You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- 20 - 247Analisis-Profilaksis Primer Perdarahan Varises Gastroesofagus Pada Sirosis Hati-Peranan Penghambat BetaDocument9 pages20 - 247Analisis-Profilaksis Primer Perdarahan Varises Gastroesofagus Pada Sirosis Hati-Peranan Penghambat BetaArga Krittas MaranNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- 1341 1936 1 PBDocument5 pages1341 1936 1 PBHumamuddinNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Law, AbstractDocument1 pageLaw, AbstractHumamuddinNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Health Law Education With The Islamic Transcendental ParadigmDocument8 pagesHealth Law Education With The Islamic Transcendental ParadigmHumamuddinNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Screening For Depression in Cardiac RehaDocument7 pagesScreening For Depression in Cardiac RehaHumamuddinNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Aturan Baru THR 2017 PDFDocument1 pageAturan Baru THR 2017 PDFHumamuddinNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- 2016 Lacroix S Nutrition in CV RehabDocument7 pages2016 Lacroix S Nutrition in CV RehabHumamuddinNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Egusa 2008Document15 pagesEgusa 2008HumamuddinNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Duty Abundance Policy in Puskesmas in Services of BPJS of HealthDocument10 pagesDuty Abundance Policy in Puskesmas in Services of BPJS of HealthHumamuddinNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- Law, AbstractDocument1 pageLaw, AbstractHumamuddinNo ratings yet
- The American Journal of Medicine Volume 123 Issue 3-Supp-S 2010 (Doi 10.1016/j.amjmed.2009.12.006) Sunder Mudaliar; Robert R. Henry - Effects of Incretin Hormones on Β-Cell Mass and Function, BodyDocument9 pagesThe American Journal of Medicine Volume 123 Issue 3-Supp-S 2010 (Doi 10.1016/j.amjmed.2009.12.006) Sunder Mudaliar; Robert R. Henry - Effects of Incretin Hormones on Β-Cell Mass and Function, BodyHumamuddinNo ratings yet
- Aturan Baru THR 2017 PDFDocument1 pageAturan Baru THR 2017 PDFHumamuddinNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Teacher Experience and The Class Size Effect - Experimental EvidenceDocument31 pagesTeacher Experience and The Class Size Effect - Experimental EvidenceHumamuddinNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- What Drives The Reversal of The Gender Education Gap? Evidence From GermanyDocument43 pagesWhat Drives The Reversal of The Gender Education Gap? Evidence From GermanyHumamuddinNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Jurnal Down Syndrome2 PDFDocument8 pagesJurnal Down Syndrome2 PDFHumamuddinNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Metabolisme ProteinDocument10 pagesMetabolisme ProteinJulian HuningkorNo ratings yet
- Jurnal Pneumonia PDFDocument8 pagesJurnal Pneumonia PDFHumamuddin100% (2)
- LampiranSK PPDB IC 2012 GorontaloDocument3 pagesLampiranSK PPDB IC 2012 GorontaloHumamuddinNo ratings yet
- LISTA OFERTA FARMACIAS MARZO 2024Document7 pagesLISTA OFERTA FARMACIAS MARZO 2024pabloo.viedmaNo ratings yet
- Dengue FeverDocument1 pageDengue Feverapi-266482250No ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- What Is Health PromotionDocument5 pagesWhat Is Health Promotionpuskesmas beloNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- WHO / OMS FWC MCA 17.05 EngDocument44 pagesWHO / OMS FWC MCA 17.05 EngsofiabloemNo ratings yet
- Daftar Harga KFTD Sby Per 1 April 2022Document370 pagesDaftar Harga KFTD Sby Per 1 April 2022farmasi psrNo ratings yet
