You might also like
- The Lemonade Diet Ingredients and Recipe PDFDocument14 pagesThe Lemonade Diet Ingredients and Recipe PDFTradingTheEdges100% (3)
- Tracheostomy Operating TechniqueDocument34 pagesTracheostomy Operating TechniqueIsa BasukiNo ratings yet
- How I Stopped SweatingDocument14 pagesHow I Stopped Sweatingscribd_acount01No ratings yet
- Total LaryngectomyDocument15 pagesTotal LaryngectomyKumaran Bagavathi RagavanNo ratings yet
- Tendon InjuriesDocument48 pagesTendon InjuriesdiasNo ratings yet
- Sullivan's Interpersonal Model of Personality DevelopmentDocument42 pagesSullivan's Interpersonal Model of Personality DevelopmentPamDavidGabriel75% (4)
- Midterm Leadership and Management (MCN 107) EXAMDocument26 pagesMidterm Leadership and Management (MCN 107) EXAMsophi30100% (1)
- Activity Intolerance (NCP)Document3 pagesActivity Intolerance (NCP)Sonia Letran Singson100% (3)
- Aaos Elbow Surgical Approaches-1Document9 pagesAaos Elbow Surgical Approaches-1Mossa SultanyNo ratings yet
- Laryngofissure TechniqueDocument5 pagesLaryngofissure TechniqueJamesNo ratings yet
- Thoracotomy Through The Auscultatory Triangle - Ann Thorac Surg.1989Document2 pagesThoracotomy Through The Auscultatory Triangle - Ann Thorac Surg.1989Adriana PavelNo ratings yet
- Thoracotomy Through The Auscultatory Triangle: HorowitzDocument2 pagesThoracotomy Through The Auscultatory Triangle: HorowitzRadioputro WicaksonoNo ratings yet
- Median Sternotomy ProcedureDocument5 pagesMedian Sternotomy ProcedureNelly NehNo ratings yet
- Reoperative Cardiac Surgery - Part II: Heart Surgery Forum April 2018Document9 pagesReoperative Cardiac Surgery - Part II: Heart Surgery Forum April 2018David RamirezNo ratings yet
- Percutaneous Tracheostomy: A Comprehensive Review.Document11 pagesPercutaneous Tracheostomy: A Comprehensive Review.Hitomi-No ratings yet
- Technique: Median Sternotomy - Gold Standard Incision For Cardiac SurgeonsDocument8 pagesTechnique: Median Sternotomy - Gold Standard Incision For Cardiac SurgeonsRobert ChristevenNo ratings yet
- TracheostomyDocument10 pagesTracheostomyanitaabreu123No ratings yet
- The First Dorsal Metacarpal Propeller Perforator FDMP Flap For Finger ReconstructionDocument5 pagesThe First Dorsal Metacarpal Propeller Perforator FDMP Flap For Finger ReconstructionSunderraj EllurNo ratings yet
- Judet QuadricepsplastyDocument4 pagesJudet QuadricepsplastyRakesh Kumar100% (1)
- Tracheostomy: As. Univ. Dr. Andrei Cristian Bobocea As. Univ. Dr. Serban Radu MatacheDocument21 pagesTracheostomy: As. Univ. Dr. Andrei Cristian Bobocea As. Univ. Dr. Serban Radu MatacheIoana VasileNo ratings yet
- TracheostomyDocument8 pagesTracheostomyShar CatedralNo ratings yet
- Anesthesia.: Baltimore, MDDocument9 pagesAnesthesia.: Baltimore, MDJaime VasquezNo ratings yet
- Surgical Removal of Spinal Tumors: Article by James Willey, Cst/Cfa, and Mark V. Iarkins, M DDocument8 pagesSurgical Removal of Spinal Tumors: Article by James Willey, Cst/Cfa, and Mark V. Iarkins, M DLuwiNo ratings yet
- 2009 Reconstruccion DiafragmaDocument5 pages2009 Reconstruccion DiafragmaJavier VegaNo ratings yet
- Tracheostomy PDFDocument8 pagesTracheostomy PDFVeronica GaticaNo ratings yet
- Deltopectoral ApproachDocument4 pagesDeltopectoral ApproachAlex DiconiNo ratings yet
- Tracheostomy 191224152833Document106 pagesTracheostomy 191224152833Dimas SevantoNo ratings yet
- Secondary Flexor RepairDocument10 pagesSecondary Flexor RepairŠišmišova DevojkaNo ratings yet
- Tracheal TraumaDocument3 pagesTracheal TraumaWalid DarwicheNo ratings yet
- 10 20515-Otd 97205-190634Document6 pages10 20515-Otd 97205-190634majanga johnNo ratings yet
