You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Cheat Sheet RevisedDocument2 pagesCheat Sheet RevisedUSC Upstate Nursing Coaches100% (3)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Musculoskeletal ProblemsDocument12 pagesMusculoskeletal ProblemsUSC Upstate Nursing CoachesNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Sulfonylurea Agents (Diabinese, Glucotrol, Diabeta) : 2. Meglitinide Analogues (Prandin)Document11 pagesSulfonylurea Agents (Diabinese, Glucotrol, Diabeta) : 2. Meglitinide Analogues (Prandin)Kristin EdwardsNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Assessment of Hematologic Disorders: Patient HistoryDocument3 pagesAssessment of Hematologic Disorders: Patient HistoryUSC Upstate Nursing CoachesNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Memory Pics Hematology OncologyDocument28 pagesMemory Pics Hematology OncologyKristin EdwardsNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
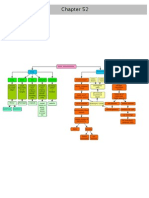
- Chapter 52 Bone ClassificationsDocument1 pageChapter 52 Bone ClassificationsUSC Upstate Nursing CoachesNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Assessment of Hematologic Disorders - Physical AssessmentDocument3 pagesAssessment of Hematologic Disorders - Physical AssessmentUSC Upstate Nursing CoachesNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Compilation of Class 10.26.10Document13 pagesCompilation of Class 10.26.10USC Upstate Nursing CoachesNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Ch. 52 Musculoskeletal AssessmentDocument28 pagesCh. 52 Musculoskeletal AssessmentUSC Upstate Nursing CoachesNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- Chapter 41 Hematologic ProblemsDocument6 pagesChapter 41 Hematologic ProblemsUSC Upstate Nursing CoachesNo ratings yet
- Lupus, Sclerosis, Lymes, Fibromyalgia GoutDocument2 pagesLupus, Sclerosis, Lymes, Fibromyalgia GoutUSC Upstate Nursing CoachesNo ratings yet
- Memory Pics: MusculoskeletalDocument17 pagesMemory Pics: MusculoskeletalUSC Upstate Nursing CoachesNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Memory Pics: NeurologicalDocument12 pagesMemory Pics: NeurologicalUSC Upstate Nursing CoachesNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- CH 54 AmputationsDocument12 pagesCH 54 AmputationsUSC Upstate Nursing CoachesNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Memory Pics: RenalDocument8 pagesMemory Pics: RenalUSC Upstate Nursing CoachesNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Assessment of The Hematologic SystemDocument36 pagesAssessment of The Hematologic SystemUSC Upstate Nursing CoachesNo ratings yet
- Memory Pics: SensoryDocument12 pagesMemory Pics: SensoryUSC Upstate Nursing CoachesNo ratings yet
- Chapter 21Document4 pagesChapter 21USC Upstate Nursing CoachesNo ratings yet
- Chapter 19Document6 pagesChapter 19USC Upstate Nursing CoachesNo ratings yet
- CH 53: Musculoskeletal Problems (Per Amendolair)Document32 pagesCH 53: Musculoskeletal Problems (Per Amendolair)USC Upstate Nursing CoachesNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Immunity & Cancer (Spartanburg)Document17 pagesImmunity & Cancer (Spartanburg)USC Upstate Nursing CoachesNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Interventions For Clients With Hematologic ProblemsDocument50 pagesInterventions For Clients With Hematologic ProblemsUSC Upstate Nursing CoachesNo ratings yet
- Male Reproductive ProblemsDocument6 pagesMale Reproductive ProblemsUSC Upstate Nursing CoachesNo ratings yet
- CH 52: Musculoskeletal Assessment (Per Amendolair)Document27 pagesCH 52: Musculoskeletal Assessment (Per Amendolair)USC Upstate Nursing CoachesNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- White Blood Cells (WBC) TotalDocument1 pageWhite Blood Cells (WBC) TotalUSC Upstate Nursing CoachesNo ratings yet
- CH 54: Musculoskeletal Trauma (Per Amendolair)Document54 pagesCH 54: Musculoskeletal Trauma (Per Amendolair)USC Upstate Nursing CoachesNo ratings yet
