You might also like
- 4 Oral Cavity ProceduresDocument10 pages4 Oral Cavity ProceduresAnne MarieNo ratings yet
- Soft tissue closure techniques for oroantral communicationsDocument9 pagesSoft tissue closure techniques for oroantral communicationsLalo DmNo ratings yet
- Ijomi 15 415Document4 pagesIjomi 15 415Bagis Emre GulNo ratings yet
- Paladar 03Document8 pagesPaladar 03Marlon MartinezNo ratings yet
- CX PLAST PERIO Functional and Esthetic Outcome Enhancement of Periodontal Surgery by ApplicationDocument8 pagesCX PLAST PERIO Functional and Esthetic Outcome Enhancement of Periodontal Surgery by ApplicationV y M Grupo EspecialistaNo ratings yet
- Principles_of_Flaps,_Suturing_and_Management_of_difficult_extractionDocument14 pagesPrinciples_of_Flaps,_Suturing_and_Management_of_difficult_extractionSRO oONo ratings yet
- 1 s2.0 S0011853222001604 MainDocument20 pages1 s2.0 S0011853222001604 MainDANTE DELEGUERYNo ratings yet
- Vestibuloplasty: Related TermsDocument29 pagesVestibuloplasty: Related Termsمظفر منعم ميران عباسNo ratings yet
- The Palatal Advanced Flap: A Pedicle Flap For Primary Coverage of Immediately Placed ImplantsDocument7 pagesThe Palatal Advanced Flap: A Pedicle Flap For Primary Coverage of Immediately Placed ImplantsMárcia ChatelieNo ratings yet
- Ebook ProstoDocument20 pagesEbook Prostofachira rusdiNo ratings yet
- Soft Tissues Remodeling Technique As A N PDFDocument12 pagesSoft Tissues Remodeling Technique As A N PDFjorgeNo ratings yet
- Practical Applications: Decision Making in Gingival Recession Treatment: Scientific Evidence and Clinical ExperienceDocument12 pagesPractical Applications: Decision Making in Gingival Recession Treatment: Scientific Evidence and Clinical ExperienceAlexa LoyaNo ratings yet
- Asianrhinoplasty: Dean M. Toriumi,, Colin D. PeroDocument18 pagesAsianrhinoplasty: Dean M. Toriumi,, Colin D. PerodrbantmNo ratings yet
- A Novel Modified Vista Technique With Connective Tissue Graft in The Treatment of Gingival Recession - Chowdary 2020Document19 pagesA Novel Modified Vista Technique With Connective Tissue Graft in The Treatment of Gingival Recession - Chowdary 2020Natalia AcevedoNo ratings yet
- Extraction Site Reconstruction For Alveolar Ridge Preservation. Part 2: Membrane-Assisted Surgical TechniqueDocument4 pagesExtraction Site Reconstruction For Alveolar Ridge Preservation. Part 2: Membrane-Assisted Surgical TechniqueLuis MonteroNo ratings yet
- Surgical Incisions Balancing Surgical and Cosmetic Outcomes in Head and Neck OncosurgeryDocument4 pagesSurgical Incisions Balancing Surgical and Cosmetic Outcomes in Head and Neck OncosurgeryDwarika Prasad BajgaiNo ratings yet
- Jawline Contouring AlfaroDocument5 pagesJawline Contouring AlfaroÂngelo Rosso LlantadaNo ratings yet
- Assessment of Anterior Tucking and Cartilage Support Tympanoplasty To Evaluate Graft Uptake and Hearing OutcomeDocument4 pagesAssessment of Anterior Tucking and Cartilage Support Tympanoplasty To Evaluate Graft Uptake and Hearing OutcomeAkanshaNo ratings yet
- 2004-AJODO-Joondeph-Open-bite Closure With Mandibular OsteotomyDocument3 pages2004-AJODO-Joondeph-Open-bite Closure With Mandibular OsteotomyAlejandro RuizNo ratings yet
- Surgically Assisted Rapid Palatal Expansion:: An Outpatient Technique With Long-Term StabilityDocument4 pagesSurgically Assisted Rapid Palatal Expansion:: An Outpatient Technique With Long-Term StabilityemanNo ratings yet
