Physician, and Care of Medical Outliers: BMC Medical Ethics January 2005mroctavNo ratings yet
- Principles of BioethicsDocument7 pagesPrinciples of BioethicsNuronnisah Kalinggalan PadjiriNo ratings yet
- Ethical Issues in HealthDocument12 pagesEthical Issues in HealthEdwin OtworiNo ratings yet
- Advanced Practice Nursing EthicalDocument5 pagesAdvanced Practice Nursing EthicalNurse PractitionerNo ratings yet
- NLM Sas 7Document13 pagesNLM Sas 7Zzimply Tri Sha UmaliNo ratings yet
- Individuals in Public Health and Health PolicyDocument12 pagesIndividuals in Public Health and Health PolicyMarvin BautistaNo ratings yet
- Ethical PrinciplesDocument2 pagesEthical PrinciplesyoonjessNo ratings yet
- .Trashed-1648312261-American J Hematol - 2001 - Ballas - Ethical Issues in The Management of Sickle Cell PainDocument6 pages.Trashed-1648312261-American J Hematol - 2001 - Ballas - Ethical Issues in The Management of Sickle Cell PainDr. Smiley JadonandanNo ratings yet
- Medical ethics principles and branchesDocument6 pagesMedical ethics principles and branchesdobuol gorNo ratings yet
- 4 Ethical DecisionmakingDocument12 pages4 Ethical DecisionmakingSherry Rose MisaNo ratings yet
- Teori Etika KeperawatanDocument19 pagesTeori Etika Keperawatandwidui93No ratings yet
- Principles of Justice in Health Care RationingDocument7 pagesPrinciples of Justice in Health Care RationingDalene EvangelioNo ratings yet
- The Four Bioethical PrinciplesDocument4 pagesThe Four Bioethical Principlesariansofia1031No ratings yet
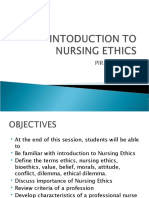
- Intoduction To Nursing EthicsDocument17 pagesIntoduction To Nursing EthicsAnjo Pasiolco CanicosaNo ratings yet
- NCM108 Module 1-CDocument9 pagesNCM108 Module 1-Cmirai desuNo ratings yet
- Patricia Ann Potter - Anne Griffin Perry - Patricia A Stockert - Amy Hall - Fundamentals of Nursing-Elsevier Mosby (2013) - 321-330Document17 pagesPatricia Ann Potter - Anne Griffin Perry - Patricia A Stockert - Amy Hall - Fundamentals of Nursing-Elsevier Mosby (2013) - 321-330Rachma WatiNo ratings yet
- Ethics in MidwiferyDocument12 pagesEthics in MidwiferyRoselineTigga100% (1)
- QlassicDocument64 pagesQlassicchuanhan_tan100% (2)
- Who Icf ModelDocument10 pagesWho Icf ModelXulkanain ZENo ratings yet
- Who Icf ModelDocument10 pagesWho Icf ModelXulkanain ZENo ratings yet
- WCPT - Declaraciones de Politica Fisio 2013Document124 pagesWCPT - Declaraciones de Politica Fisio 2013Hadassah Salinas de FerroNo ratings yet
- QlassicDocument64 pagesQlassicchuanhan_tan100% (2)
- QlassicDocument64 pagesQlassicchuanhan_tan100% (2)
- Chronic Low Back PainDocument14 pagesChronic Low Back PainranggadrNo ratings yet
- Malaysian Dietary Guidelines 2010 - Executive Summary PDFDocument27 pagesMalaysian Dietary Guidelines 2010 - Executive Summary PDFXulkanain ZENo ratings yet
- CRP REVIEW by Physio.30913pptDocument8 pagesCRP REVIEW by Physio.30913pptXulkanain ZENo ratings yet
- NAD407 Principles of Nutrition Nhspf7YDocument8 pagesNAD407 Principles of Nutrition Nhspf7YXulkanain ZENo ratings yet
- Maths SequencesDocument19 pagesMaths SequencesXulkanain ZENo ratings yet
- Management of Gross Motor (PT)Document63 pagesManagement of Gross Motor (PT)Xulkanain ZENo ratings yet
- KNGF Guideline For Physical Therapy Cardiac Rehabilitation FlowchartDocument3 pagesKNGF Guideline For Physical Therapy Cardiac Rehabilitation FlowchartXulkanain ZENo ratings yet
