You might also like
- Medicine Alaa Notes (All Files Merged) - Best Pro Choice-.Pdf-1Document120 pagesMedicine Alaa Notes (All Files Merged) - Best Pro Choice-.Pdf-1maimoona suleman100% (6)
- My Personal Experience With The Hpcna Forein Trained Medical Lisencening Examination 1Document15 pagesMy Personal Experience With The Hpcna Forein Trained Medical Lisencening Examination 1Kandiwapa Shivute100% (2)
- Example of Personal StatementDocument3 pagesExample of Personal StatementSamer Ehab100% (3)
- Stroke Lecture PDFDocument41 pagesStroke Lecture PDFPAK DHENo ratings yet
- Systemic Lupus Erythematosus: Medical Surgical and Critical Care DepartmentDocument31 pagesSystemic Lupus Erythematosus: Medical Surgical and Critical Care DepartmentLalisaM ActivityNo ratings yet
- Systemic Lupus Erythematosus: Medical Surgical and Critical Care DepartmentDocument31 pagesSystemic Lupus Erythematosus: Medical Surgical and Critical Care DepartmentLalisaM ActivityNo ratings yet
- Connective Tissue Disorders: DR Josephine Ojoo MBCHB FRCP CCST (Resp) Dip Hiv Med Senior Lecturer Maseno UniversityDocument70 pagesConnective Tissue Disorders: DR Josephine Ojoo MBCHB FRCP CCST (Resp) Dip Hiv Med Senior Lecturer Maseno UniversityMalueth AnguiNo ratings yet
- Autoimmune DisordersDocument33 pagesAutoimmune DisordersSteph ReyesNo ratings yet
- Connect Tissue 200002Document54 pagesConnect Tissue 200002AyeshaNo ratings yet
- SleDocument66 pagesSleNur Liyana Ahmad Zaki100% (1)
- Systemic Lupus Erythematosus: Jason Ryan, MD, MPHDocument22 pagesSystemic Lupus Erythematosus: Jason Ryan, MD, MPHLava calolaNo ratings yet
- 5.rheumatology SummaryDocument123 pages5.rheumatology SummarytotyNo ratings yet
- 5.rheumatology SummaryDocument123 pages5.rheumatology SummaryAyatNo ratings yet
- Autoimmune DiseasesDocument70 pagesAutoimmune DiseasesAdebisi OluwatomiwaNo ratings yet
- Disorders of The Immune System 3: Richard A. Mcpherson, M.DDocument45 pagesDisorders of The Immune System 3: Richard A. Mcpherson, M.DrismaarnisNo ratings yet
- Autoimmune Disorders: DR Muhammad ZUBAIR Consultant Chemical PathologistDocument52 pagesAutoimmune Disorders: DR Muhammad ZUBAIR Consultant Chemical PathologistZubair YousafNo ratings yet
- Systemic Lupus ErythematosusDocument40 pagesSystemic Lupus ErythematosusAkshan SentinelNo ratings yet
- Systemic Lupus ErythematosusDocument11 pagesSystemic Lupus Erythematosuspumpkin_kingNo ratings yet
- Ch6 Immune 1Document81 pagesCh6 Immune 1Louis FortunatoNo ratings yet
- Immune Disorders..Ppt FairDocument79 pagesImmune Disorders..Ppt FairSumi SebastianNo ratings yet
- Rheumatology Summary From AmbusDocument77 pagesRheumatology Summary From AmbusAlupoaie SilviuNo ratings yet
- Arthritis and Related Connective Tissue DiseasesDocument201 pagesArthritis and Related Connective Tissue DiseasesJuanitoCabatañaLimIIINo ratings yet
- Pediatric Systemic Lupus Erythematosus: Pediatric Rheumatology Red Team Resident Teaching SeriesDocument52 pagesPediatric Systemic Lupus Erythematosus: Pediatric Rheumatology Red Team Resident Teaching SeriesLili ManaoNo ratings yet
- Rheumatology Year 4Document90 pagesRheumatology Year 4Abdalla SamatarNo ratings yet