- Surgic Al Ma Na Gement Oftheseptal Per Forat Ion: Deborah Watson,, Gregory BarkdullDocument11 pagesSurgic Al Ma Na Gement Oftheseptal Per Forat Ion: Deborah Watson,, Gregory BarkdullVinoth LakshmikanthNo ratings yet
- Cme 200704Document16 pagesCme 200704tomyhardiantoNo ratings yet
- Prosthetic SurgeryDocument14 pagesProsthetic SurgeryCristina CArrera100% (1)
- Beck CD A Journal Pinhole Article October 20181Document5 pagesBeck CD A Journal Pinhole Article October 20181Michael XuNo ratings yet
- Journal Reading - Keystone FlapDocument18 pagesJournal Reading - Keystone FlapCaroline DewiNo ratings yet
- Case Report On Maxillary Labial FrenectomyDocument9 pagesCase Report On Maxillary Labial Frenectomyviolita chresnaNo ratings yet
- Aumento de Reborde Con Tejido BlandoDocument8 pagesAumento de Reborde Con Tejido BlandoSilvia SolisNo ratings yet
- LectureDocument8 pagesLectureMohamedAtefNo ratings yet
- Original Articles: Rationale and Methods For Crown LengtheningDocument4 pagesOriginal Articles: Rationale and Methods For Crown LengtheningAna CernaianuNo ratings yet
- 2015 - A New Technique For Increasing Keratinized Tisue Around Dental Implants. The Partialy Epithelialized Free Conective Tisue Graft. Retrospective Analysis of A Case Series - Eberhard FrischDocument7 pages2015 - A New Technique For Increasing Keratinized Tisue Around Dental Implants. The Partialy Epithelialized Free Conective Tisue Graft. Retrospective Analysis of A Case Series - Eberhard FrischJose LuisNo ratings yet
- ROOT COVERAGE WITH PERIOSTEUM PEDICLE GRAFT - A NOVEL APPROACH DR Vineet VinayakDocument3 pagesROOT COVERAGE WITH PERIOSTEUM PEDICLE GRAFT - A NOVEL APPROACH DR Vineet VinayakDr Vineet VinayakNo ratings yet
- Open Brow Lift Techniques and Patient EvaluationDocument8 pagesOpen Brow Lift Techniques and Patient EvaluationdoctorbanNo ratings yet
- Cohen 1968Document6 pagesCohen 1968Victor Corona BuenfilNo ratings yet
- Principles of Oral SurgeryDocument56 pagesPrinciples of Oral SurgeryJayeshNo ratings yet
- Article 3Document7 pagesArticle 3Lana DbbNo ratings yet
- Acquired Maxillary DefectsDocument19 pagesAcquired Maxillary DefectstamersarwtsaadNo ratings yet
- Incisional Hernia Open ProceduresDocument25 pagesIncisional Hernia Open ProceduresElias Emmanuel JaimeNo ratings yet
- Revision Palate SurgeryDocument6 pagesRevision Palate SurgeryMarlon MartinezNo ratings yet
- Congress Auricular Reconstruction AbstractsDocument92 pagesCongress Auricular Reconstruction AbstractsRocio RamirezNo ratings yet
- Article 009Document9 pagesArticle 009MedstudNo ratings yet
- Septalextensiongraftin Asianrhinoplasty: Na-Hyun Hwang,, Eun-Sang DhongDocument11 pagesSeptalextensiongraftin Asianrhinoplasty: Na-Hyun Hwang,, Eun-Sang DhongRaphaela TravassosNo ratings yet
- 2000 J C. H S W A: Udson Ickey Cientific Riting WardDocument6 pages2000 J C. H S W A: Udson Ickey Cientific Riting WardPremshith CpNo ratings yet
- Maxillofacial Prosthetics: Kamolphob Phasuk,, Steven P. HaugDocument11 pagesMaxillofacial Prosthetics: Kamolphob Phasuk,, Steven P. Hauglaura sanchez avilaNo ratings yet
- Types of Gingival GraftsDocument34 pagesTypes of Gingival GraftsAhmad KurukchiNo ratings yet
- Basic Implant SurgeryDocument7 pagesBasic Implant SurgeryDr.Ankur Gupta100% (1)
- Surgical Options in Oroantral Fistula TreatmentDocument5 pagesSurgical Options in Oroantral Fistula TreatmentmartarayaniNo ratings yet