- Font InfoDocument1 pageFont InfoCahyo SnNo ratings yet
- !!! Floral Office Wl700-FillabledDocument1 page!!! Floral Office Wl700-FillabledAnny StolbovaNo ratings yet
- Fracture Neck of HumerusDocument3 pagesFracture Neck of HumerusXulkanain ZENo ratings yet
- Maths SequencesDocument19 pagesMaths SequencesXulkanain ZENo ratings yet
- !!! Floral Office Wl700-FillabledDocument1 page!!! Floral Office Wl700-FillabledAnny StolbovaNo ratings yet
- !!! Chevron WL-875 Multi-FillableDocument1 page!!! Chevron WL-875 Multi-FillableXulkanain ZENo ratings yet
- !!! Quatrefoil WL-5375 Multi-FillableDocument1 page!!! Quatrefoil WL-5375 Multi-FillableXulkanain ZENo ratings yet
- Assessment of PostureDocument18 pagesAssessment of PostureKanika SinhaNo ratings yet
- 7 Physiotherapy in PeriodontologyDocument31 pages7 Physiotherapy in PeriodontologyXulkanain ZE100% (1)
- JCPT Acute LBP BrochureDocument2 pagesJCPT Acute LBP BrochureXulkanain ZENo ratings yet
- Frenkel's ExerciseDocument2 pagesFrenkel's ExerciseAnusha AppajiNo ratings yet
- Quebec Back PainDocument1 pageQuebec Back PainXulkanain ZENo ratings yet
- Physiotherapy: Michael Hegarty Miscp MCSP BSC Chartered Physiotherapist Pgdip Sports & Exercise MedicineDocument18 pagesPhysiotherapy: Michael Hegarty Miscp MCSP BSC Chartered Physiotherapist Pgdip Sports & Exercise MedicineXulkanain ZENo ratings yet
- Cranial Nerve Assesssment1Document6 pagesCranial Nerve Assesssment1Xulkanain ZENo ratings yet
- Therac-25 Medical Accelerator Case StudyDocument34 pagesTherac-25 Medical Accelerator Case StudyAkramJKhezrejiNo ratings yet
- VIDEO Game Addiction MP PresentationDocument19 pagesVIDEO Game Addiction MP PresentationPredrag MiloicaNo ratings yet
- Personal Training AgreementDocument8 pagesPersonal Training AgreementWes Geary100% (3)
- 10 - Occupational Stress Reflections On Theory and PracticeDocument15 pages10 - Occupational Stress Reflections On Theory and PracticeCatedra PsihologieNo ratings yet
- DC Healthy People ReportDocument108 pagesDC Healthy People ReportChristina SturdivantNo ratings yet
- Active Release TechniquesDocument15 pagesActive Release TechniquesPhysiotherapist Ali100% (1)
- SJDS 412562 572Document11 pagesSJDS 412562 572habeebNo ratings yet
- Know Your Magnetic FieldDocument75 pagesKnow Your Magnetic FieldAtma Jnani100% (5)
- Sickle Cell Anemia 2007Document25 pagesSickle Cell Anemia 2007R-o-N-n-e-lNo ratings yet
- Ocular InjuryDocument46 pagesOcular InjurysnyNo ratings yet
- Dreams as a Portal to Inner Wisdom: A Guide to Clinical Dream InterpretationDocument16 pagesDreams as a Portal to Inner Wisdom: A Guide to Clinical Dream InterpretationLeslie Rodriguez FranciscoNo ratings yet
- Receptor Binding Profiles of AntipsychoticsDocument1 pageReceptor Binding Profiles of AntipsychoticsM.Dalani100% (3)
- Pemphigus vulgarisPPTDocument23 pagesPemphigus vulgarisPPTSiti HanisaNo ratings yet
- Spinal Orthoses: Type Examples Motion Restriction Indications NotesDocument2 pagesSpinal Orthoses: Type Examples Motion Restriction Indications NotesBD BesorioNo ratings yet
- Analysis of Cough and Analgesic Range of Pharmaceutical Active Ingredients Using RP-HPLC MethodDocument14 pagesAnalysis of Cough and Analgesic Range of Pharmaceutical Active Ingredients Using RP-HPLC MethodDr. Varaprasad Bobbarala0% (1)
