You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- The Lemonade Diet Ingredients and Recipe PDFDocument14 pagesThe Lemonade Diet Ingredients and Recipe PDFTradingTheEdges100% (3)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- NBME 5 ReviewDocument21 pagesNBME 5 ReviewVivian Tamara Suárez89% (9)
- Adult ADHD Self-Report Scale (ASRS-v1.1) Symptom ChecklistDocument2 pagesAdult ADHD Self-Report Scale (ASRS-v1.1) Symptom ChecklistMihaela VișanNo ratings yet
- Shy BookletDocument28 pagesShy BookletDesmond ScottNo ratings yet
- Fischer Hoffman ProcessDocument11 pagesFischer Hoffman ProcessNatalie Douglas100% (1)
- Professional Foundation Level Acupressure Training CourseDocument94 pagesProfessional Foundation Level Acupressure Training CourseLuis Del Valle TorregrosaNo ratings yet
- IntussusceptionDocument33 pagesIntussusceptionNovendi RizkaNo ratings yet
- Compulsive Stereotypic and Displacement DisordersDocument5 pagesCompulsive Stereotypic and Displacement DisordersBrook Farm Veterinary CenterNo ratings yet
- Acs (Acute Coronary Syndrome)Document54 pagesAcs (Acute Coronary Syndrome)xiaou123100% (1)
- Post Stroke EpilepsyDocument5 pagesPost Stroke EpilepsyNovendi RizkaNo ratings yet
- Edexcel As Biology Unit 1 Exam Revision NotesDocument19 pagesEdexcel As Biology Unit 1 Exam Revision Notesfockoffu100% (1)
- Lymphadenopathy: Soheir Adam, MD, MSC, MrcpathDocument34 pagesLymphadenopathy: Soheir Adam, MD, MSC, MrcpathWilly OematanNo ratings yet
- Accupuncture Needle DepthDocument21 pagesAccupuncture Needle DepthStephen T LeNo ratings yet
- Solucionario Advanced 1 Ed English PDFDocument24 pagesSolucionario Advanced 1 Ed English PDFLopez JoseNo ratings yet
- Meigs SyndromeDocument9 pagesMeigs SyndromeNovendi RizkaNo ratings yet
- Does ThrombolysisDocument7 pagesDoes ThrombolysisNovendi RizkaNo ratings yet
- Chap 5 eDocument10 pagesChap 5 eNovendi RizkaNo ratings yet
- 2 6 Mental Van OmmerenDocument7 pages2 6 Mental Van OmmerenNovendi RizkaNo ratings yet
- Efusi PleuraDocument15 pagesEfusi PleuraAnonymous KPhTy0CENo ratings yet
- AHA PALS MGMT of Shock FlowchartDocument1 pageAHA PALS MGMT of Shock FlowchartMulya's SaryNo ratings yet
- Postgrad Med J 2005 Yalamarthi 174 7Document5 pagesPostgrad Med J 2005 Yalamarthi 174 7Novendi RizkaNo ratings yet
- 04 - Marile Taine Ale Pamantului RomanescDocument116 pages04 - Marile Taine Ale Pamantului RomanescCorina VavaNo ratings yet
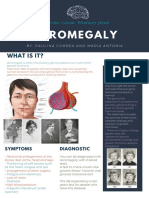
- Acromegaly: What Is It?Document1 pageAcromegaly: What Is It?Paulina CorreaaNo ratings yet
- The Prevention and Cure Effects of Aspirin Eugenol Ester On Hyperlipidemia and Its MetabonomicsDocument108 pagesThe Prevention and Cure Effects of Aspirin Eugenol Ester On Hyperlipidemia and Its MetabonomicsKavisa GhoshNo ratings yet
- Mag Ray Instruction ManualDocument7 pagesMag Ray Instruction Manualdigitaltext0% (1)
- Board Type-Power Final)Document171 pagesBoard Type-Power Final)Ibannor BanlasanNo ratings yet
- CASE REPORT On OsteomyelitisDocument30 pagesCASE REPORT On OsteomyelitisNirbhay KatiyarNo ratings yet
- Auriculo and NeuroDocument6 pagesAuriculo and NeuroFernândo SílvváNo ratings yet
- Defence MechanisDocument15 pagesDefence Mechanismanu sethi100% (2)
- Introduction To Psychology: Lecture 20 Transcript: BackDocument12 pagesIntroduction To Psychology: Lecture 20 Transcript: BackAltcineva VladNo ratings yet
- Notice: Draft Guidance For Industry: Validation of Growth-Based Rapid Microbiological Methods For Sterility Testing of Cellular and Gene Therapy Products AvailabilityDocument2 pagesNotice: Draft Guidance For Industry: Validation of Growth-Based Rapid Microbiological Methods For Sterility Testing of Cellular and Gene Therapy Products AvailabilityJustia.com100% (4)
- Paediatrica Indonesiana: Hindra Irawan Satari, Agus Firmansyah, TheresiaDocument8 pagesPaediatrica Indonesiana: Hindra Irawan Satari, Agus Firmansyah, TheresiaLestari Indah PratiwiNo ratings yet
- DiarroheaDocument44 pagesDiarroheaRashmi SharmaNo ratings yet
- Laporan Faal RespirasiDocument18 pagesLaporan Faal RespirasiLatifah RBNo ratings yet
- Oleh: Ayunda Larassati Basadi Pembimbing: Dr. I Ketut Sujana, Sp. PDDocument16 pagesOleh: Ayunda Larassati Basadi Pembimbing: Dr. I Ketut Sujana, Sp. PDMukhlisin Rizal100% (1)
- PEDIATRIC Blunt Abdominal Injury MGMT Guidelines AlgorithmDocument6 pagesPEDIATRIC Blunt Abdominal Injury MGMT Guidelines AlgorithmHaidir MuhammadNo ratings yet
- Caripirazine Review in SchizophreniaDocument13 pagesCaripirazine Review in SchizophreniaEsraa SaeedNo ratings yet
- UMMC Argatroban Protocol Revised 4-2008Document2 pagesUMMC Argatroban Protocol Revised 4-2008damondouglas100% (1)
- The Role of Yoga in Stress ManagementDocument30 pagesThe Role of Yoga in Stress ManagementKhabirul Alam0% (1)