- Palatal Obturator Prostheses Following ResectionDocument7 pagesPalatal Obturator Prostheses Following Resectiondrgayen6042No ratings yet
- Carlo Baldi, Giovanpaolo Pini-Prato, Umberto Pagliaro, Michele Nieri, Daniele Saletta, Leonardo Muzzi, - and Pierpaolo Cortellini Coronally Advanced Flap Procedure F PDFDocument8 pagesCarlo Baldi, Giovanpaolo Pini-Prato, Umberto Pagliaro, Michele Nieri, Daniele Saletta, Leonardo Muzzi, - and Pierpaolo Cortellini Coronally Advanced Flap Procedure F PDFJulio César PlataNo ratings yet
- Use of Local and Axial Pattern Flaps For Reconstruction of The Hard and Soft Palate PDFDocument9 pagesUse of Local and Axial Pattern Flaps For Reconstruction of The Hard and Soft Palate PDFJose Luis Granados SolerNo ratings yet
- Endodontic SurgeryDocument16 pagesEndodontic SurgeryauntymayaNo ratings yet
- Critical View of The Myopectineal OrificeDocument10 pagesCritical View of The Myopectineal OrificeAntonio MarmolejoNo ratings yet
- Chap 7Document7 pagesChap 7Ruth BritoNo ratings yet
- Roll Man 2013Document6 pagesRoll Man 2013SergioNo ratings yet
- Kassab2010 PDFDocument12 pagesKassab2010 PDFdhwanit31No ratings yet
- Tre Atm Ent of Gingiva L Re Cession: Moawia M. Kassab,, Hala Badawi,, Andrew R. DentinoDocument12 pagesTre Atm Ent of Gingiva L Re Cession: Moawia M. Kassab,, Hala Badawi,, Andrew R. Dentinodhwanit31100% (1)
- Correcting Transverse Jaw Discrepancies with Surgery and OrthodonticsDocument17 pagesCorrecting Transverse Jaw Discrepancies with Surgery and OrthodonticsANGIE VANNESA ARIAS PINTONo ratings yet
- Robotic Hernia Surgery: A Comprehensive Illustrated GuideFrom EverandRobotic Hernia Surgery: A Comprehensive Illustrated GuideOmar Yusef KudsiNo ratings yet
- Peri-Implant Complications: A Clinical Guide to Diagnosis and TreatmentFrom EverandPeri-Implant Complications: A Clinical Guide to Diagnosis and TreatmentNo ratings yet
- IAN injury implant dentistry diagnosis causes prevention managementDocument7 pagesIAN injury implant dentistry diagnosis causes prevention managementmaxNo ratings yet
- IAN injury implant dentistry diagnosis causes prevention managementDocument7 pagesIAN injury implant dentistry diagnosis causes prevention managementmaxNo ratings yet
- Extraction and Immediate Implant Placement With Single-Stage Surgical Procedure Technical Notes and A Case Report PDFDocument8 pagesExtraction and Immediate Implant Placement With Single-Stage Surgical Procedure Technical Notes and A Case Report PDFmaxNo ratings yet
- Tunnel Access For Guided Bone Regeneration in The Maxillary AnteriorDocument6 pagesTunnel Access For Guided Bone Regeneration in The Maxillary Anteriormax100% (1)
- Practical Techniques for Tension-Free Flap ClosureDocument12 pagesPractical Techniques for Tension-Free Flap ClosuremaxNo ratings yet
- Advanced Platelet-Rich Fibrin A New Concept For Cell-Based Tissue Engineering by Means of Inflammatory CellsDocument22 pagesAdvanced Platelet-Rich Fibrin A New Concept For Cell-Based Tissue Engineering by Means of Inflammatory CellsmaxNo ratings yet
- Aaid Joi D 10 00146Document10 pagesAaid Joi D 10 00146maxNo ratings yet
- Advanced Platelet-Rich Fibrin A New Concept For Cell-Based Tissue Engineering by Means of Inflammatory CellsDocument11 pagesAdvanced Platelet-Rich Fibrin A New Concept For Cell-Based Tissue Engineering by Means of Inflammatory CellsmaxNo ratings yet
