You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5810)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Elictation and CollaborationDocument28 pagesElictation and CollaborationalisterjosephNo ratings yet
- The Psychology of HappinessDocument32 pagesThe Psychology of HappinessPaulo Viana100% (1)
- Sample EssayDocument3 pagesSample EssayGunawan AdhigunaNo ratings yet
- Agma 2015 915-1-A02Document152 pagesAgma 2015 915-1-A02neno2405No ratings yet
- Mplsheartjournal D 17 00004Document6 pagesMplsheartjournal D 17 00004Irina NeamtuNo ratings yet
- 1218 Anexa 15 - 8724 - 6616Document9 pages1218 Anexa 15 - 8724 - 6616Irina NeamtuNo ratings yet
- Epidemiology of Peripheral Artery DiseaseDocument18 pagesEpidemiology of Peripheral Artery DiseaseIrina NeamtuNo ratings yet
- Managementul Pacientilor Boala Arteriala PerifericaDocument5 pagesManagementul Pacientilor Boala Arteriala PerifericaIrina NeamtuNo ratings yet
- Incidence of Peripheral Vascular Changes in Diabetes MellitusDocument5 pagesIncidence of Peripheral Vascular Changes in Diabetes MellitusIrina NeamtuNo ratings yet
- Pi Is 0741521414007095Document12 pagesPi Is 0741521414007095Irina NeamtuNo ratings yet
- Managementul Pacientilor Boala Arteriala PerifericaDocument2 pagesManagementul Pacientilor Boala Arteriala PerifericaIrina NeamtuNo ratings yet
- Complications After Peripheral Vascular Interventions in OctogenariansDocument7 pagesComplications After Peripheral Vascular Interventions in OctogenariansIrina NeamtuNo ratings yet
- Population-Based Study of Incidence, Risk Factors, Outcome, and Prognosis of Ischemic Peripheral Arterial EventsDocument11 pagesPopulation-Based Study of Incidence, Risk Factors, Outcome, and Prognosis of Ischemic Peripheral Arterial EventsIrina NeamtuNo ratings yet
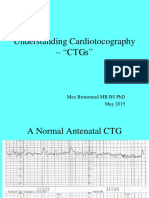
- Understanding Cardiotocography - "CTGS": Max Brinsmead MB Bs PHD May 2015Document29 pagesUnderstanding Cardiotocography - "CTGS": Max Brinsmead MB Bs PHD May 2015Irina NeamtuNo ratings yet
- 24Document485 pages24Irina Neamtu100% (1)
- 04 Jul Aug 0414 MeltonDocument9 pages04 Jul Aug 0414 MeltonajipalipatlipatNo ratings yet
- Switch Gear SafetyDocument16 pagesSwitch Gear SafetyAnila SadasivanNo ratings yet
- Classroom Confidential - Sarah KarnasiewiczDocument9 pagesClassroom Confidential - Sarah KarnasiewiczEmilie AnnNo ratings yet
- Mendoza vs. ArrietaDocument2 pagesMendoza vs. ArrietaDara CompuestoNo ratings yet
- Group 1 Research PaperDocument60 pagesGroup 1 Research Paperkaith etcubanNo ratings yet
- 十二生肖Zodiac and Names of YearsanimalsDocument31 pages十二生肖Zodiac and Names of YearsanimalsyueNo ratings yet
- Stortel WLNDocument3 pagesStortel WLNPonpes Sumber BarokahNo ratings yet
- Tutorial Cylinder Refined MeshDocument9 pagesTutorial Cylinder Refined MeshShawn WaltzNo ratings yet
- Neo Fax 2011Document409 pagesNeo Fax 2011Lourdes M. RodriguezNo ratings yet
- Religious Policy of AkbarDocument10 pagesReligious Policy of AkbarAnuj PratapNo ratings yet
- Mark (10) Divorce & RemarriageDocument7 pagesMark (10) Divorce & RemarriageJoseph Faustin LunguNo ratings yet
- Exp No. 11 Chem Process Lab ReportDocument5 pagesExp No. 11 Chem Process Lab ReportSourav SutradharNo ratings yet
- Movements and Media As Interacting Systems. Ann Am Acad Polit Soc SciDocument14 pagesMovements and Media As Interacting Systems. Ann Am Acad Polit Soc SciTalita SouzaNo ratings yet
- Contrastive WEEK 3Document11 pagesContrastive WEEK 3Nguyễn Anh DuyNo ratings yet
- Gour Govinda Swami - Sri Krishna JanmastamiDocument30 pagesGour Govinda Swami - Sri Krishna JanmastamiOnkar YemulNo ratings yet
- Activity 5 Genres of Pop CultureDocument1 pageActivity 5 Genres of Pop CultureJoshua Jae AquinoNo ratings yet
- Good Manners and God BehaviorDocument36 pagesGood Manners and God BehaviorJhanette De Los ReyesNo ratings yet
- Letter of Recommendation For École Polytechnique's Bachelor ProgramDocument2 pagesLetter of Recommendation For École Polytechnique's Bachelor ProgramRishabh TaNo ratings yet
- NCFP Membership FormDocument2 pagesNCFP Membership FormDennisEstrellosoAlbisoNo ratings yet
- Grant Etal 2017Document93 pagesGrant Etal 2017catmyngiNo ratings yet
- HP Vertica 7.1.x IntegratingApacheHadoopDocument135 pagesHP Vertica 7.1.x IntegratingApacheHadoopRahul VishwakarmaNo ratings yet
- Modules 01-02 Progress Test 1A: MusicDocument8 pagesModules 01-02 Progress Test 1A: MusicCsalád RéderNo ratings yet
- What Is A Persuasive EssayDocument3 pagesWhat Is A Persuasive EssayMicaela EncinasNo ratings yet
- PDF Upload-366341Document17 pagesPDF Upload-366341edm kdNo ratings yet
- The Impacts of Self-Driving Cars On Society: A Review: Submitted By: Raihan Rahman ID: 1830006Document10 pagesThe Impacts of Self-Driving Cars On Society: A Review: Submitted By: Raihan Rahman ID: 1830006Raihan RahmanNo ratings yet
- Shadow of The ForestDocument2 pagesShadow of The ForestAnita StankovicNo ratings yet