You might also like
- A Review of Thromboelastography PDFDocument5 pagesA Review of Thromboelastography PDFmarceloNo ratings yet
- Thrombectomy Procedures - Percutaneous Mechanical, Vascular Surgical, PharmaceuticalFrom EverandThrombectomy Procedures - Percutaneous Mechanical, Vascular Surgical, PharmaceuticalNo ratings yet
- Principles and Practice of Pharmacology for AnaesthetistsFrom EverandPrinciples and Practice of Pharmacology for AnaesthetistsRating: 5 out of 5 stars5/5 (1)
- Graphic Anaesthesia, second edition: Essential diagrams, equations and tables for anaesthesiaFrom EverandGraphic Anaesthesia, second edition: Essential diagrams, equations and tables for anaesthesiaNo ratings yet
- Evidence-Based Obstetric AnesthesiaFrom EverandEvidence-Based Obstetric AnesthesiaStephen H. HalpernNo ratings yet
- Anesthesiology Resident Manual of Procedures: A Step-by-Step GuideFrom EverandAnesthesiology Resident Manual of Procedures: A Step-by-Step GuideNo ratings yet
- Pediatric Anesthesiology Review: Clinical Cases for Self-AssessmentFrom EverandPediatric Anesthesiology Review: Clinical Cases for Self-AssessmentNo ratings yet
- Mechanisms of Drug Toxicity: Proceedings of the Third International Pharmacological MeetingFrom EverandMechanisms of Drug Toxicity: Proceedings of the Third International Pharmacological MeetingH. RaškováNo ratings yet
- Minimally Invasive Surgery for Chronic Pain Management: An Evidence-Based ApproachFrom EverandMinimally Invasive Surgery for Chronic Pain Management: An Evidence-Based ApproachGiorgio PietramaggioriNo ratings yet
- Infective Endocarditis: A Multidisciplinary ApproachFrom EverandInfective Endocarditis: A Multidisciplinary ApproachArman KilicNo ratings yet
- Liquid Biopsy in Urogenital Cancers and its Clinical UtilityFrom EverandLiquid Biopsy in Urogenital Cancers and its Clinical UtilitySeyed Mohammad Kazem AghamirNo ratings yet
- Lung Metabolism: Proteolysis and Antioproteolysis Biochemical Pharmacology Handling of Bioactive SubstancesFrom EverandLung Metabolism: Proteolysis and Antioproteolysis Biochemical Pharmacology Handling of Bioactive SubstancesAlain JunodNo ratings yet
- Anesthesia for Congenital Heart DiseaseFrom EverandAnesthesia for Congenital Heart DiseaseStephen A. StayerNo ratings yet
- Vascular Responses to PathogensFrom EverandVascular Responses to PathogensFelicity N.E. GavinsNo ratings yet
- AnaesthesiaDocument5 pagesAnaesthesiaAnonymous 4jkFIRalKNo ratings yet
- Lippincott S Anesthesia Review 1001 Questions And.20Document1 pageLippincott S Anesthesia Review 1001 Questions And.20Reem Salem0% (1)
- The Radiology Assistant - CT in TraumaDocument18 pagesThe Radiology Assistant - CT in Traumaابو عبد الرحمنNo ratings yet
- Telegram Cloud Document 4 5893461163299045618 PDFDocument232 pagesTelegram Cloud Document 4 5893461163299045618 PDFAndreea FlorinaNo ratings yet
- Anesthesia Complications in the Dental OfficeFrom EverandAnesthesia Complications in the Dental OfficeRobert C. BosackNo ratings yet
- Assessment of Postoperative Fever BMJDocument40 pagesAssessment of Postoperative Fever BMJMario Guzmán GutiérrezNo ratings yet
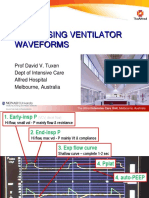
- Ventilator Waveforms DavidTuxen2Document41 pagesVentilator Waveforms DavidTuxen2Syed Shahrul Naz Syed100% (1)