- Encircle The Best Answer: C) Health Means Not Seeing A DoctorDocument7 pagesEncircle The Best Answer: C) Health Means Not Seeing A DoctorMuhammad Usman KhanNo ratings yet
- Presby Methotrexate Protocol For Ectopic PregnancyDocument3 pagesPresby Methotrexate Protocol For Ectopic PregnancyTrina JoyceNo ratings yet
- Anger ManagementDocument4 pagesAnger ManagementAmron Azman100% (1)
- BooksDocument13 pagesBooksDoru Vrajitoru0% (1)
- 31 Premature EjaculationDocument4 pages31 Premature EjaculationWàrìs Ràfìqùé ßàlòçhNo ratings yet
- Maternal Newborn AtiDocument4 pagesMaternal Newborn Atiapi-243590841100% (3)
- AuriculotherapyDocument7 pagesAuriculotherapy4gen_7No ratings yet
- AMTA Covered Modalities ListDocument8 pagesAMTA Covered Modalities Listbackch9011No ratings yet
- Dialysis Inspection Tool 2014Document11 pagesDialysis Inspection Tool 2014Maek100% (1)
- Cashew Apple Report FinalDocument138 pagesCashew Apple Report FinalAbhijeet Singh50% (2)
- Failure in FpsDocument7 pagesFailure in FpsbabukanchaNo ratings yet
- Case Study OBDocument19 pagesCase Study OBLele Alwayzthesame KearneyNo ratings yet
- International Conference Photodynamic Therapy and Medical Laser Applications Milan, 24th-27th June, 1 992Document143 pagesInternational Conference Photodynamic Therapy and Medical Laser Applications Milan, 24th-27th June, 1 992Max SinghNo ratings yet
- Resume March2023Document2 pagesResume March2023api-625227498No ratings yet
- Question Paper Unit A161 02 Modules b1 b2 b3 Higher TierDocument16 pagesQuestion Paper Unit A161 02 Modules b1 b2 b3 Higher TierAnonymous QFkCS837bNo ratings yet
- Transformed: Moving to the Product Operating ModelFrom EverandTransformed: Moving to the Product Operating ModelRating: 4 out of 5 stars4/5 (1)
- The Coaching Habit: Say Less, Ask More & Change the Way You Lead ForeverFrom EverandThe Coaching Habit: Say Less, Ask More & Change the Way You Lead ForeverRating: 4.5 out of 5 stars4.5/5 (186)
- Transformed: Moving to the Product Operating ModelFrom EverandTransformed: Moving to the Product Operating ModelRating: 4 out of 5 stars4/5 (1)
- How to Talk to Anyone at Work: 72 Little Tricks for Big Success Communicating on the JobFrom EverandHow to Talk to Anyone at Work: 72 Little Tricks for Big Success Communicating on the JobRating: 4.5 out of 5 stars4.5/5 (36)
- How the World Sees You: Discover Your Highest Value Through the Science of FascinationFrom EverandHow the World Sees You: Discover Your Highest Value Through the Science of FascinationRating: 4 out of 5 stars4/5 (7)
- The Introverted Leader: Building on Your Quiet StrengthFrom EverandThe Introverted Leader: Building on Your Quiet StrengthRating: 4.5 out of 5 stars4.5/5 (35)
- The First Minute: How to start conversations that get resultsFrom EverandThe First Minute: How to start conversations that get resultsRating: 4.5 out of 5 stars4.5/5 (55)
- The 7 Habits of Highly Effective PeopleFrom EverandThe 7 Habits of Highly Effective PeopleRating: 4 out of 5 stars4/5 (2564)
- Billion Dollar Lessons: What You Can Learn from the Most Inexcusable Business Failures of the Last Twenty-five YearsFrom EverandBillion Dollar Lessons: What You Can Learn from the Most Inexcusable Business Failures of the Last Twenty-five YearsRating: 4.5 out of 5 stars4.5/5 (52)
