You might also like
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Shing Tu MandirDocument13 pagesShing Tu Mandirkostya1No ratings yet
- Chinese HisotryDocument2 pagesChinese Hisotrykostya1No ratings yet
- Chinese CultureDocument14 pagesChinese CultureDaisyTsui100% (1)
- Developmental Psychology SS271 Assignment #2 (Worth 5% of Your Final Grade) Choose One of The Following Two Options: Option 1: Interview A Parent AssignmentDocument6 pagesDevelopmental Psychology SS271 Assignment #2 (Worth 5% of Your Final Grade) Choose One of The Following Two Options: Option 1: Interview A Parent Assignmentkostya1No ratings yet
- Loinc and Snomed CT: Daniel J. Vreeman, PT, DPT, MSCDocument88 pagesLoinc and Snomed CT: Daniel J. Vreeman, PT, DPT, MSCkostya1No ratings yet
- 11 X 17 Printing Instructions PDFDocument1 page11 X 17 Printing Instructions PDFkostya1No ratings yet
- MIDDLE ADULTHOOD: THE PEAK AND DECLINEDocument10 pagesMIDDLE ADULTHOOD: THE PEAK AND DECLINEkostya1No ratings yet
- HandbookDocument17 pagesHandbookkostya1No ratings yet
- 11 X 17 Printing InstructionsDocument21 pages11 X 17 Printing Instructionskostya1No ratings yet
- LeadershipDocument67 pagesLeadershipkostya1No ratings yet
- LeadershipDocument67 pagesLeadershipkostya1No ratings yet
- 2010 EA Conf - RA Track Presentation - 20100506Document47 pages2010 EA Conf - RA Track Presentation - 20100506John OhnoNo ratings yet
- CHC Student Created Test Questions (2) - Feb15-2018Document12 pagesCHC Student Created Test Questions (2) - Feb15-2018kostya1No ratings yet
- Niagara OutlineDocument3 pagesNiagara Outlinekostya1No ratings yet
- 神经外科双语教学课件Document262 pages神经外科双语教学课件kostya1No ratings yet
- 11 X 17 Printing InstructionsDocument1 page11 X 17 Printing Instructionskostya1No ratings yet
- CaseDocument3 pagesCasekostya1No ratings yet
- Bullous Dermatoses112Document84 pagesBullous Dermatoses112kostya1No ratings yet
- Cultural Communication in Norwegian HealthcareDocument9 pagesCultural Communication in Norwegian Healthcarekostya1No ratings yet
- Comprehensive Search ReportDocument3 pagesComprehensive Search Reportkostya1No ratings yet
- Research PaperDocument8 pagesResearch PaperSumit AcharyaNo ratings yet
- Application Form Sec 10 CHDDocument6 pagesApplication Form Sec 10 CHDkostya1No ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Il Gem 4000 Operating and Maintenance ProcedureDocument15 pagesIl Gem 4000 Operating and Maintenance ProcedureHfsh OmerNo ratings yet
- Brosur Signa ExplorerDocument16 pagesBrosur Signa ExplorerEky Novri ArdiNo ratings yet
- Work Book. Anatomy of Female Reproductive Organs. Methods of ExaminationDocument4 pagesWork Book. Anatomy of Female Reproductive Organs. Methods of ExaminationNathalie DeebNo ratings yet
- Formula and TablesDocument6 pagesFormula and TablesMaria RahimNo ratings yet
- Thrombolytic TherapyDocument37 pagesThrombolytic TherapySani sunilNo ratings yet
- AlopeciaDocument2 pagesAlopeciaAldrich ArquizaNo ratings yet
- Acute Compartment Syndrome of The Extremities - UpToDateDocument22 pagesAcute Compartment Syndrome of The Extremities - UpToDateSatrio Bangun NegoroNo ratings yet
- L95 NecropsyDocument7 pagesL95 NecropsyKING 5 News100% (1)
- Medical Etymology: by Teresa Marcotte & Beth BoyerDocument67 pagesMedical Etymology: by Teresa Marcotte & Beth Boyerbethboyer1No ratings yet
- Pflipsen Anaphylaxis Recognition and ManagementDocument10 pagesPflipsen Anaphylaxis Recognition and ManagementOlivia McCuskerNo ratings yet
- Childhood Trauma:Impact On Personality/Role in Personality DisordersDocument13 pagesChildhood Trauma:Impact On Personality/Role in Personality DisordersNancee Y.No ratings yet
- NCP FinalDocument4 pagesNCP Finalmarkanthony3903No ratings yet
- PREBORD NLE8part1Document671 pagesPREBORD NLE8part1Bryan NorwayneNo ratings yet
- Family Case StudyDocument25 pagesFamily Case StudyJezner GamosNo ratings yet
- Status EpilepticusDocument22 pagesStatus EpilepticusVivi Kristiani RumapeaNo ratings yet
- Diagnosing Pompe Disease (Also Known As AcidDocument4 pagesDiagnosing Pompe Disease (Also Known As Aciddonnal47No ratings yet
- Time Table Panitia - NewDocument3 pagesTime Table Panitia - NewcelinNo ratings yet
- Fact Sheet on Emerging and Re-Emerging Infectious DiseasesDocument7 pagesFact Sheet on Emerging and Re-Emerging Infectious DiseasesAmanda PratiwiNo ratings yet
- HS 2212 Wa U5Document4 pagesHS 2212 Wa U5bnvjNo ratings yet
- Emrcp CNS 38-62Document22 pagesEmrcp CNS 38-62dryusufsNo ratings yet
- Recent Updates On Nanomedicine Based Products: Current Sce-Nario and Future OpportunitiesDocument13 pagesRecent Updates On Nanomedicine Based Products: Current Sce-Nario and Future OpportunitiesvijuNo ratings yet
- Acute Prescribing - Challenges and Solutions - Ajit KulkarniDocument51 pagesAcute Prescribing - Challenges and Solutions - Ajit KulkarniAgha QaimiNo ratings yet
- Lecture 3-Epidemiological TriadDocument19 pagesLecture 3-Epidemiological Triadvikas takNo ratings yet
- Medico-Legal Aspects of Physical InjuriesDocument9 pagesMedico-Legal Aspects of Physical InjuriesRhem Rick Corpuz100% (1)
- Doctor's OrderDocument2 pagesDoctor's OrderWiljohn de la CruzNo ratings yet
- Antenatal CareDocument12 pagesAntenatal CarefiramnNo ratings yet
- Infective EndocarditisDocument3 pagesInfective EndocarditisAlfrin Antony80% (5)
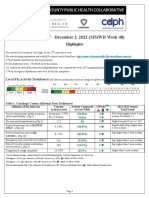
- 2022-23 Flu Surveillance Report - Week 48Document5 pages2022-23 Flu Surveillance Report - Week 48WKYC.comNo ratings yet
- Europian Surgical Abstract 2 PDFDocument114 pagesEuropian Surgical Abstract 2 PDFDrAmmar MagdyNo ratings yet
- The Role of "Eye Platelet Rich Plasma" (E-Prp) For Wound Healing in OphthalmologyDocument9 pagesThe Role of "Eye Platelet Rich Plasma" (E-Prp) For Wound Healing in OphthalmologyJoel OberlinNo ratings yet