- Thoracodorsal Artery Perforator Flap (TAP Flap)Document1 pageThoracodorsal Artery Perforator Flap (TAP Flap)Consultorio Cirurgia plásticaNo ratings yet
- 2011 FIRMIN Autologous Ear ReconstructionDocument8 pages2011 FIRMIN Autologous Ear ReconstructionDimitris RodriguezNo ratings yet
- Raza 2017Document7 pagesRaza 2017Robert ChristevenNo ratings yet
- 5.2 Thoracotomy EmergencyDocument28 pages5.2 Thoracotomy Emergencytepat rshsNo ratings yet
- The Deltopectoral FlapDocument10 pagesThe Deltopectoral FlapR KNo ratings yet
- The First Dorsal Metacarpal Artery Flap Family: A ReviewDocument5 pagesThe First Dorsal Metacarpal Artery Flap Family: A ReviewAry YounusNo ratings yet
- Arthrodesis Visualbee2 140217084354 Phpapp02Document56 pagesArthrodesis Visualbee2 140217084354 Phpapp02Monem ShakeerNo ratings yet
- Traqueostomia - Cirugia Minimamente InvasivaDocument8 pagesTraqueostomia - Cirugia Minimamente InvasivaStefani AtlleNo ratings yet
- Hamdi, JPRAS2006Document9 pagesHamdi, JPRAS2006Zouzou YuNo ratings yet
- Primary Thumb Reconstruction in A Mutilated HandDocument13 pagesPrimary Thumb Reconstruction in A Mutilated HandLuciano RuizNo ratings yet
- Tibial Fractures Useful Plastering Technique: MethodDocument4 pagesTibial Fractures Useful Plastering Technique: MethodgregraynerNo ratings yet
- Voices Uchicago Edu-LarynxDocument5 pagesVoices Uchicago Edu-LarynxAhmed KhalidNo ratings yet
- Gibson Et Al-2012-Transforaminal Endoscopic Spinal SurgeryDocument7 pagesGibson Et Al-2012-Transforaminal Endoscopic Spinal SurgeryjuanguapoNo ratings yet
- Annrcse01509 0sutureDocument3 pagesAnnrcse01509 0sutureNichole Audrey SaavedraNo ratings yet
- Thoracic IncisionsDocument10 pagesThoracic IncisionsRadioputro WicaksonoNo ratings yet
- Open Access Atlas of Otolaryngology, Head & Neck Operative SurgeryDocument16 pagesOpen Access Atlas of Otolaryngology, Head & Neck Operative SurgeryMihai Ionut TanaseNo ratings yet
- Thoracic Incisions PDFDocument14 pagesThoracic Incisions PDFalbimar239512No ratings yet
- Jena 2015Document3 pagesJena 2015amdreyNo ratings yet
- Cricothyroidotomy and Needle CricothyrotomyDocument10 pagesCricothyroidotomy and Needle CricothyrotomykityamuwesiNo ratings yet
- Cricothyroidotomy and Needle CricothyrotomyDocument10 pagesCricothyroidotomy and Needle CricothyrotomyDANDYNo ratings yet
- Pleurectomy Through The Triangle of Auscultation: ThoraxDocument2 pagesPleurectomy Through The Triangle of Auscultation: ThoraxRifka WidianingrumNo ratings yet
- TracheostomyDocument3 pagesTracheostomyJon AsuncionNo ratings yet
- Thoracotomy GuidelinesDocument9 pagesThoracotomy GuidelinesMuhammad Hassan RazaNo ratings yet
- Temporal Bone Resection: Brian Ho, MD, C. Arturo Solares, MD, FACS, Benedict Panizza, MBBS, MBA, FRACSDocument5 pagesTemporal Bone Resection: Brian Ho, MD, C. Arturo Solares, MD, FACS, Benedict Panizza, MBBS, MBA, FRACSAyuAnatrieraNo ratings yet
- Tactical Combat Casualty Care (TCCC) Guidelines: 25 January 2024Document17 pagesTactical Combat Casualty Care (TCCC) Guidelines: 25 January 2024Willans Eduardo Rosha HumerezNo ratings yet
- Quaba FlpaDocument3 pagesQuaba FlpaSyed WaheduzzamanNo ratings yet
- Full Endoscopic Bilateral Over The Top Decompression in LumbarDocument6 pagesFull Endoscopic Bilateral Over The Top Decompression in Lumbarckilincer2No ratings yet
- Finger Amputations: Aviram M. Giladi and Kevin C. ChungDocument12 pagesFinger Amputations: Aviram M. Giladi and Kevin C. ChungREM biusNo ratings yet
- Peroneal CompartmentDocument7 pagesPeroneal CompartmentAntonio ANo ratings yet
- Lambou Delto PectoralDocument9 pagesLambou Delto PectoralalexNo ratings yet