- Diseases of BLOOD VESSELSDocument119 pagesDiseases of BLOOD VESSELSmeeeenonNo ratings yet
- Lecture 5.16 - LeucaemiaDocument16 pagesLecture 5.16 - LeucaemiajernsssNo ratings yet
- Immune DisorderDocument37 pagesImmune DisorderJessica TieuNo ratings yet
- Systemic Lupus ErythematosusDocument37 pagesSystemic Lupus ErythematosusdzikroulNo ratings yet
- SLE by Mahmoud - IbrahimDocument7 pagesSLE by Mahmoud - Ibrahimradybdh000No ratings yet
- Biology Project For Class 12Document21 pagesBiology Project For Class 12kishore kolanjiNo ratings yet
- BCA Immune2020Document40 pagesBCA Immune2020Inukaicchi TakumichiNo ratings yet
- Systemic Lupus ErythematosusDocument1 pageSystemic Lupus ErythematosusZara MohammedNo ratings yet
- Mechanisms of AutoimmunityDocument22 pagesMechanisms of Autoimmunitybudi darmantaNo ratings yet
- Systemic Lupus ErythematosusDocument75 pagesSystemic Lupus ErythematosusThe AbyssinicansNo ratings yet
- Splenomegaly and White Cell Abnormalities: Benjamin Kizito Birungi Facilitator: Dr. Ssebuliba MosesDocument58 pagesSplenomegaly and White Cell Abnormalities: Benjamin Kizito Birungi Facilitator: Dr. Ssebuliba MosesNinaNo ratings yet
- Systemic Lupus Erythematosus: The Hydra Headed, The Chameleonic Disease!!Document42 pagesSystemic Lupus Erythematosus: The Hydra Headed, The Chameleonic Disease!!adamu mohammadNo ratings yet
- Diseases of The Immune System (II)Document73 pagesDiseases of The Immune System (II)Visca ZerlindaNo ratings yet
- Autoimmune Diseases: Clinical NutritionDocument39 pagesAutoimmune Diseases: Clinical NutritionRachael TheisenNo ratings yet
- Systemic Lupus Erythematosus SLE: DefinitionDocument19 pagesSystemic Lupus Erythematosus SLE: DefinitionShimmering MoonNo ratings yet
- Systemic Lupus Eritematus Kuliah KlerkDocument76 pagesSystemic Lupus Eritematus Kuliah KlerkAnonymous y6NmP9NHkYNo ratings yet
- Systemic Lupus ErythematosusDocument37 pagesSystemic Lupus ErythematosusFirman Ichlasul AmalNo ratings yet
- 07.02.2020 Lupus ErythematosusDocument67 pages07.02.2020 Lupus ErythematosussujataNo ratings yet
- RHEUMATOLOGYDocument121 pagesRHEUMATOLOGYYuni Pratiwi80% (5)
- Dermatology Lupus Erythematosus: Name: Muhammad Nooraiman Ahmad Noordin Group: 30 ADocument14 pagesDermatology Lupus Erythematosus: Name: Muhammad Nooraiman Ahmad Noordin Group: 30 AAiman TymerNo ratings yet
- AutoinmunidadDocument21 pagesAutoinmunidadRobert Caballero BardalesNo ratings yet
- Systemic Lupus Erythematosus: Pathogenesis, Clinical Manifestations and DiagnosisDocument51 pagesSystemic Lupus Erythematosus: Pathogenesis, Clinical Manifestations and DiagnosisNesa Telge GintingNo ratings yet
- Systemic Lupus Erythematosus & Rheumatoid Arthritis: Hildebrand Hanoch Victor Departemen Ilmu Penyakit Dalam FK Uki 2014Document65 pagesSystemic Lupus Erythematosus & Rheumatoid Arthritis: Hildebrand Hanoch Victor Departemen Ilmu Penyakit Dalam FK Uki 2014JendrianiNo ratings yet
- Week 16 - Autoimmune DiseasesDocument25 pagesWeek 16 - Autoimmune DiseasesKyle CollladoNo ratings yet
- RH 2Document23 pagesRH 2bismahNo ratings yet
- Dental Considerations For Patients With Lupus ErythematosusDocument55 pagesDental Considerations For Patients With Lupus ErythematosusPhyo Ko KoNo ratings yet