- Basics of Chest X-RayDocument44 pagesBasics of Chest X-RayMelissa Aina Mohd YusofNo ratings yet
- Important MCQDocument23 pagesImportant MCQFarrukh Ali KhanNo ratings yet
- AnaesthesiaDocument8 pagesAnaesthesiarakeeb qadriNo ratings yet
- Measuring Cardiac Output: Intermittent Bolus Thermodilution MethodDocument6 pagesMeasuring Cardiac Output: Intermittent Bolus Thermodilution Methodsathi111No ratings yet
- Essentials of Evidence-Based Practice of Neuroanesthesia and Neurocritical CareFrom EverandEssentials of Evidence-Based Practice of Neuroanesthesia and Neurocritical CareHemanshu PrabhakarNo ratings yet
- L. A. Geddes ME, PHD Auth. Handbook of Blood Pressure MeasurementDocument171 pagesL. A. Geddes ME, PHD Auth. Handbook of Blood Pressure MeasurementYashNo ratings yet
- Avinash B Kumar MD Assistant Professor Anesthesiology and Critical Care Dec 2006Document29 pagesAvinash B Kumar MD Assistant Professor Anesthesiology and Critical Care Dec 2006sgod34No ratings yet
- Wilson Disease: Pathogenesis, Molecular Mechanisms, Diagnosis, Treatment and MonitoringFrom EverandWilson Disease: Pathogenesis, Molecular Mechanisms, Diagnosis, Treatment and MonitoringKarl Heinz WeissNo ratings yet
- Regional Nerve Blocks And Infiltration Therapy: Textbook and Color AtlasFrom EverandRegional Nerve Blocks And Infiltration Therapy: Textbook and Color AtlasDanilo JankovicNo ratings yet
- Arab-Board ExamDocument104 pagesArab-Board Examahmed.farag.ali2020No ratings yet
- Anesthesia For EndosDocument14 pagesAnesthesia For EndosJosé Moreira Lima Neto100% (1)
- Prehospital Anesthesia HandbookDocument46 pagesPrehospital Anesthesia HandbookoscarNo ratings yet
- Diploma Guide - EnglishDocument11 pagesDiploma Guide - EnglishAndra Victoria TitaNo ratings yet
- ACE 2007 4A QuestionsDocument29 pagesACE 2007 4A QuestionsRachana GudipudiNo ratings yet
- Anaesthesia and Sedation Outside TheatresDocument15 pagesAnaesthesia and Sedation Outside Theatresمحمد زينNo ratings yet
- Role of Simulation in Anesthesia PracticeDocument39 pagesRole of Simulation in Anesthesia PracticeNitin ..100% (1)
- Evidence Based Emergency Care PDFDocument2 pagesEvidence Based Emergency Care PDFMelissa0% (1)
- Acquired TTP - Clinical Manifestations and Diagnosis - UpToDateDocument16 pagesAcquired TTP - Clinical Manifestations and Diagnosis - UpToDatepradeep danielNo ratings yet
- Cisatracurium - An Overview - ScienceDirect TopicsDocument10 pagesCisatracurium - An Overview - ScienceDirect Topicspradeep danielNo ratings yet
- 3.4.3 Left Atrial Size - 123sonographyDocument8 pages3.4.3 Left Atrial Size - 123sonographypradeep danielNo ratings yet
- Caudal anesthesia guideDocument27 pagesCaudal anesthesia guidepradeep daniel100% (1)
- Anaesthetic Management of The Child With Haematological Malignancy - BJA Education - Oxford AcademicDocument19 pagesAnaesthetic Management of The Child With Haematological Malignancy - BJA Education - Oxford Academicpradeep danielNo ratings yet
- A Method For Reliable and Simultaneous Cannulation of The Epidural and Subarachnoid Spaces in PigsDocument6 pagesA Method For Reliable and Simultaneous Cannulation of The Epidural and Subarachnoid Spaces in Pigspradeep danielNo ratings yet
- Editorial: Ó 2002 Blackwell Science LTDDocument5 pagesEditorial: Ó 2002 Blackwell Science LTDpradeep danielNo ratings yet