- 05 - Thoracic Cavity Lab - NZFDocument42 pages05 - Thoracic Cavity Lab - NZFRolin KhatibNo ratings yet
- Venopuncion y PitagorasDocument2 pagesVenopuncion y PitagorasLucas EliasNo ratings yet
- Posterior Interosseous Artery Flap For Hand Defects: Original ArticleDocument3 pagesPosterior Interosseous Artery Flap For Hand Defects: Original ArticleKristina DewiNo ratings yet
- Difficult Acute Cholecystitis: Treatment and Technical IssuesFrom EverandDifficult Acute Cholecystitis: Treatment and Technical IssuesNo ratings yet
- A Manual of the Operations of Surgery: For the Use of Senior Students, House Surgeons, and Junior PractitionersFrom EverandA Manual of the Operations of Surgery: For the Use of Senior Students, House Surgeons, and Junior PractitionersNo ratings yet
- Lessons in Ornamental Penmanship (Part 1)Document6 pagesLessons in Ornamental Penmanship (Part 1)icen00bNo ratings yet
- Lessons in Ornamental Penmanship (Part 2)Document5 pagesLessons in Ornamental Penmanship (Part 2)icen00bNo ratings yet
- Practical Algorithms To Rank Necklaces, Lyndon Words, and de Bruijn SequencesDocument19 pagesPractical Algorithms To Rank Necklaces, Lyndon Words, and de Bruijn Sequencesicen00bNo ratings yet
- Efficient Constructions of The Prefer-Same and Prefer-Opposite de Bruijn SequencesDocument28 pagesEfficient Constructions of The Prefer-Same and Prefer-Opposite de Bruijn Sequencesicen00bNo ratings yet
- 1183497876Document6 pages1183497876icen00bNo ratings yet
- A Surprisingly Simple de Bruijn Sequence Construction: Discrete Mathematics January 2016Document8 pagesA Surprisingly Simple de Bruijn Sequence Construction: Discrete Mathematics January 2016icen00bNo ratings yet
- A Fast Algorithm To Generate Necklaces With &xed Content: 2003 Elsevier Science B.V. All Rights ReservedDocument13 pagesA Fast Algorithm To Generate Necklaces With &xed Content: 2003 Elsevier Science B.V. All Rights Reservedicen00bNo ratings yet
- On Greedy Algorithms For Binary de Bruijn SequencesDocument22 pagesOn Greedy Algorithms For Binary de Bruijn Sequencesicen00bNo ratings yet
- On Arc-Disjoint Hamiltonian Cycles in de Bruijn Graphs: March 2010Document6 pagesOn Arc-Disjoint Hamiltonian Cycles in de Bruijn Graphs: March 2010icen00bNo ratings yet
- De-Bruijn Sequence and Application in Graph Theory.: Ashish KumarDocument14 pagesDe-Bruijn Sequence and Application in Graph Theory.: Ashish Kumaricen00bNo ratings yet
- Theoretical Computer Science: Abbas Alhakim, Evan Sala, Joe SawadaDocument5 pagesTheoretical Computer Science: Abbas Alhakim, Evan Sala, Joe Sawadaicen00bNo ratings yet
- 8.5 Infusion of Hypertonic Mannitol Solutions: Fluid PhysiologyDocument2 pages8.5 Infusion of Hypertonic Mannitol Solutions: Fluid Physiologyicen00bNo ratings yet
- Journal of Computer and System Sciences: Bastien Cazaux, Thierry Lecroq, Eric RivalsDocument19 pagesJournal of Computer and System Sciences: Bastien Cazaux, Thierry Lecroq, Eric Rivalsicen00bNo ratings yet
- Qualifications in Level 3 Adult Offer Jan21 UpdateDocument103 pagesQualifications in Level 3 Adult Offer Jan21 Updateicen00bNo ratings yet
- EobWUGTuSM2G1lBk7pjNMw Template Analytical Skills TableDocument1 pageEobWUGTuSM2G1lBk7pjNMw Template Analytical Skills Tableicen00bNo ratings yet
- Fluid Physiology 8.2 Infusion of Hypertonic SalineDocument2 pagesFluid Physiology 8.2 Infusion of Hypertonic Salineicen00bNo ratings yet
- 1332417353-QA326 Thromboprophylaxis Body Weight1Document4 pages1332417353-QA326 Thromboprophylaxis Body Weight1icen00bNo ratings yet