- Unit 3 Part 4 Organ-Specific Autoimmune DisordersDocument23 pagesUnit 3 Part 4 Organ-Specific Autoimmune DisordersReman AlingasaNo ratings yet
- Lupus: Dr. John BergmanDocument62 pagesLupus: Dr. John BergmanAndrew FongNo ratings yet
- Systemic Lupus ErythematosusDocument68 pagesSystemic Lupus Erythematosustitis sariNo ratings yet
- Systemic Lupus ErythematosusDocument29 pagesSystemic Lupus ErythematosusNoreen PadillaNo ratings yet
- Medical MnemonicsDocument65 pagesMedical MnemonicsMIRZA MUHAMMAD ADNAN100% (1)
- Auto Immune Disorder 2016Document38 pagesAuto Immune Disorder 2016vistaNo ratings yet
- Muskuloskeletal 2Document80 pagesMuskuloskeletal 2feby faradillaNo ratings yet
- Systemic Lupus Erythematosus (SLE)Document56 pagesSystemic Lupus Erythematosus (SLE)Hendy Tri Saputra SigaiNo ratings yet
- Systemic Lupus Erythematosus: June 1& 8, 2015Document94 pagesSystemic Lupus Erythematosus: June 1& 8, 2015Azizan HannyNo ratings yet
- Types of Arthritis 1Document22 pagesTypes of Arthritis 1Mikee PaningbatanNo ratings yet
- Skin Problems in RheumatologyDocument52 pagesSkin Problems in RheumatologyAyi Abdul BasithNo ratings yet
- Sle 1Document36 pagesSle 1Votey CHNo ratings yet
- Rheumatoid ArthritisDocument53 pagesRheumatoid ArthritisnsamariosNo ratings yet
- Cleodocranial Dysplasis 2018 Dr. KH ShivuteDocument22 pagesCleodocranial Dysplasis 2018 Dr. KH ShivuteKandiwapa ShivuteNo ratings yet
- Cell InjuryDocument10 pagesCell InjuryKandiwapa ShivuteNo ratings yet
- 5 Direct RetainersDocument56 pages5 Direct RetainersKandiwapa ShivuteNo ratings yet
- Introduction To CTDocument36 pagesIntroduction To CTKandiwapa ShivuteNo ratings yet
- Lecture 2 Oral Mucosa and Lips 2018-02-16Document6 pagesLecture 2 Oral Mucosa and Lips 2018-02-16Kandiwapa ShivuteNo ratings yet
- Questions of The Lectures 1Document1 pageQuestions of The Lectures 1Kandiwapa ShivuteNo ratings yet
- Radiation Safety of Medical Staff, Working With Sources of Ionizing RadiationDocument50 pagesRadiation Safety of Medical Staff, Working With Sources of Ionizing RadiationKandiwapa ShivuteNo ratings yet
- Mucogingival Surgery: Recession: K H Shivute Final Year Dental Student Dental Surgery Sechenov University '18Document31 pagesMucogingival Surgery: Recession: K H Shivute Final Year Dental Student Dental Surgery Sechenov University '18Kandiwapa Shivute100% (1)
- Lecture 1. Surgical DentistryDocument40 pagesLecture 1. Surgical DentistryKandiwapa ShivuteNo ratings yet
- 3rd Lecture Oral MucosaDocument13 pages3rd Lecture Oral MucosaKandiwapa ShivuteNo ratings yet
- Lecture 2 Boils and Carbucules - Ru.enDocument22 pagesLecture 2 Boils and Carbucules - Ru.enKandiwapa ShivuteNo ratings yet
- Oniipa Town Dream BigDocument2 pagesOniipa Town Dream BigKandiwapa ShivuteNo ratings yet
- Ans 30 Dec Nbde 1 RQDocument10 pagesAns 30 Dec Nbde 1 RQKandiwapa ShivuteNo ratings yet
- Trusted Medical Answers-In Seconds.: General MycologyDocument19 pagesTrusted Medical Answers-In Seconds.: General MycologyntnquynhproNo ratings yet
- Bells PalsyDocument15 pagesBells PalsyDavid SugiartoNo ratings yet
- Aedes Species in Laboratory"Document3 pagesAedes Species in Laboratory"International Journal of Innovative Science and Research TechnologyNo ratings yet
