You might also like
- Microcirculation in Cardiovascular DiseasesFrom EverandMicrocirculation in Cardiovascular DiseasesEnrico Agabiti-RoseiNo ratings yet
- The Charcot Foot. The British Editorial Society of Bone & Joint Surgery. 2016Document5 pagesThe Charcot Foot. The British Editorial Society of Bone & Joint Surgery. 2016Jose Fernando DiezNo ratings yet
- C PPPP "P P PP# PDocument11 pagesC PPPP "P P PP# PLeni CarununganNo ratings yet
- Jurnal Orto NDocument12 pagesJurnal Orto Ndokter1991No ratings yet
- Christopher W. DiGiovanni ArticleDocument10 pagesChristopher W. DiGiovanni ArticleRajiv NegandhiNo ratings yet
- Killinger 2010Document8 pagesKillinger 2010Andrea TixeNo ratings yet
- Hypertrophic Osteoarthropathy: An Unusual Cause of Knee Pain and Recurrent EffusionDocument3 pagesHypertrophic Osteoarthropathy: An Unusual Cause of Knee Pain and Recurrent EffusionWami FadelNo ratings yet
- Etiology, Pathophysiology andDocument6 pagesEtiology, Pathophysiology andlatifa adluNo ratings yet
- The Diabetic FootDocument12 pagesThe Diabetic FootOliver Vebrian SampelilingNo ratings yet
- Osteoarthritis: in The ClinicDocument16 pagesOsteoarthritis: in The ClinicKurosaki IchigoNo ratings yet
- Jurnal BTKV Edy CLTI 4 FebruariDocument10 pagesJurnal BTKV Edy CLTI 4 FebruarimcvuNo ratings yet
- Effects of Exercise and Physical Activity On Knee OsteoarthritisDocument9 pagesEffects of Exercise and Physical Activity On Knee OsteoarthritisJoseph LimNo ratings yet
- Ankle Fractures in Diabetics: Victor R. Prisk, MD, Dane K. Wukich, MDDocument15 pagesAnkle Fractures in Diabetics: Victor R. Prisk, MD, Dane K. Wukich, MDAnonymous kdBDppigENo ratings yet
- Obesity Inflammation and Endothelial DysDocument8 pagesObesity Inflammation and Endothelial DysgoldNo ratings yet
- Osteonecrosis of The Femoral Head.2Document10 pagesOsteonecrosis of The Femoral Head.2Nitya KrishnaNo ratings yet
- Journal of Clinical & Translational EndocrinologyDocument6 pagesJournal of Clinical & Translational EndocrinologyEka JuliantaraNo ratings yet
- HHS Public Access: Diagnosis and Treatment of Hip and Knee Osteoarthritis: A ReviewDocument25 pagesHHS Public Access: Diagnosis and Treatment of Hip and Knee Osteoarthritis: A ReviewJose PerezNo ratings yet
- Osteoarthritis: OsteoartriteDocument9 pagesOsteoarthritis: OsteoartriteSofia Cerezo MuñozNo ratings yet
- Duque2021 Article OsteosarcopeniaAGeriatricGiantDocument4 pagesDuque2021 Article OsteosarcopeniaAGeriatricGiantVERONICA BARRERANo ratings yet
- Hipertensi 2Document23 pagesHipertensi 2ayunimrsNo ratings yet
- Care of The Patient With Fracture Neck of Femur For Non-Emergency SurgeryDocument7 pagesCare of The Patient With Fracture Neck of Femur For Non-Emergency SurgeryChärlayne Joyce GuzmänNo ratings yet
- OsteoartritisDocument11 pagesOsteoartritisSavira Rizka MeidySNo ratings yet
- Sps 23132Document9 pagesSps 23132TrioRWicaksanaNo ratings yet
- Comparing The Effects of Ultrasound and Microwave Physiotherapy Treatments On Knee Osteoarthritis by MEasuring Osteocalcin Level and Erythrocyte Sedimentation Rate in BloodDocument5 pagesComparing The Effects of Ultrasound and Microwave Physiotherapy Treatments On Knee Osteoarthritis by MEasuring Osteocalcin Level and Erythrocyte Sedimentation Rate in BloodAlfiana ApriliaNo ratings yet