- Calcium Channel Blocker Formulary Review 24 June 14Document6 pagesCalcium Channel Blocker Formulary Review 24 June 14icen00bNo ratings yet
- Christian Lorenz Scheurer: The Techniques ofDocument3 pagesChristian Lorenz Scheurer: The Techniques oficen00bNo ratings yet
- Axillary Artery and Vein Cannulation 2015Document4 pagesAxillary Artery and Vein Cannulation 2015icen00bNo ratings yet
- Creating Mattes: Tips N TricksDocument3 pagesCreating Mattes: Tips N Tricksicen00bNo ratings yet
- Color Matching: Tips & TricksDocument4 pagesColor Matching: Tips & Tricksicen00bNo ratings yet
- Blending Ideas: Tips & TricksDocument4 pagesBlending Ideas: Tips & Tricksicen00bNo ratings yet
- Understanding Diagnostic Plots For Linear Regression AnalysisDocument5 pagesUnderstanding Diagnostic Plots For Linear Regression Analysisicen00bNo ratings yet
- PTP Form FinalDocument7 pagesPTP Form FinalRiaCapNo ratings yet
- Theophylline by DP 307 936,933,946,956Document10 pagesTheophylline by DP 307 936,933,946,956Muhammad AbdullahNo ratings yet
- Accumulation of Nitrate in Vegetables and Its Possible Implications To Human HealthDocument10 pagesAccumulation of Nitrate in Vegetables and Its Possible Implications To Human HealthJesus David Calderon GomezNo ratings yet
- HyperthermiaDocument3 pagesHyperthermiaSäbïná D. GabätöNo ratings yet
- Microcytic Anemia PDFDocument8 pagesMicrocytic Anemia PDFMargarita TorresNo ratings yet
- Dyes Ep Mar04 NallapatiDocument6 pagesDyes Ep Mar04 Nallapativiky26No ratings yet
- Gedesnii TugjrelDocument40 pagesGedesnii TugjrelSaibo BoldsaikhanNo ratings yet
- UTSDocument8 pagesUTSMikaela LozanoNo ratings yet
- INDIBEH 1 - ReviewerDocument4 pagesINDIBEH 1 - Reviewereinstein metrilloNo ratings yet
- Mag Ray Instruction ManualDocument7 pagesMag Ray Instruction Manualdigitaltext0% (1)
- Angina Pectoris (Stable Angina) Nursing Care Management - Study GuideDocument8 pagesAngina Pectoris (Stable Angina) Nursing Care Management - Study GuideSachin Singh100% (1)
- The Prevention and Cure Effects of Aspirin Eugenol Ester On Hyperlipidemia and Its MetabonomicsDocument108 pagesThe Prevention and Cure Effects of Aspirin Eugenol Ester On Hyperlipidemia and Its MetabonomicsKavisa GhoshNo ratings yet
- Incision SitesDocument4 pagesIncision SitesmidskiescreamzNo ratings yet
- Iaedp Research Summaries 3 FinalDocument6 pagesIaedp Research Summaries 3 Finalapi-250253869No ratings yet
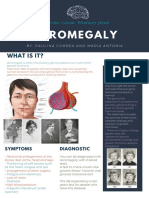
- Acromegaly: What Is It?Document1 pageAcromegaly: What Is It?Paulina CorreaaNo ratings yet
- EOE1 01 Rev A Radiation Therapy An OverviewDocument7 pagesEOE1 01 Rev A Radiation Therapy An OverviewsoraNo ratings yet
- Main - Factsheet Tacrolimus OintmentDocument4 pagesMain - Factsheet Tacrolimus OintmentSakuranbochanNo ratings yet
- 2013 SC Decisions PDFDocument520 pages2013 SC Decisions PDFInes Hamoy JunioNo ratings yet
- Overcome ShynessDocument3 pagesOvercome ShynessLM CuestaNo ratings yet
- This Study Is Currently Recruiting Participants.: SponsorDocument6 pagesThis Study Is Currently Recruiting Participants.: SponsorAalpesh KachhadiyaNo ratings yet
- Speaking Test Avcn 1: Unit 1: Hospital StaffDocument5 pagesSpeaking Test Avcn 1: Unit 1: Hospital StaffHoàng Huy NguyễnNo ratings yet
- Nutrisi and ObesityDocument35 pagesNutrisi and ObesityDeta Meila PutriNo ratings yet
- Sand Brochure July 2016Document2 pagesSand Brochure July 2016Jack CianfaglioneNo ratings yet
- Positive Symptoms Negative Symptoms Cognitive Symptoms: SchizophreniaDocument5 pagesPositive Symptoms Negative Symptoms Cognitive Symptoms: SchizophreniaAisyah BurhanNo ratings yet
- Aspen Vs EspenDocument3 pagesAspen Vs EspeninoesienaNo ratings yet