- Extention of Alveolar Ridge Without Raising The Mucoperiosteal Flapusing Minimally-Invasive Dental Implant Surgery - A New Step Ineffective Implantology PDFDocument4 pagesExtention of Alveolar Ridge Without Raising The Mucoperiosteal Flapusing Minimally-Invasive Dental Implant Surgery - A New Step Ineffective Implantology PDFmaxNo ratings yet
- Telescopic Crowns As Attachments For Implant Supported Restorations A Case SeriesDocument9 pagesTelescopic Crowns As Attachments For Implant Supported Restorations A Case SeriesmaxNo ratings yet
- Extention of Alveolar Ridge Without Raising The Mucoperiosteal Flapusing Minimally-Invasive Dental Implant Surgery - A New Step Ineffective Implantology PDFDocument4 pagesExtention of Alveolar Ridge Without Raising The Mucoperiosteal Flapusing Minimally-Invasive Dental Implant Surgery - A New Step Ineffective Implantology PDFmaxNo ratings yet
- Advanced Platelet-Rich Fibrin A New Concept For Cell-Based Tissue Engineering by Means of Inflammatory CellsDocument11 pagesAdvanced Platelet-Rich Fibrin A New Concept For Cell-Based Tissue Engineering by Means of Inflammatory CellsmaxNo ratings yet
- Ifu1076 en GB 01Document3 pagesIfu1076 en GB 01maxNo ratings yet
- PLPF PDFDocument88 pagesPLPF PDFmaxNo ratings yet
- Telescopic Crowns As Attachments For Implant Supported Restorations A Case SeriesDocument15 pagesTelescopic Crowns As Attachments For Implant Supported Restorations A Case SeriesmaxNo ratings yet
- Telescopic Crowns As Attachments For Implant Supported Restorations A Case SeriesDocument9 pagesTelescopic Crowns As Attachments For Implant Supported Restorations A Case SeriesmaxNo ratings yet
- A New Papilla Preservation Technique For Periodontal Regeneration of Severely Compromised TeethDocument6 pagesA New Papilla Preservation Technique For Periodontal Regeneration of Severely Compromised TeethmaxNo ratings yet
- Use of Fisiograft in Intrabony Defects-A Clinical and Radiological StudyDocument4 pagesUse of Fisiograft in Intrabony Defects-A Clinical and Radiological StudymaxNo ratings yet
- Instructions For Use: Nobelactive® ImplantDocument3 pagesInstructions For Use: Nobelactive® ImplantmaxNo ratings yet
- Instructions For UseDocument3 pagesInstructions For UsemaxNo ratings yet
- Types of Implant Surgical Guides in Dentistry A ReviewDocument10 pagesTypes of Implant Surgical Guides in Dentistry A Reviewmax100% (2)
- RTR Case Studies 07 BD - 0Document28 pagesRTR Case Studies 07 BD - 0maxNo ratings yet
- SB RinjaniDocument16 pagesSB RinjanimaxNo ratings yet
- Advanced Platelet-Rich Fibrin A New Concept For Cell-Based Tissue Engineering by Means of Inflammatory CellsDocument11 pagesAdvanced Platelet-Rich Fibrin A New Concept For Cell-Based Tissue Engineering by Means of Inflammatory CellsmaxNo ratings yet
- Champagne Fig Cultivar Released by Louisiana Agricultural Experiment StationDocument2 pagesChampagne Fig Cultivar Released by Louisiana Agricultural Experiment StationmaxNo ratings yet
- IAN injury implant dentistry diagnosis causes prevention managementDocument7 pagesIAN injury implant dentistry diagnosis causes prevention managementmaxNo ratings yet
- Aaid Joi D 10 00146Document10 pagesAaid Joi D 10 00146maxNo ratings yet
- Practical Techniques for Tension-Free Flap ClosureDocument12 pagesPractical Techniques for Tension-Free Flap ClosuremaxNo ratings yet
- FISIOGRAFT ENG Set 17 PDFDocument28 pagesFISIOGRAFT ENG Set 17 PDFmaxNo ratings yet
- Clasificacion Senos MaxilaresDocument8 pagesClasificacion Senos MaxilaresSebastián BernalNo ratings yet
