You might also like
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Cover Kebijakan MutuDocument1 pageCover Kebijakan MutuSeptaPratamaAptNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- PHARMACOLOGY-introDocument18 pagesPHARMACOLOGY-introSeptaPratamaAptNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Principle of Drug ActionDocument15 pagesPrinciple of Drug ActionSeptaPratamaAptNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- PlagiarismDocument33 pagesPlagiarismMahrukh BaigNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Drug AntagonismDocument9 pagesDrug AntagonismSeptaPratamaAptNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
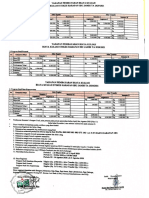
- Biaya Kuliah PMB 2020Document1 pageBiaya Kuliah PMB 2020SeptaPratamaAptNo ratings yet
- Stok Opname 28 Feb (Gudang) - 1Document144 pagesStok Opname 28 Feb (Gudang) - 1SeptaPratamaAptNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Infographic Antimicrobial Resistance 20140430 PDFDocument1 pageInfographic Antimicrobial Resistance 20140430 PDFMarkus AbiogNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Stok Opname 28 Feb (Gudang) - 1Document144 pagesStok Opname 28 Feb (Gudang) - 1SeptaPratamaAptNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Eligible Study Programmes by Partners Final1701191426Document130 pagesEligible Study Programmes by Partners Final1701191426Eko Bayu AjiNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Beta LactamDocument14 pagesBeta LactamSeptaPratamaAptNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Antimicrobial Stewardship PDFDocument37 pagesAntimicrobial Stewardship PDFSeptaPratamaAptNo ratings yet
- Drug Dose Adjustment in Chronic Renal Diseases: Medicine UpdateDocument7 pagesDrug Dose Adjustment in Chronic Renal Diseases: Medicine UpdateSeptaPratamaAptNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Antimicrobial StewardshipDocument37 pagesAntimicrobial StewardshipSeptaPratamaAptNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Ang 2 PDFDocument12 pagesAng 2 PDFSeptaPratamaAptNo ratings yet
- Invoice Septa UnajaDocument1 pageInvoice Septa UnajaSeptaPratamaAptNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- I Don't KnowDocument1 pageI Don't KnowSeptaPratamaAptNo ratings yet
- E1304amcp - 11.15.13 Final JMCP VersionDocument22 pagesE1304amcp - 11.15.13 Final JMCP VersionSeptaPratamaAptNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Probiotics For Prevention of Necrotizing Enterocolitis in Preterm Infants - AlFaleh, K - 2014 - Cochrane Library PDFDocument19 pagesProbiotics For Prevention of Necrotizing Enterocolitis in Preterm Infants - AlFaleh, K - 2014 - Cochrane Library PDFSeptaPratamaAptNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- E1304amcp - 11.15.13 Final JMCP VersionDocument22 pagesE1304amcp - 11.15.13 Final JMCP VersionSeptaPratamaAptNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Drug-Induced Nephrotoxicity: Cynthia A. Naughton, Pharmd, BCPS, North Dakota State University College of PharmacyDocument8 pagesDrug-Induced Nephrotoxicity: Cynthia A. Naughton, Pharmd, BCPS, North Dakota State University College of PharmacyAbdur Rachman Ba'abdullahNo ratings yet
- Order Obat 2Document4 pagesOrder Obat 2SeptaPratamaAptNo ratings yet
- 3rd LabDocument47 pages3rd LabUmair GulzarNo ratings yet
- No. 018/UGM/OGV/EP/XIX/2017: AIESEC in Universitas Gadjah MadaDocument2 pagesNo. 018/UGM/OGV/EP/XIX/2017: AIESEC in Universitas Gadjah MadaSeptaPratamaAptNo ratings yet
- Itinerary Visit ParisDocument1 pageItinerary Visit ParisSeptaPratamaAptNo ratings yet
- SSM Application SummaryDocument61 pagesSSM Application SummarySeptaPratamaAptNo ratings yet
