You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Covid-19 Test Report: Patient Name: Akash GargDocument1 pageCovid-19 Test Report: Patient Name: Akash GargGenestrings Diagnostic CenterNo ratings yet
- Digi T Vigilance TestDocument6 pagesDigi T Vigilance TestJillianne FrancoNo ratings yet
- Table of Specification For Second Periodical Test in Mapeh IvDocument4 pagesTable of Specification For Second Periodical Test in Mapeh IvJENNIFER SERVONo ratings yet
- Bahasa Inggris UTS Kelas 5 SMT 2Document5 pagesBahasa Inggris UTS Kelas 5 SMT 2Aulia Laily MaulindaNo ratings yet
- Co2 Laser CatalogueDocument24 pagesCo2 Laser CatalogueBlin RodsNo ratings yet
- Empowering Parents: AutismDocument10 pagesEmpowering Parents: AutismSuellen Concessio FernandesNo ratings yet
- Range Animal Nutrition (Exercise)Document48 pagesRange Animal Nutrition (Exercise)AkyasManjaniqNo ratings yet
- 7.5.2.2 Final Report of Dumagat AuroraDocument127 pages7.5.2.2 Final Report of Dumagat AuroraAlvin HalconNo ratings yet
- Skin CareDocument5 pagesSkin Carejoseph100% (1)
- MMQL Escala YoungDocument8 pagesMMQL Escala YoungDanny PazNo ratings yet
- Obstetrical Procedures 72Document3 pagesObstetrical Procedures 72Rosnalia HariyantoNo ratings yet
- Formal Special Areas: Border Management Red Corridor PncpcaDocument29 pagesFormal Special Areas: Border Management Red Corridor PncpcaAnirban MandalNo ratings yet
- Notification No.19151 - Revised Guidelines MUKTADocument22 pagesNotification No.19151 - Revised Guidelines MUKTADeepak PeraNo ratings yet
- Intern TicklerDocument10 pagesIntern TicklerRem AlfelorNo ratings yet
- Operating Room Personnel OrganizationDocument4 pagesOperating Room Personnel OrganizationantihistamiiineNo ratings yet
- Communication and Nutrional EducationDocument11 pagesCommunication and Nutrional EducationSabrina PanjaitanNo ratings yet
- Define Hospital ManagementDocument4 pagesDefine Hospital ManagementRenit AntoNo ratings yet
- Clinical Surgical 1Document2 pagesClinical Surgical 1Ohana NanaNo ratings yet
- Anti-Inflammatory Diet: What Is Inflammation?Document13 pagesAnti-Inflammatory Diet: What Is Inflammation?Perrela PerrelaNo ratings yet
- Tratament Diuretic in Insuficienta CardiacaDocument19 pagesTratament Diuretic in Insuficienta CardiacaOlga HMNo ratings yet
- Occupational Therapy Assessment: 1. SensesDocument17 pagesOccupational Therapy Assessment: 1. SensesVIJAYA DHARSHINI M Bachelor in Occupational Therapy (BOT)No ratings yet
- Contractor Safety Rules PDFDocument10 pagesContractor Safety Rules PDFKEERTHI INDUSTRIESNo ratings yet
- Perbandingan Kasus Fatal Akibat Covid-19 Pada Beberapa Negara Asia TenggaraDocument6 pagesPerbandingan Kasus Fatal Akibat Covid-19 Pada Beberapa Negara Asia Tenggarasofia uyNo ratings yet
- Go Wyoming (Sept. 17, 2020)Document24 pagesGo Wyoming (Sept. 17, 2020)Watertown Daily TimesNo ratings yet
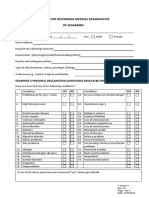
- Format For Recording Medical Examinatios of SeafarersDocument4 pagesFormat For Recording Medical Examinatios of SeafarersАлексNo ratings yet
- (Comprehensive Geriatric Assessment) Experiencia Com Idosos de Colombia E BrasilDocument27 pages(Comprehensive Geriatric Assessment) Experiencia Com Idosos de Colombia E BrasilBrisa NarvaezNo ratings yet
- Mal PresentationsDocument4 pagesMal Presentationsإسراء محمودNo ratings yet
- Nazanin HorriDocument2 pagesNazanin Horrifonochu FrankzenoNo ratings yet
- Nursing Care Plan: Clustered Cues Nursing Diagnosis Rationale Outcome Criteria Nursing Intervention Rationale EvaluationDocument23 pagesNursing Care Plan: Clustered Cues Nursing Diagnosis Rationale Outcome Criteria Nursing Intervention Rationale EvaluationTweenie DalumpinesNo ratings yet
- Pyeongtaek City Foreigner GuideDocument54 pagesPyeongtaek City Foreigner Guidejoelbuxton100% (2)