- Accuracy of CAD CAM Fabricated Removable Par 2017 The Journal of ProstheticDocument7 pagesAccuracy of CAD CAM Fabricated Removable Par 2017 The Journal of ProstheticAlina Toma100% (1)
- Bio HorizonsDocument28 pagesBio Horizonsdanidani_01No ratings yet
- The Socket Shield Technique Case ReportDocument5 pagesThe Socket Shield Technique Case ReportAhmed Mohammed Saaduddin SapriNo ratings yet
- Meta Tags - Cosmodontist DentalDocument2 pagesMeta Tags - Cosmodontist Dentalotos mediaNo ratings yet
- Implant Catalog PDFDocument128 pagesImplant Catalog PDFodontoviNo ratings yet
- Inferior Level of Maxillary Sinus and Cortical BoneDocument10 pagesInferior Level of Maxillary Sinus and Cortical BoneLisbethNo ratings yet
- Dds Logbook 2012Document81 pagesDds Logbook 2012তৌহিদ তপুNo ratings yet
- Espertise Magazine 25Document24 pagesEspertise Magazine 25BatmanNo ratings yet
- Zimmer Tapered Swiss Plus Implant System CatalogueDocument8 pagesZimmer Tapered Swiss Plus Implant System CatalogueGretaSmidtNo ratings yet
- Dental Implant Literature ReviewDocument8 pagesDental Implant Literature Reviewafdtfhtut100% (1)
- Practice: Surgical Guidelines For Dental Implant PlacementDocument14 pagesPractice: Surgical Guidelines For Dental Implant PlacementAna94No ratings yet
- Principles of Fixed Implant ProsthodonticsDocument6 pagesPrinciples of Fixed Implant ProsthodonticsManar Abu ShadyNo ratings yet
- MCQ September 2004 Paper1Document11 pagesMCQ September 2004 Paper1api-2629165190% (10)
- Bone Augmentation in Implant Dentistry PDFDocument274 pagesBone Augmentation in Implant Dentistry PDFradia hamdoun100% (1)
- Implantium SurgicalDocument10 pagesImplantium SurgicalMyat NyanNo ratings yet
- Biological Aspects of Dental ImplantDocument23 pagesBiological Aspects of Dental ImplantAli AlmakramiNo ratings yet
- Basal Osseointegrated Implants ClassificDocument7 pagesBasal Osseointegrated Implants ClassificAnkur SaladaNo ratings yet
- Zero bone loss around implants possible with soft tissue augmentationDocument4 pagesZero bone loss around implants possible with soft tissue augmentationmarwaNo ratings yet
- PDFDocument12 pagesPDFEnrique Molina ZuviriaNo ratings yet
- Esthetics, Light and Colour in DentistryDocument101 pagesEsthetics, Light and Colour in DentistryDeepa MKNo ratings yet
- 01 Id 0000188379 46220 91Document8 pages01 Id 0000188379 46220 91Alejandro FereñoNo ratings yet
- Maxillary Superimposition - A Comparison of Three Methods For Cephalometric Evaluation of Growth and Treatment ChangeDocument10 pagesMaxillary Superimposition - A Comparison of Three Methods For Cephalometric Evaluation of Growth and Treatment ChangeNataly ComettaNo ratings yet
- Retention of Hopeless TeethDocument7 pagesRetention of Hopeless Teethbabyfish11No ratings yet
- Ante's 1926 Law Revisited A Systematic Review On SDocument10 pagesAnte's 1926 Law Revisited A Systematic Review On SJuan Jose Stuven RodriguezNo ratings yet
- Comparison of OverdenturesDocument2 pagesComparison of Overdenturesmfaheemuddin85No ratings yet
- JIndianProsthodontSoc6272-2051525 054155Document3 pagesJIndianProsthodontSoc6272-2051525 054155Pradusha RevuruNo ratings yet
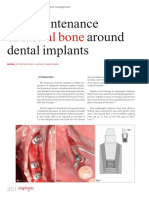
- Crestal Bone: The Maintenance of Around Dental ImplantsDocument5 pagesCrestal Bone: The Maintenance of Around Dental ImplantsJing XueNo ratings yet
- Applications of Orthodontic Mini-ImplantsDocument277 pagesApplications of Orthodontic Mini-ImplantsNicolas Homsi100% (1)