You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5807)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Grinding Wheels, Honing Stones and Turning BitsDocument6 pagesGrinding Wheels, Honing Stones and Turning BitsSamer SalibaNo ratings yet
- Unofficial TranscriptDocument3 pagesUnofficial Transcriptapi-516350014No ratings yet
- Analisis Statistik JurnalDocument3 pagesAnalisis Statistik JurnalalaixmunakamalaNo ratings yet
- Desain Sampel Zidna Sabela - 418Document23 pagesDesain Sampel Zidna Sabela - 418alaixmunakamalaNo ratings yet
- Tesis Breastfeeding Challeges: Keywords: Breasfeeding, Formula MilkDocument1 pageTesis Breastfeeding Challeges: Keywords: Breasfeeding, Formula MilkalaixmunakamalaNo ratings yet
- Jurding Bu Siti ThomasDocument20 pagesJurding Bu Siti ThomasgembeljokerNo ratings yet
- WBC-Lymphocyte MaturationDocument4 pagesWBC-Lymphocyte MaturationalaixmunakamalaNo ratings yet
- RBC MaturationDocument8 pagesRBC MaturationalaixmunakamalaNo ratings yet
- Anal FistulaDocument6 pagesAnal Fistulaalaixmunakamala100% (1)
- Central Banking and Monetary PolicyDocument6 pagesCentral Banking and Monetary Policyrishit0504No ratings yet
- HSC ICT Sheet Chapter 03Document22 pagesHSC ICT Sheet Chapter 03Muhammad Masum Hosen100% (1)
- SABIC Flat ProductDocument15 pagesSABIC Flat ProductAiman AliNo ratings yet
- #2.5. Monitoring of Analog InputsDocument24 pages#2.5. Monitoring of Analog InputsNaufal Reyhan FadhilNo ratings yet
- Bhumitra Dubey-Economics ProjectDocument13 pagesBhumitra Dubey-Economics ProjectShinchan NoharaNo ratings yet
- Gideon Craft Ideas For Sunday SchoolDocument5 pagesGideon Craft Ideas For Sunday SchoolOhfallynMae Dela Cruz QuirozNo ratings yet
- Arch Styles Quiz Answer Sheet 2020-2Document1 pageArch Styles Quiz Answer Sheet 2020-2PatrickNo ratings yet
- 3 Gas Power CyclesDocument32 pages3 Gas Power CyclesFikri Azim100% (2)
- Woody Ornamentals Pest ManagementDocument59 pagesWoody Ornamentals Pest ManagementantonioforteseNo ratings yet
- Visual Weight Cheat Sheet NewDocument1 pageVisual Weight Cheat Sheet NewRicardo W. BrandNo ratings yet
- Cambridge International AS & A Level: Mathematics 9709/41Document16 pagesCambridge International AS & A Level: Mathematics 9709/41Juan ChavezNo ratings yet
- Gradient Domain High Dynamic Range Compression MatlabDocument3 pagesGradient Domain High Dynamic Range Compression MatlabRicky100% (1)
- Floor Plan BookletDocument10 pagesFloor Plan BookletZUK GamingNo ratings yet
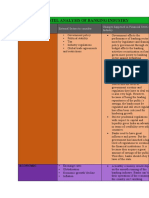
- Pestel Analysis of Banking IndustryDocument6 pagesPestel Analysis of Banking IndustryAnooja SajeevNo ratings yet
- English Language Marking SchemeDocument7 pagesEnglish Language Marking SchemeSamuel Arkorful JuniorNo ratings yet
- Booster VSD Atv 310 2 X 1,5 KWDocument6 pagesBooster VSD Atv 310 2 X 1,5 KWvanesapurnamapNo ratings yet
- Chapter 4 Heat Teacher's GuideDocument34 pagesChapter 4 Heat Teacher's GuideAhmad Zaidi100% (9)
- Syria Files - Re - SAUDI ARABIA Joradan France Israel CIA Spy Agencies Is INVESTING MILLIONS To TOPPLE ASSAD and IranDocument3 pagesSyria Files - Re - SAUDI ARABIA Joradan France Israel CIA Spy Agencies Is INVESTING MILLIONS To TOPPLE ASSAD and IranAl_AuransNo ratings yet
- (SUMMARY) OB Chapter 11Document4 pages(SUMMARY) OB Chapter 11Keane Indira NariswariNo ratings yet
- Integration Using Trigonometric TransformationsDocument10 pagesIntegration Using Trigonometric TransformationsGdeity PlaysNo ratings yet
- Ch3 Brute Force and Exhaustive Searchmodifieduntil StringmatchingDocument20 pagesCh3 Brute Force and Exhaustive Searchmodifieduntil StringmatchingAdan A AlawnehNo ratings yet
- Edexcel International GCSE Chemistry Chapter 12 The Halogens Learning PlanDocument1 pageEdexcel International GCSE Chemistry Chapter 12 The Halogens Learning PlanBesan BadranNo ratings yet
- PIANCwg 28 MainDocument87 pagesPIANCwg 28 Mainapi-370957950% (2)
- PCB Board Surface Finish CompareDocument2 pagesPCB Board Surface Finish ComparepcbboardszNo ratings yet
- MG6250 Ep04Document56 pagesMG6250 Ep04jhonnyNo ratings yet
- Ex Works PlanetsWater 'Full' AWG Direct Wholesale Factory Price List 2013Document9 pagesEx Works PlanetsWater 'Full' AWG Direct Wholesale Factory Price List 2013Oglas OglasiNo ratings yet
- True DiscountDocument8 pagesTrue Discountsathish14singhNo ratings yet
- Updates On Labor LawsDocument10 pagesUpdates On Labor LawsKoolen AlvarezNo ratings yet