- Who QualityRights Toolkit Docket 2012Document338 pagesWho QualityRights Toolkit Docket 2012Vaishnavi JayakumarNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Tugas PKLDocument91 pagesTugas PKLrhayNo ratings yet
- ACFrOgC7kFmrz7iEnBDL67AiKdbKlFMHl1zSW1zdMlsXgWhOx IxkCP5y O3JMN7QJRXOQ99igj4mtYtTGFSXHHiQ8f1qHodCf9IN9s1svwzyLyJ39fEv2dQeBXju2Y PDFDocument26 pagesACFrOgC7kFmrz7iEnBDL67AiKdbKlFMHl1zSW1zdMlsXgWhOx IxkCP5y O3JMN7QJRXOQ99igj4mtYtTGFSXHHiQ8f1qHodCf9IN9s1svwzyLyJ39fEv2dQeBXju2Y PDFAnis HaerunnisaNo ratings yet
- 2017 - Stockist ObatDocument6 pages2017 - Stockist ObatUrdona Proteksia NezaraNo ratings yet
- 3rd Quarter Reviewer in Mapeh 10Document8 pages3rd Quarter Reviewer in Mapeh 10cali anna100% (3)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- ANEXA1 Lista Medicamente Decontate de CASDocument39 pagesANEXA1 Lista Medicamente Decontate de CASVas RetNo ratings yet
- Alemayehu Tadesse Third Draft Proposal, Alex3 LastDocument37 pagesAlemayehu Tadesse Third Draft Proposal, Alex3 LastZeleke WondimuNo ratings yet
- NPHCDA's Minimum Standards for Primary Healthcare in NigeriaDocument71 pagesNPHCDA's Minimum Standards for Primary Healthcare in NigeriaDaramola BlessingNo ratings yet
- Health Care Systems OverviewDocument177 pagesHealth Care Systems Overviewraina menezesNo ratings yet
- Catalogo 2018 Formas FarmaceuitcasDocument16 pagesCatalogo 2018 Formas FarmaceuitcasYasminNo ratings yet
- The Role of The Government in Economics: Executive SummaryDocument10 pagesThe Role of The Government in Economics: Executive SummaryrojithvNo ratings yet
- Pharmacovigilance Topic 2 CAMDocument9 pagesPharmacovigilance Topic 2 CAMedwin osiyelNo ratings yet
- Anta Assignment SAMPLEDocument3 pagesAnta Assignment SAMPLEMSKCNo ratings yet
- 28-Guidelines For Drinking-Water Quality, Vol. 1, Recommendations (3rd Edition) - WHO-9241546387-Wo PDFDocument541 pages28-Guidelines For Drinking-Water Quality, Vol. 1, Recommendations (3rd Edition) - WHO-9241546387-Wo PDFJai KumarNo ratings yet
- EMHJ - 24 - 3 - 2018 IraqDocument92 pagesEMHJ - 24 - 3 - 2018 Iraqxll21No ratings yet
- Asesmen Awal KeperawatanDocument2 pagesAsesmen Awal Keperawatanyunia pratiwiNo ratings yet
- Kartu StokDocument3 pagesKartu StokRoni Keysa WidjaksonoNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Auto-Disable Syringes What To Look ForDocument8 pagesAuto-Disable Syringes What To Look Forabhi_818No ratings yet
- PPG All Produk Per TGL 16 Feb 2021 FixDocument2,024 pagesPPG All Produk Per TGL 16 Feb 2021 FixAnonymous aaAQ6dgNo ratings yet
- Amitriptili N Acarbose 100: Allopurino LDocument12 pagesAmitriptili N Acarbose 100: Allopurino Lgudang farmasiNo ratings yet
- Stok 060722Document31 pagesStok 060722Joyoboyo PrimaNo ratings yet
- UNIT 9 - ôn tập-đã chuyển đổiDocument4 pagesUNIT 9 - ôn tập-đã chuyển đổiThảo NgaNo ratings yet
- Mothers ' Experiences of Quality of Care and Potential Benefits of Implementing The WHO Safe Childbirth Checklist: A Case Study of Aceh IndonesiaDocument8 pagesMothers ' Experiences of Quality of Care and Potential Benefits of Implementing The WHO Safe Childbirth Checklist: A Case Study of Aceh Indonesialisnawati rahayuNo ratings yet
- Developmental Articles Primary Health Care and Community Based Rehabilitation: Implications For Physical TherapyDocument33 pagesDevelopmental Articles Primary Health Care and Community Based Rehabilitation: Implications For Physical TherapyRaúl Ferrer PeñaNo ratings yet
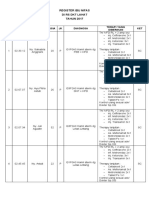
- Register Ibu Nifas 2017Document6 pagesRegister Ibu Nifas 2017jkn rsiampNo ratings yet