You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5810)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Anatomy of The SpineDocument83 pagesAnatomy of The SpineUkhti Nur Zannah83% (6)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- OrchestrationDocument566 pagesOrchestrationpelocoha93% (15)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- USMLE STEP - 1 Self NotesDocument11 pagesUSMLE STEP - 1 Self NotesStudent AkashNo ratings yet
- MF 6400 7400 HHP en 14671Document19 pagesMF 6400 7400 HHP en 14671Dan Strafuschi100% (1)
- Melbourne Basin Guide PDFDocument92 pagesMelbourne Basin Guide PDFBrad Weir100% (2)
- Anderson Darling TestDocument45 pagesAnderson Darling Testpandyakavi100% (1)
- Diagnóstico Por Imagem - ThrallDocument764 pagesDiagnóstico Por Imagem - ThrallMariana de Queiroz Sampaio100% (1)
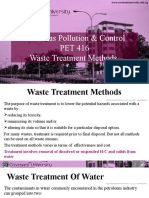
- Oil & Gas Pollution & Control PET 416 Waste Treatment MethodsDocument24 pagesOil & Gas Pollution & Control PET 416 Waste Treatment MethodsVictoria AinaNo ratings yet
- Math 8-Third Quarter ExaminationDocument4 pagesMath 8-Third Quarter ExaminationJoeyGansan80% (5)
- English: Quarter 4: Week 3 Learning Activity SheetsDocument8 pagesEnglish: Quarter 4: Week 3 Learning Activity SheetsFrances Quibuyen Datuin100% (1)
- Astm D4239 18 SulphurDocument8 pagesAstm D4239 18 SulphurMd Naseem Javed100% (4)
- Crossm: Hendra and Nipah Virus Infection in Cultured Human Olfactory Epithelial CellsDocument5 pagesCrossm: Hendra and Nipah Virus Infection in Cultured Human Olfactory Epithelial CellsfreddyNo ratings yet
- 74M1 PDFDocument23 pages74M1 PDFfreddyNo ratings yet
- Transmission of Human Infection With Nipah Virus: InvitedarticleDocument6 pagesTransmission of Human Infection With Nipah Virus: InvitedarticlefreddyNo ratings yet
- Inducible Rubicon Facilitates Viral Replication by Antagonizing Interferon ProductionDocument14 pagesInducible Rubicon Facilitates Viral Replication by Antagonizing Interferon ProductionfreddyNo ratings yet
- 201combined Science Paper 6 AnswerDocument9 pages201combined Science Paper 6 AnswerfreddyNo ratings yet
- JJJJJJJJDocument4 pagesJJJJJJJJfreddyNo ratings yet
- Metabolites Typhoid CarriesDocument15 pagesMetabolites Typhoid CarriesfreddyNo ratings yet
- Antagonist 1Document30 pagesAntagonist 1freddyNo ratings yet
- Upsr Maths TipsDocument32 pagesUpsr Maths Tipssenthanm2013No ratings yet
- Vaccine: Jason R. Andrews, Edward T. RyanDocument8 pagesVaccine: Jason R. Andrews, Edward T. RyanfreddyNo ratings yet
- DirectDocument7 pagesDirectfreddyNo ratings yet
- SSADocument10 pagesSSAAnkush KumarNo ratings yet
- Question Text: Select One: A. B. C. D. eDocument11 pagesQuestion Text: Select One: A. B. C. D. eRandyl Garcia EsmeroNo ratings yet
- Camasuire Stalp Cu FerocimentDocument8 pagesCamasuire Stalp Cu FerocimentChelemen MaryaNo ratings yet
- Septic Tank Components and Design of Septic TankDocument21 pagesSeptic Tank Components and Design of Septic TankChau Suktana EnlingNo ratings yet
- Manuskrip RiniDocument11 pagesManuskrip RiniRiniWagisanRkwtNo ratings yet
- MSDS - TOPCO (I)Document19 pagesMSDS - TOPCO (I)Andrea VarasNo ratings yet
- SOAL SEMESTER Genap KLS X 20202021 - Sastra InggrisDocument4 pagesSOAL SEMESTER Genap KLS X 20202021 - Sastra InggrisIka Endah MadyasariNo ratings yet
- Satellite P55T B5340Document4 pagesSatellite P55T B5340Marcelino SalazarNo ratings yet
- Medical Laboratory SIWES Report For NigeDocument40 pagesMedical Laboratory SIWES Report For NigeAbdulrauf AmeenNo ratings yet
- Wa Police Building Code Technical CriteriaDocument73 pagesWa Police Building Code Technical CriteriaKazz BastidasNo ratings yet
- Lm3622 Aplication CircuitDocument2 pagesLm3622 Aplication CircuitDavid LopezNo ratings yet
- Module 1Document9 pagesModule 1ALEXANDER BRYAN GONo ratings yet
- MCY4463PFRW4Document3 pagesMCY4463PFRW4Matheus Albuquerque de SaturnoNo ratings yet
- Direction in MotionDocument5 pagesDirection in MotionDaniel BerryNo ratings yet
- Debreu (1953) - Nonnegative Square MatricesDocument12 pagesDebreu (1953) - Nonnegative Square MatricesHilarius HilarianteNo ratings yet
- Theology 131 Dacanay Master NotesDocument14 pagesTheology 131 Dacanay Master NotesTrinca Diploma100% (1)
- Update 1 Of:: Use of Solid Catalysts in Friedel Crafts Acylation ReactionsDocument34 pagesUpdate 1 Of:: Use of Solid Catalysts in Friedel Crafts Acylation ReactionsikaNo ratings yet
- DATASHEETDocument3 pagesDATASHEETPersonal OpxionNo ratings yet
- 2-1 MFCSQN Bank R16Document8 pages2-1 MFCSQN Bank R16Bhargavipriyanka YarramNo ratings yet