You might also like
- Folio EleveDocument20 pagesFolio Elevelorenzacazzato9No ratings yet
- Les Fractures MandibulairesDocument6 pagesLes Fractures Mandibulairesadelmiringui2No ratings yet
- Physiopathologie de L Éruption DentaireDocument9 pagesPhysiopathologie de L Éruption DentaireMOMONo ratings yet
- Tumeurs Osseuses Primitives: ECN N°304Document6 pagesTumeurs Osseuses Primitives: ECN N°304Simionescu AlinNo ratings yet
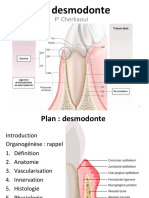
- Desmodonte ÉtudiantsDocument42 pagesDesmodonte ÉtudiantsMossabRamboukNo ratings yet
- Généralités Sur Les FracturesDocument5 pagesGénéralités Sur Les Fracturesrayanou2004.ahNo ratings yet
- 02 Phenomene de CroissanceDocument7 pages02 Phenomene de CroissanceImoona iiNo ratings yet
- Le Mobile FoetalDocument44 pagesLe Mobile FoetalBlaack LotusNo ratings yet
- CancérologieDocument20 pagesCancérologieAbdou RahmouniNo ratings yet
- Les Atteintes Musculo-Squelettiques Dans L'hémophilie JFR 2023Document36 pagesLes Atteintes Musculo-Squelettiques Dans L'hémophilie JFR 2023Stella Di MareNo ratings yet
- TD O4. Incisions Sutures 16.11.15 (Mode de Compatibilité)Document54 pagesTD O4. Incisions Sutures 16.11.15 (Mode de Compatibilité)Sosakkada100% (1)
- Membrane Induite PDFDocument49 pagesMembrane Induite PDFJean PatateNo ratings yet
- La Radiographie ConventionnelleDocument3 pagesLa Radiographie ConventionnellemerymorenaaNo ratings yet
- Age Osseux Etmaturation Osseuse A Envoyer 8-2-2023 PDFDocument48 pagesAge Osseux Etmaturation Osseuse A Envoyer 8-2-2023 PDFDavida glenne MamboundouNo ratings yet
- Cours Tumeurs OsseusesDocument22 pagesCours Tumeurs OsseusesBarinaNo ratings yet
- Tumeurs Osseusses BénignesDocument100 pagesTumeurs Osseusses BénignesAtte Marie Frederic ArraNo ratings yet
- Biomecanique 20articulaire 20GV 20 PDFDocument72 pagesBiomecanique 20articulaire 20GV 20 PDFSimo AsterNo ratings yet
- Anat DescDocument53 pagesAnat Descdahbyamine37No ratings yet
- Lexique Dentaire DR Albert Hauteville PDDocument30 pagesLexique Dentaire DR Albert Hauteville PDAsma Sama100% (1)
- Vol 4 No 4Document68 pagesVol 4 No 4Ho DaNo ratings yet
- Embryologie Face & Cavité Buccale 2Document17 pagesEmbryologie Face & Cavité Buccale 2Yo YaNo ratings yet
- Citadelle Des Cours Théoriques en EPSDocument120 pagesCitadelle Des Cours Théoriques en EPSINDRAP MENNo ratings yet
- Metastases Osseuses - Metastases VertebralesDocument20 pagesMetastases Osseuses - Metastases Vertebralesbensaadaidir14No ratings yet
- These Modèles D'endommagement Et de Rupture Des Matériaux BiologiquesDocument251 pagesThese Modèles D'endommagement Et de Rupture Des Matériaux BiologiquesFrederic WustNo ratings yet
- Semiologie OsteoarticulaireDocument90 pagesSemiologie OsteoarticulaireVikn SandNo ratings yet
- NPAPSNC 22 Aout 2023 Maladies Chroniques Decouvrez L Alimentation Acido Basique SDDocument20 pagesNPAPSNC 22 Aout 2023 Maladies Chroniques Decouvrez L Alimentation Acido Basique SDWilfrid MdtNo ratings yet