- Brew Like A BaristaDocument25 pagesBrew Like A Baristacoolzat33% (3)
- Acute Coronary Syndromes - BJA Education - Oxford AcademicDocument18 pagesAcute Coronary Syndromes - BJA Education - Oxford Academicpradeep danielNo ratings yet
- Christoph 2005Document12 pagesChristoph 2005pradeep danielNo ratings yet
- How To Choose The Right Machine For YouDocument5 pagesHow To Choose The Right Machine For Youpradeep danielNo ratings yet
- Obstructive Jaundice and Perioperative ManagementsDocument8 pagesObstructive Jaundice and Perioperative ManagementsTri UtomoNo ratings yet
- LupusDocument7 pagesLupusorapoosaNo ratings yet
- Supraglottic Airway Devices Recent PDFDocument6 pagesSupraglottic Airway Devices Recent PDFpradeep danielNo ratings yet
- Paediatric Anaesthesia Formulas: Fluid RequirementsDocument13 pagesPaediatric Anaesthesia Formulas: Fluid RequirementsFemiko Panji AprilioNo ratings yet
- Manejo Del Samgrado PerioperatorioDocument64 pagesManejo Del Samgrado PerioperatorioDarwin QuijanoNo ratings yet
- R On T PhenomeneonDocument3 pagesR On T Phenomeneonpradeep danielNo ratings yet
- Hyperkalemia KI PDFDocument9 pagesHyperkalemia KI PDFNarinder SharmaNo ratings yet
- Indian J Surg Oncol Preoperative Management of Patients Undergoing Cytoreductive Surgery and Hyperthermic Intraperitoneal ChemotherapyDocument7 pagesIndian J Surg Oncol Preoperative Management of Patients Undergoing Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapypradeep danielNo ratings yet
- Anaesthesia Resident's HandbookDocument445 pagesAnaesthesia Resident's HandbookAnastasiafynn50% (2)
- Minor Complications During Thoracic Epidural.14Document2 pagesMinor Complications During Thoracic Epidural.14pradeep danielNo ratings yet
- Atelectasis BjaDocument10 pagesAtelectasis Bjapradeep danielNo ratings yet
- Eightball Corner PocketDocument2 pagesEightball Corner Pocketpradeep danielNo ratings yet
- Clinical Procedures in Emergency Medicine 5th EditDocument1 pageClinical Procedures in Emergency Medicine 5th Editpradeep danielNo ratings yet
- Sepsis What S New in 2019 .9Document6 pagesSepsis What S New in 2019 .9pradeep danielNo ratings yet
- Perioperative Uid Management: Science, Art or Random Chaos?Document5 pagesPerioperative Uid Management: Science, Art or Random Chaos?pradeep danielNo ratings yet
- Monitoring Depth of AnaesthesiaDocument10 pagesMonitoring Depth of AnaesthesiaSuresh KumarNo ratings yet
- New Airway Concepts BjaDocument13 pagesNew Airway Concepts Bjapradeep danielNo ratings yet
- 10.1007@s12630 019 01306 XDocument12 pages10.1007@s12630 019 01306 Xpradeep danielNo ratings yet
- Handling Section Editor:Dr David Polaner: Title Page Letters To The EditorsDocument5 pagesHandling Section Editor:Dr David Polaner: Title Page Letters To The Editorspradeep danielNo ratings yet
- Acetaminophen Suppository Mechanism of Action Side Effects Nursing ResponsibilitiesDocument2 pagesAcetaminophen Suppository Mechanism of Action Side Effects Nursing ResponsibilitiesNiziu BearsNo ratings yet
- To Study The Attitude of IV B.D.S. and Intern Students From A Dental College in Western Maharashtra Towards Pursuing Post Graduate Course in Oral Medicine and RadiologyDocument7 pagesTo Study The Attitude of IV B.D.S. and Intern Students From A Dental College in Western Maharashtra Towards Pursuing Post Graduate Course in Oral Medicine and RadiologyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- HEALTH ReviewerDocument7 pagesHEALTH Reviewersalazar dinnieseNo ratings yet