- 1 s2.0 S0378427416329381 MainDocument1 page1 s2.0 S0378427416329381 MainSeptaPratamaAptNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- WHO - Indoor Air PollutionDocument484 pagesWHO - Indoor Air PollutionCosmo Deus100% (2)
- Denah ApotekDocument1 pageDenah ApotekSeptaPratamaAptNo ratings yet
- Cervical Changes During Menstrual Cycle (Photos)Document9 pagesCervical Changes During Menstrual Cycle (Photos)divyanshu kumarNo ratings yet
- Dysfunctional Uterine Bleeding (DUB)Document1 pageDysfunctional Uterine Bleeding (DUB)Bheru LalNo ratings yet
- Untitled Form - Google Forms00Document3 pagesUntitled Form - Google Forms00Ericka Rivera SantosNo ratings yet
- JAR Part 66 Examination Mod 03Document126 pagesJAR Part 66 Examination Mod 03Shreyas PingeNo ratings yet
- Rifle Threat Performance Matrix: SeriesDocument1 pageRifle Threat Performance Matrix: SeriesKuhnNo ratings yet
- BrainPOP Nutrition Quiz242342Document1 pageBrainPOP Nutrition Quiz242342MathableNo ratings yet
- Ideal Discharge Elderly PatientDocument3 pagesIdeal Discharge Elderly PatientFelicia Risca RyandiniNo ratings yet
- Non-Binary or Genderqueer GendersDocument9 pagesNon-Binary or Genderqueer GendersJuan SerranoNo ratings yet
- JOHARI Window WorksheetDocument2 pagesJOHARI Window WorksheetAnonymous j9lsM2RBaINo ratings yet
- Sample Quantitative Descriptive Paper 1Document20 pagesSample Quantitative Descriptive Paper 1oishimontrevanNo ratings yet
- MPSI OverviewDocument15 pagesMPSI OverviewZaqee AlvaNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Project Report On MKT Segmentation of Lux SoapDocument25 pagesProject Report On MKT Segmentation of Lux Soapsonu sahNo ratings yet
- Big Elephants Are Useful Mnemonics & IdiomsDocument144 pagesBig Elephants Are Useful Mnemonics & IdiomsNachoAndrésLlorente100% (1)
- Differential Partitioning of Betacyanins and Betaxanthins Employing Aqueous Two Phase ExtractionDocument8 pagesDifferential Partitioning of Betacyanins and Betaxanthins Employing Aqueous Two Phase ExtractionPaul Jefferson Flores HurtadoNo ratings yet
- BATES CH 6 The Thorax and LungsDocument2 pagesBATES CH 6 The Thorax and LungsAngelica Mae Dela CruzNo ratings yet
- Culturally Safe Classroom Context PDFDocument2 pagesCulturally Safe Classroom Context PDFdcleveland1706No ratings yet
- Stress Relieving, Normalising and Annealing: Datasheet For Non-Heat-TreatersDocument2 pagesStress Relieving, Normalising and Annealing: Datasheet For Non-Heat-TreatersGani PateelNo ratings yet
- Ott OTT Ecolog 1000 Water Level LoggerDocument3 pagesOtt OTT Ecolog 1000 Water Level LoggerNedimZ1No ratings yet
- Sialoree BotoxDocument5 pagesSialoree BotoxJocul DivinNo ratings yet
- Mrunal Handout 12 CSP20Document84 pagesMrunal Handout 12 CSP20SREEKANTHNo ratings yet
- Gut Health Elimination Diet Meal Plan FINALDocument9 pagesGut Health Elimination Diet Meal Plan FINALKimmy BathamNo ratings yet
- Biography of Murray (1893-1988) : PersonologyDocument6 pagesBiography of Murray (1893-1988) : PersonologyMing100% (1)
- Anatomy and Physiology Chapter 2Document28 pagesAnatomy and Physiology Chapter 2Marshalee FrancisNo ratings yet
- Easy Rasam Recipe Made Without Rasam PowderDocument6 pagesEasy Rasam Recipe Made Without Rasam PowderPrantik Adhar SamantaNo ratings yet
- Senior Cohousing - Sherry Cummings, Nancy P. KropfDocument86 pagesSenior Cohousing - Sherry Cummings, Nancy P. KropfAnastasia JoannaNo ratings yet
- UntitledDocument18 pagesUntitledSpace HRNo ratings yet
- Dirty Dozen List of Endocrine DisruptorsDocument4 pagesDirty Dozen List of Endocrine DisruptorsMariuszNo ratings yet
- SPKT Thiet Ke Co Khi 1Document33 pagesSPKT Thiet Ke Co Khi 1Chiến PhanNo ratings yet
- SpectraSensors TDL Analyzers in RefineriesDocument8 pagesSpectraSensors TDL Analyzers in Refineries1977specopsNo ratings yet
- Labor EstimateDocument26 pagesLabor EstimateAngelica CabreraNo ratings yet