- 2011 Conference Handbook: 26-28 September 2011Document3 pages2011 Conference Handbook: 26-28 September 2011Fiskha WihanarniNo ratings yet
- Terapi Pasien HMS 2020Document108 pagesTerapi Pasien HMS 2020alvindwi lufikaNo ratings yet
- Pucci 2005Document4 pagesPucci 2005yorghiLNo ratings yet
- Case Report: Yafanita Izzati Nurina, Usman HadiDocument8 pagesCase Report: Yafanita Izzati Nurina, Usman HadiZuraidaNo ratings yet
- Nut 3704 AssignmentDocument6 pagesNut 3704 AssignmentCebisile NeneNo ratings yet
- FDARDocument2 pagesFDARTrisha Marie JimenezNo ratings yet
- Strong: Nutritional Risk Screening Tool For Children Aged Month - 18 Years On Admission To The HospitalDocument3 pagesStrong: Nutritional Risk Screening Tool For Children Aged Month - 18 Years On Admission To The HospitalninaNo ratings yet
- Acute and Chronic OsteomyelitisDocument19 pagesAcute and Chronic OsteomyelitisEndy Destriawan50% (2)
- Final Exam Bis 380Document4 pagesFinal Exam Bis 380api-613297004No ratings yet
- Dengue Report (For Checking)Document34 pagesDengue Report (For Checking)Mark ReyesNo ratings yet
- Page 2012 RESEARCH DESIGNS IN SPORTS PHYSICAL THERAPY PDFDocument11 pagesPage 2012 RESEARCH DESIGNS IN SPORTS PHYSICAL THERAPY PDFValeRichardNo ratings yet
- Absolute, Relative and Attributable RisksDocument61 pagesAbsolute, Relative and Attributable RisksIndah Afriani NasutionNo ratings yet
- Overlooked 150 Year Old Household Cleaner A Remedy For Swine Flu?Document4 pagesOverlooked 150 Year Old Household Cleaner A Remedy For Swine Flu?nsmith7100% (2)
- Theme 6 ChlamydiaDocument28 pagesTheme 6 ChlamydiaAmitNo ratings yet
- Unhealthful Lifestyle and Personal Habits Specifically Poor Personal Hygiene As Health ThreatDocument1 pageUnhealthful Lifestyle and Personal Habits Specifically Poor Personal Hygiene As Health ThreatGlaire ZarateNo ratings yet
- 4.case History in CD - Extra OralDocument16 pages4.case History in CD - Extra OralDrRakesh MishraNo ratings yet
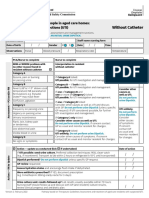
- Form Ams Clinical Pathway Fillable Form Without CatheterDocument1 pageForm Ams Clinical Pathway Fillable Form Without CatheterTeenu JobyNo ratings yet
- Minor Head Trauma in Infants and Childre ManagmentDocument12 pagesMinor Head Trauma in Infants and Childre ManagmentRita ValenteNo ratings yet
- Hubungan Lama Hemodialisis Dengan Kardiomegali Pada Pasien Gagal Ginjal Kronik Di Unit Hemodialisa Rumah Sakit DustiraDocument9 pagesHubungan Lama Hemodialisis Dengan Kardiomegali Pada Pasien Gagal Ginjal Kronik Di Unit Hemodialisa Rumah Sakit DustiraPbkkel 15No ratings yet
- Principles of Epidemiology - Part (I)Document40 pagesPrinciples of Epidemiology - Part (I)khalid alatwiNo ratings yet
- Patient Profile: 1 - PageDocument9 pagesPatient Profile: 1 - PagelynlynNo ratings yet
- CertificateDocument1 pageCertificateAbhijit MishraNo ratings yet
- 17.uzuegbunam Miracle ChiamakaDocument17 pages17.uzuegbunam Miracle ChiamakaEchezonaNo ratings yet
- Department of Haematology Test Name Result Unit Bio. Ref. Range MethodDocument5 pagesDepartment of Haematology Test Name Result Unit Bio. Ref. Range MethodSunil KhandekarNo ratings yet