- TelecardiologyDocument20 pagesTelecardiologyPushpavalli Mohan100% (1)
- Depression and CancerDocument4 pagesDepression and CancerRommy EspinozaNo ratings yet
- 19 AD CBT Mock Questions A4 V1 PDFDocument29 pages19 AD CBT Mock Questions A4 V1 PDFAncy JustineNo ratings yet
- Urethral Trauma - Injuries Poisoning - MSD Manual Professional EditionDocument2 pagesUrethral Trauma - Injuries Poisoning - MSD Manual Professional EditionNaufal NaswanNo ratings yet
- My Parkinson's CB - Blue Heron Health NewsDocument23 pagesMy Parkinson's CB - Blue Heron Health Newscuongch30% (1)
- Wulandari (2015)Document37 pagesWulandari (2015)sry yanaNo ratings yet
- Occupational Therapy Rehabilitation Paraplegic PatientDocument7 pagesOccupational Therapy Rehabilitation Paraplegic PatientAlina PasăreNo ratings yet
- Real Exam Ethics OSCEDocument3 pagesReal Exam Ethics OSCEmonica ortizNo ratings yet
- HYPERTENSION CASE MANAGEMENTDocument49 pagesHYPERTENSION CASE MANAGEMENTCarl Angelo SuaybaguioNo ratings yet
- Priyanshu Raj Test ReportsDocument5 pagesPriyanshu Raj Test ReportsMr XNo ratings yet
- First Aid For Gunshot Wounds and FracturesDocument42 pagesFirst Aid For Gunshot Wounds and FracturesIfedigbo-Ejidike NwamakaNo ratings yet
- Agreement Between 2D and 3D Radiographic Outcome Assessment 1 Year After Periapical SurgeryDocument11 pagesAgreement Between 2D and 3D Radiographic Outcome Assessment 1 Year After Periapical SurgeryMufidah NurulNo ratings yet
- Colon Cleansing Kit Dosage CalendarDocument36 pagesColon Cleansing Kit Dosage CalendarYoungBodyNo ratings yet
- Epi NotesDocument5 pagesEpi NoteshoneykrizelNo ratings yet
- Oxcarbazepine - AdultsDocument3 pagesOxcarbazepine - Adultsakshay dahiweleNo ratings yet
- BPJS Coding IcdDocument4 pagesBPJS Coding IcdDewi Agustina100% (1)
- PBL 1 Aspergillus - G1Document14 pagesPBL 1 Aspergillus - G1Rahmi Syarafina HakimNo ratings yet
- Jadwal Praktik Dokter 19082019Document23 pagesJadwal Praktik Dokter 19082019Novin EkasariNo ratings yet
- Introduction in Skeletal System1Document11 pagesIntroduction in Skeletal System1joana cortezNo ratings yet
- Guidelines For The Safe and Quality Use of Clozapine in The WA Health System PDFDocument49 pagesGuidelines For The Safe and Quality Use of Clozapine in The WA Health System PDFAdrian TintareanuNo ratings yet
- Annotated Ultra BTR Short 22-4-23 FMT, Derma, Anaesthesia, OrthoDocument27 pagesAnnotated Ultra BTR Short 22-4-23 FMT, Derma, Anaesthesia, OrthoAshok DaukiyaNo ratings yet
- Andrew Solomon Case Study - EditedDocument5 pagesAndrew Solomon Case Study - EditedJefferson KagiriNo ratings yet
- NHM Letter World Diabetes DayDocument9 pagesNHM Letter World Diabetes DayAnonymous RCDcVGlFpzNo ratings yet
- TORCH in PregnancyDocument122 pagesTORCH in PregnancyroserosannaNo ratings yet
- Daftar Pustaka-DikonversiDocument7 pagesDaftar Pustaka-DikonversiRomi MufthiNo ratings yet
- (Grade 9) MAPEH (Health) - Drugs (2nd)Document3 pages(Grade 9) MAPEH (Health) - Drugs (2nd)KenNo ratings yet
- Legmed CaseDocument282 pagesLegmed CasePrecious PatawegNo ratings yet