- 1-Disease MechanismsDocument5 pages1-Disease MechanismsMarian Dane PunzalanNo ratings yet
- Evaluation and Treatment of Stage 0 Charcot's Neuroarthropathy of The Foot and AnkleDocument11 pagesEvaluation and Treatment of Stage 0 Charcot's Neuroarthropathy of The Foot and AnkleAnonymous kdBDppigENo ratings yet
- The Diabetic Foot: From Art To Science.Document11 pagesThe Diabetic Foot: From Art To Science.Claudio NogueiraNo ratings yet
- (1479683X - European Journal of Endocrinology) Approach To The Patient With Secondary OsteoporosisDocument12 pages(1479683X - European Journal of Endocrinology) Approach To The Patient With Secondary OsteoporosismeoconmapmapNo ratings yet
- Osteoarthritis-Patterns, Cardio-Metabolic Risk Factors and Risk of All-Cause Mortality: 20 Years Follow-Up in Patients After Hip or Knee ReplacementDocument9 pagesOsteoarthritis-Patterns, Cardio-Metabolic Risk Factors and Risk of All-Cause Mortality: 20 Years Follow-Up in Patients After Hip or Knee Replacementaxl___No ratings yet
- Osteoarthritis Guide: Causes, Symptoms, TreatmentsDocument3 pagesOsteoarthritis Guide: Causes, Symptoms, TreatmentsFrancisco Palma CarvajalNo ratings yet
- American Medical Women's Association Position Paper On OsteoporosisDocument7 pagesAmerican Medical Women's Association Position Paper On OsteoporosisVincent NandoNo ratings yet
- Rajbhandari2002 Article CharcotNeuroarthropathyInDiabe PDFDocument12 pagesRajbhandari2002 Article CharcotNeuroarthropathyInDiabe PDFSaumil ShahNo ratings yet
- FulltextDocument11 pagesFulltextajeet84bhu2920No ratings yet
- Type 1 Diabetes and Osteoporosis A Review of LiteratureDocument8 pagesType 1 Diabetes and Osteoporosis A Review of LiteraturebqvlqjugfNo ratings yet
- Frykberg RG, Et Al. Diabetic Foot Disorders.Document68 pagesFrykberg RG, Et Al. Diabetic Foot Disorders.Jared MalanNo ratings yet
- Osteomyelitis of The Foot in Diabetic Patients: Benjamin A. LipskyDocument9 pagesOsteomyelitis of The Foot in Diabetic Patients: Benjamin A. Lipskyvijay SaxsenaNo ratings yet
- Surg Recon F&ADocument13 pagesSurg Recon F&AJeffNo ratings yet
- Musculo-Skeletal Disorders - Polymalagia ArthritisDocument22 pagesMusculo-Skeletal Disorders - Polymalagia ArthritisKyle J. NortonNo ratings yet
- Cia 15 485Document7 pagesCia 15 485Faradilla PuspitasariNo ratings yet
- The Open Orthopaedics Journal: Adolescent Idiopathic ScoliosisDocument12 pagesThe Open Orthopaedics Journal: Adolescent Idiopathic ScoliosisBecky YuliagustinaNo ratings yet
- Degenerative Joint DiseasesDocument30 pagesDegenerative Joint DiseasesBahaa ShaabanNo ratings yet
- BMJ 2006 p639Document5 pagesBMJ 2006 p639Wahab RasyidNo ratings yet
- Protrusio Acetabuli Diagnosis and TreatmentDocument10 pagesProtrusio Acetabuli Diagnosis and TreatmentFerney Leon BalceroNo ratings yet
- Art Culo SEOM SER SEIOMM SECOT 1657603419Document17 pagesArt Culo SEOM SER SEIOMM SECOT 1657603419Patricia Mestres CampdepadrosNo ratings yet
- Hepatic Osteodystrophy MechanismDocument14 pagesHepatic Osteodystrophy MechanismM.miracleNo ratings yet
- Abrams-2019-The Gout WarsDocument7 pagesAbrams-2019-The Gout WarsNash YoungNo ratings yet