- CH 41: Hematological Assessment (Per Amendolair)Document28 pagesCH 41: Hematological Assessment (Per Amendolair)USC Upstate Nursing CoachesNo ratings yet
- Chapter 22: Crossword (Per Black)Document3 pagesChapter 22: Crossword (Per Black)USC Upstate Nursing CoachesNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Fatigue: Symptom Tiredness Lethargy SleepDocument10 pagesFatigue: Symptom Tiredness Lethargy Sleepjohnjoseph4069No ratings yet
- Panic Attacks PDFDocument8 pagesPanic Attacks PDFluis_violinosNo ratings yet
- Epidemiology of Diabetes MellitusDocument5 pagesEpidemiology of Diabetes Mellitusarkanthos77No ratings yet
- End Stage Renal Disease Case StudyDocument8 pagesEnd Stage Renal Disease Case StudyNikko Dela CruzNo ratings yet
- Health - ALL ABT STRESSSSSSSSSDocument10 pagesHealth - ALL ABT STRESSSSSSSSSDennise Adrianne OfarilNo ratings yet
- Cardiology Workshop HighlightsDocument32 pagesCardiology Workshop HighlightsChristabella Natalia WijayaNo ratings yet
- Primary HyperparathyroidismDocument5 pagesPrimary HyperparathyroidismAbdul QuyyumNo ratings yet
- Carcinosin: A Clinical and Pathogenetic Study of the NosodeDocument11 pagesCarcinosin: A Clinical and Pathogenetic Study of the NosodeSohail LatifNo ratings yet
- Undergraduate Medicine Study Notes PDFDocument764 pagesUndergraduate Medicine Study Notes PDFSHAKEEL1991No ratings yet
- Maloy, Katherine - A Case-Based Approach To Emergency Psychiatry-Oxford University Press (2016)Document225 pagesMaloy, Katherine - A Case-Based Approach To Emergency Psychiatry-Oxford University Press (2016)Cristina Lefter100% (1)
- Question Chapter 6 Cerebellum and Its ConnectionsDocument13 pagesQuestion Chapter 6 Cerebellum and Its ConnectionsTrang BuiNo ratings yet
- Free Closed Door Coaching Prof Arconado - Microbiology - 200 Items Key PDFDocument14 pagesFree Closed Door Coaching Prof Arconado - Microbiology - 200 Items Key PDFAnne MorenoNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Hypnotism MesmerismDocument32 pagesHypnotism MesmerismMuthu KumarNo ratings yet
- The Water CureDocument5 pagesThe Water Curezaheer intdirectorNo ratings yet
- Thalamic Stroke and BehaviourDocument9 pagesThalamic Stroke and BehaviourparkdhingraNo ratings yet
- Introduction To Medical Surgical Nursing 5th Edition Linton Solutions ManualDocument4 pagesIntroduction To Medical Surgical Nursing 5th Edition Linton Solutions ManualJoannaBarnettcfixjNo ratings yet
- Isosorbide Mononitrate: Adult: PO Regular Release (ISMO, Monoket) 20 MG B.I.D. 7 H ApartDocument2 pagesIsosorbide Mononitrate: Adult: PO Regular Release (ISMO, Monoket) 20 MG B.I.D. 7 H ApartAubrey Unique EvangelistaNo ratings yet
- HyperthyroidismDocument4 pagesHyperthyroidismavinash dhameriyaNo ratings yet
- NCP Liver CirrhosisDocument7 pagesNCP Liver CirrhosisIris Jimenez-BuanNo ratings yet
- Case Study About Hypertension With Electrolyte Imbalance Part 3Document2 pagesCase Study About Hypertension With Electrolyte Imbalance Part 3THE NURSING CORNERS100% (1)
- DrugsDocument18 pagesDrugsdantacNo ratings yet
- Varaha Mihira's Sarvato Bhadra ChakraDocument59 pagesVaraha Mihira's Sarvato Bhadra ChakraRohith6No ratings yet
- Music TherapyDocument13 pagesMusic TherapyXavier KiranNo ratings yet
- Moon in 12 HouseDocument5 pagesMoon in 12 HouseastroparamNo ratings yet
- Medical MarijuanaDocument4 pagesMedical MarijuanaDanielZepedaPereaNo ratings yet
- Parakeet RingneckDocument2 pagesParakeet RingneckAhmer KhanNo ratings yet
- Bleeding Disorders: Coagulopathy (Also Called Clotting Disorder and Bleeding DisorderDocument5 pagesBleeding Disorders: Coagulopathy (Also Called Clotting Disorder and Bleeding DisorderAyisha EdwinNo ratings yet
- BMI PresentationDocument25 pagesBMI PresentationJenny Bolesa BarrerasNo ratings yet
- MastitisDocument4 pagesMastitisAshleigh Johnstone100% (2)
- TIBBDocument25 pagesTIBBtakwaniaNo ratings yet