- Scaling Up: How a Few Companies Make It...and Why the Rest Don't, Rockefeller Habits 2.0From EverandScaling Up: How a Few Companies Make It...and Why the Rest Don't, Rockefeller Habits 2.0Rating: 5 out of 5 stars5/5 (1)
- The 4 Disciplines of Execution: Revised and Updated: Achieving Your Wildly Important GoalsFrom EverandThe 4 Disciplines of Execution: Revised and Updated: Achieving Your Wildly Important GoalsRating: 4.5 out of 5 stars4.5/5 (48)
- Spark: How to Lead Yourself and Others to Greater SuccessFrom EverandSpark: How to Lead Yourself and Others to Greater SuccessRating: 4.5 out of 5 stars4.5/5 (130)
- Work Stronger: Habits for More Energy, Less Stress, and Higher Performance at WorkFrom EverandWork Stronger: Habits for More Energy, Less Stress, and Higher Performance at WorkRating: 4.5 out of 5 stars4.5/5 (12)
- Sustainability Management: Global Perspectives on Concepts, Instruments, and StakeholdersFrom EverandSustainability Management: Global Perspectives on Concepts, Instruments, and StakeholdersRating: 5 out of 5 stars5/5 (1)
- The 12 Week Year: Get More Done in 12 Weeks than Others Do in 12 MonthsFrom EverandThe 12 Week Year: Get More Done in 12 Weeks than Others Do in 12 MonthsRating: 4.5 out of 5 stars4.5/5 (411)
- 7 Principles of Transformational Leadership: Create a Mindset of Passion, Innovation, and GrowthFrom Everand7 Principles of Transformational Leadership: Create a Mindset of Passion, Innovation, and GrowthRating: 5 out of 5 stars5/5 (51)
- The Power of People Skills: How to Eliminate 90% of Your HR Problems and Dramatically Increase Team and Company Morale and PerformanceFrom EverandThe Power of People Skills: How to Eliminate 90% of Your HR Problems and Dramatically Increase Team and Company Morale and PerformanceRating: 5 out of 5 stars5/5 (22)
- Leadership Skills that Inspire Incredible ResultsFrom EverandLeadership Skills that Inspire Incredible ResultsRating: 4.5 out of 5 stars4.5/5 (11)
- The 7 Habits of Highly Effective People: 30th Anniversary EditionFrom EverandThe 7 Habits of Highly Effective People: 30th Anniversary EditionRating: 5 out of 5 stars5/5 (336)
- Unlocking Potential: 7 Coaching Skills That Transform Individuals, Teams, & OrganizationsFrom EverandUnlocking Potential: 7 Coaching Skills That Transform Individuals, Teams, & OrganizationsRating: 4.5 out of 5 stars4.5/5 (27)
- Summary: Choose Your Enemies Wisely: Business Planning for the Audacious Few: Key Takeaways, Summary and AnalysisFrom EverandSummary: Choose Your Enemies Wisely: Business Planning for the Audacious Few: Key Takeaways, Summary and AnalysisRating: 4.5 out of 5 stars4.5/5 (3)
- How to Lead: Wisdom from the World's Greatest CEOs, Founders, and Game ChangersFrom EverandHow to Lead: Wisdom from the World's Greatest CEOs, Founders, and Game ChangersRating: 4.5 out of 5 stars4.5/5 (95)
- Get Scalable: The Operating System Your Business Needs To Run and Scale Without YouFrom EverandGet Scalable: The Operating System Your Business Needs To Run and Scale Without YouRating: 5 out of 5 stars5/5 (1)
- Good to Great by Jim Collins - Book Summary: Why Some Companies Make the Leap...And Others Don'tFrom EverandGood to Great by Jim Collins - Book Summary: Why Some Companies Make the Leap...And Others Don'tRating: 4.5 out of 5 stars4.5/5 (63)