- Osteonecrosis of The Femoral Head: Evaluation and TreatmentDocument10 pagesOsteonecrosis of The Femoral Head: Evaluation and TreatmentHector Ulises Quintanilla SotoNo ratings yet
- Christopher W DiGiovanni Article PDFDocument10 pagesChristopher W DiGiovanni Article PDFStefano Pareschi PasténNo ratings yet
- Perioperative Management of Diabetic Foot: Nune SoghomonyanDocument3 pagesPerioperative Management of Diabetic Foot: Nune SoghomonyanUswatun HasanahNo ratings yet
- Protocolo Clínico e Diretrizes Terapêuticas para Osteoporose no BrasilDocument22 pagesProtocolo Clínico e Diretrizes Terapêuticas para Osteoporose no BrasilDaniNo ratings yet
- The Use of Nanotechnology in Cardiovascular DiseasDocument13 pagesThe Use of Nanotechnology in Cardiovascular DiseasCNo ratings yet
- Lespasio Et Al 2017 Knee Osteoarthritis A PrimerDocument7 pagesLespasio Et Al 2017 Knee Osteoarthritis A PrimerMuhammad MuktiNo ratings yet
- Knee Oa NcbiDocument7 pagesKnee Oa NcbiFitria Dewi LestariNo ratings yet
- OsteoarthritisDocument3 pagesOsteoarthritisVanessa Da CruzNo ratings yet
- OsteoarthritisDocument10 pagesOsteoarthritisGiri PriyaNo ratings yet
- OA JurnalDocument6 pagesOA JurnalAndriani WhyntNo ratings yet
- A Literature Review of Total Hip Arthroplasty in Patients With Ankylosing Spondylitis: Perioperative Considerations and OutcomeDocument7 pagesA Literature Review of Total Hip Arthroplasty in Patients With Ankylosing Spondylitis: Perioperative Considerations and OutcomeSivabharathi SivanandamNo ratings yet
- article2 EUALR CARDIOVASCULAR EVENT ASSOCIATED WITH INITIATING ALLOPURINOL AND FEBUXOSTATDocument1 pagearticle2 EUALR CARDIOVASCULAR EVENT ASSOCIATED WITH INITIATING ALLOPURINOL AND FEBUXOSTATindream81No ratings yet
- OsteoarthritisDocument8 pagesOsteoarthritisErick CalcaligongNo ratings yet
- Risk Factors and Burden of Osteoarthritis: SciencedirectDocument5 pagesRisk Factors and Burden of Osteoarthritis: SciencedirectlindapramusintaNo ratings yet
- Physiology of Pain, Classification and TreatmentDocument40 pagesPhysiology of Pain, Classification and TreatmentTestingAccNo ratings yet
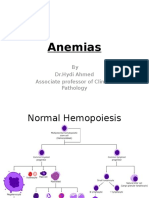
- Anemias (1) by DR - Hydi 3rd MBBS-2016Document63 pagesAnemias (1) by DR - Hydi 3rd MBBS-2016Suban GouseNo ratings yet
- Diabetic Foot Care GuideDocument4 pagesDiabetic Foot Care Guidewjde AlharbeNo ratings yet
- Suplemento 1Document56 pagesSuplemento 1Dessirhe LaraNo ratings yet
- Thesis Reza Salman Roghani PDFDocument76 pagesThesis Reza Salman Roghani PDFscoopyNo ratings yet
- Nursing Vol3 Issue1 Article 4Document9 pagesNursing Vol3 Issue1 Article 4Mark Angelo Picar AbelleraNo ratings yet
- Vitamin B-12 Associated Neurological DiseasesDocument25 pagesVitamin B-12 Associated Neurological DiseasesNitin SainiNo ratings yet
- 43871Document48 pages43871api-266813497No ratings yet
- Toronto Clinical Neuropathy Score and Modified Toronto Clinical Neuropathy Score Diagnostic Tests in Distal Diabetic Sensorimotor Polyneuropathy PatientsDocument10 pagesToronto Clinical Neuropathy Score and Modified Toronto Clinical Neuropathy Score Diagnostic Tests in Distal Diabetic Sensorimotor Polyneuropathy PatientsSurya DharmaNo ratings yet
