You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5814)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- 0nvkwxysn505jodxuxkr5z3v PDFDocument2 pages0nvkwxysn505jodxuxkr5z3v PDFAnjali Thomas50% (2)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Kidney Quiz - Path Exam 3Document15 pagesKidney Quiz - Path Exam 3tatti9990% (1)
- Phyllanthus Amarus Ethnomedicinal Uses Phytochemistry and Pharmacology PDFDocument29 pagesPhyllanthus Amarus Ethnomedicinal Uses Phytochemistry and Pharmacology PDFPaula AlmeidaNo ratings yet
- Pathogenesis of Bacterial InfectionDocument9 pagesPathogenesis of Bacterial Infectionsonyda444No ratings yet
- Patient Info/doctor/febrile-ConvulsionsDocument6 pagesPatient Info/doctor/febrile-Convulsionsholly theressaNo ratings yet
- Para Sa KinabukasanDocument40 pagesPara Sa KinabukasanMickey mg100% (1)
- Fungal KeratitisDocument34 pagesFungal KeratitisbhartiNo ratings yet
- History of Hospital-Acquired InfectionsDocument16 pagesHistory of Hospital-Acquired InfectionsRasha MuhammadNo ratings yet
- Pigeon Racing PigeonDocument7 pagesPigeon Racing Pigeonsundarhicet83No ratings yet
- Sexual Intercourse - Painful DefinitionDocument6 pagesSexual Intercourse - Painful DefinitionVali EnciuNo ratings yet
- DiseaseDocument8 pagesDiseaseErnest CañosNo ratings yet
- Periodic TestDocument6 pagesPeriodic TestDhang Nario100% (1)
- Form ICRA HAIsDocument25 pagesForm ICRA HAIsLakhsmie Herawati YuwantinaNo ratings yet
- 123Document40 pages123Shannara21100% (1)
- Expanded Program On ImmunizationDocument5 pagesExpanded Program On ImmunizationFreya Revamonte100% (6)
- Mefloquine LariamDocument1,753 pagesMefloquine LariamJudicial Watch, Inc.No ratings yet
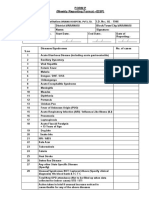
- Form P (Weekly Reporting Format - IDSP) : Oriana Hospital PVT - LTDDocument2 pagesForm P (Weekly Reporting Format - IDSP) : Oriana Hospital PVT - LTDRavi ParmarNo ratings yet
- Altered Immune ResponseDocument20 pagesAltered Immune Responsesho bartNo ratings yet
- East Africa University Bosaso, Puntland Somalia Faculty of Medicine Communicable Disease MR Buruj Ali SaladDocument42 pagesEast Africa University Bosaso, Puntland Somalia Faculty of Medicine Communicable Disease MR Buruj Ali SaladShaimaa AbdulkadirNo ratings yet
- POINTERSDocument49 pagesPOINTERSJonas Marvin AnaqueNo ratings yet
- Pregnant Women Invitation LetterDocument3 pagesPregnant Women Invitation LetterDulanjalee SachittraNo ratings yet
- 4-Farmakologi Obat Penyakit MataDocument30 pages4-Farmakologi Obat Penyakit MataDensy Nurtita FitrianiNo ratings yet
- Cutaneous Manifestations of TuberculosisDocument35 pagesCutaneous Manifestations of TuberculosisSaid Plazola MercadoNo ratings yet
- Covid 19Document22 pagesCovid 19imad khanNo ratings yet
- BSC MLT PDFDocument23 pagesBSC MLT PDFMayur Parmar0% (1)
- When You've Been Fully Vaccinated - CDC - 7.27.21Document3 pagesWhen You've Been Fully Vaccinated - CDC - 7.27.21WWMTNo ratings yet
- Bronchitis LectureDocument46 pagesBronchitis LecturesanathanadharmaNo ratings yet
- AbstractDocument1 pageAbstractLauAnRuNo ratings yet
- 150 Question Labce Quez. 1 PDFDocument87 pages150 Question Labce Quez. 1 PDFadvance ascpNo ratings yet
- CNS Infection - NelsonDocument13 pagesCNS Infection - Nelsonsai saiNo ratings yet