- Bandolier Topi AniesDocument22 pagesBandolier Topi AniesFrancisco MirettiNo ratings yet
- Nur3111p Professionalism and Lifelong Learning ReflectionDocument6 pagesNur3111p Professionalism and Lifelong Learning Reflectionapi-578141969No ratings yet
- Clinical Fact Sheet PNDocument2 pagesClinical Fact Sheet PNapi-360120287No ratings yet
- Neuropati 1Document73 pagesNeuropati 1Bukhori HamamuraNo ratings yet
- Research Article: Improving The Reliability and Utility of Streptozotocin-Induced Rat Diabetic ModelDocument15 pagesResearch Article: Improving The Reliability and Utility of Streptozotocin-Induced Rat Diabetic ModelSipend AnatomiNo ratings yet
- The Diabetic Foot: From Art To Science.Document11 pagesThe Diabetic Foot: From Art To Science.Claudio NogueiraNo ratings yet
- St. Paul University Nursing Case StudyDocument8 pagesSt. Paul University Nursing Case StudyRoxanne MariÑas DelvoNo ratings yet
- Komplikasi Diabetes (Akut Dan Kronik) : Luh Gede Sri YennyDocument50 pagesKomplikasi Diabetes (Akut Dan Kronik) : Luh Gede Sri YennyArya WinataNo ratings yet
- Cochrane: LibraryDocument36 pagesCochrane: LibraryEeqNo ratings yet
- Diabetes and Nerve Damage: CausesDocument5 pagesDiabetes and Nerve Damage: CausesAntonio A. BonitaNo ratings yet
- Psychosomatic Pain: Ertuğrul AllahverdiDocument20 pagesPsychosomatic Pain: Ertuğrul AllahverdidiasNo ratings yet
- Emg BasicsDocument5 pagesEmg BasicsSantosh DashNo ratings yet
- Diabetic FootDocument22 pagesDiabetic FootNaikko80100% (1)
- Guillain Barre Syndrome-REVISED FINAL Orange2Document108 pagesGuillain Barre Syndrome-REVISED FINAL Orange2Minnie Chavez CardonaNo ratings yet
- Lepra Reactions: Causes, Types and TreatmentDocument24 pagesLepra Reactions: Causes, Types and TreatmentSWAPAN KUMAR SARKAR100% (2)
- Diabetic Neuropathy Treatment Case StudyDocument2 pagesDiabetic Neuropathy Treatment Case Studyjonas1889No ratings yet
- Ultima Cold Laser DeviceDocument2 pagesUltima Cold Laser DeviceullasaaithalNo ratings yet
- Managing Diabetic Foot ProblemsDocument48 pagesManaging Diabetic Foot Problemsanand787No ratings yet
- Paidepally Srinivas RaoDocument9 pagesPaidepally Srinivas RaoShyam KalavalapalliNo ratings yet
- Alpha-Lipoic Acid and Diabetic NeuropathyDocument7 pagesAlpha-Lipoic Acid and Diabetic NeuropathyPedro Rodriguez PicazoNo ratings yet
- Pain Classification and Cancer Pain ManagementDocument50 pagesPain Classification and Cancer Pain ManagementAli Aftab100% (1)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (14)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 3.5 out of 5 stars3.5/5 (2)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (4)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 5 out of 5 stars5/5 (5)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (327)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 3.5 out of 5 stars3.5/5 (33)
- Daniel Kahneman's "Thinking Fast and Slow": A Macat AnalysisFrom EverandDaniel Kahneman's "Thinking Fast and Slow": A Macat AnalysisRating: 3.5 out of 5 stars3.5/5 (130)
- Summary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisFrom EverandSummary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisRating: 5 out of 5 stars5/5 (3)