You might also like
- The Dental Pulp: Biology, Pathology, and Regenerative TherapiesFrom EverandThe Dental Pulp: Biology, Pathology, and Regenerative TherapiesNo ratings yet
- Pigmentedlesionsoftheoral Cavity:: An UpdateDocument12 pagesPigmentedlesionsoftheoral Cavity:: An UpdateBima Ewando KabanNo ratings yet
- Oral and Maxillofacial PathologyDocument11 pagesOral and Maxillofacial PathologyIzadora VeigaNo ratings yet
- Sbikorva, 2018Document3 pagesSbikorva, 2018Izadora VeigaNo ratings yet
- Melanin-Associated Pigmented Lesions of The Oral Mucosa: Presentation, Differential Diagnosis, and TreatmentDocument10 pagesMelanin-Associated Pigmented Lesions of The Oral Mucosa: Presentation, Differential Diagnosis, and TreatmentFalling InsideNo ratings yet
- Oral Melanotic Macule - An Unusual Occurrence in GingivaDocument4 pagesOral Melanotic Macule - An Unusual Occurrence in GingivaYeni PuspitasariNo ratings yet
- Gingival Pigmentation and Its Treatment ModalititesDocument4 pagesGingival Pigmentation and Its Treatment ModalititesramaNo ratings yet
- Oral Melanotic Macule - A Case Report: Journal of Indian Society of Pedodontics and Preventive Dentistry July 2004Document4 pagesOral Melanotic Macule - A Case Report: Journal of Indian Society of Pedodontics and Preventive Dentistry July 2004Yeni PuspitasariNo ratings yet
- Lower Facial and Cervical Lymphadenopathy in The Context of Clinical DentistryDocument4 pagesLower Facial and Cervical Lymphadenopathy in The Context of Clinical Dentistryfaizal prabowo KalimanNo ratings yet
- Oral MelanoticDocument3 pagesOral MelanoticWulan Ambar WatyNo ratings yet
- 2 ApikDocument5 pages2 ApikAhmad Syauqie Al MuhdarNo ratings yet
- A Classification of Oral Pigmentation: Se-Quences.v":"Document2 pagesA Classification of Oral Pigmentation: Se-Quences.v":"Purva DalmiaNo ratings yet
- Journal Reading IpmDocument7 pagesJournal Reading Ipmdian permata pratamaNo ratings yet
- Differential Diagnosis of Tongue LesionsDocument12 pagesDifferential Diagnosis of Tongue LesionsKartikakhairaniNo ratings yet
- Beggs 2010Document13 pagesBeggs 2010shaheena ahmedNo ratings yet
- KalmarDocument8 pagesKalmarKING COMICNo ratings yet
- Clinical Success of Fiber-Reinforced Composite Resin As A Space MaintainerDocument2 pagesClinical Success of Fiber-Reinforced Composite Resin As A Space MaintainerKartika KurniasariNo ratings yet
- A Case of Longitudinal Melanonychia in A Child - Benign or MalignaDocument7 pagesA Case of Longitudinal Melanonychia in A Child - Benign or MalignaMariana JuravleNo ratings yet
- Differential Diagnosis of Tongue Lesions: Quintessence International June 2003Document13 pagesDifferential Diagnosis of Tongue Lesions: Quintessence International June 2003Sidney QuinceNo ratings yet
- Oral Ulceration: GP Guide To Diagnosis and Treatment: Stephen Flint Ma, PHD, MB BS, BDS, FDSRCS, Ffdrcsi, FicdDocument9 pagesOral Ulceration: GP Guide To Diagnosis and Treatment: Stephen Flint Ma, PHD, MB BS, BDS, FDSRCS, Ffdrcsi, FicdEstuNo ratings yet
- Black and Brown Oro-Facial Mucocutaneous NeoplasmsDocument15 pagesBlack and Brown Oro-Facial Mucocutaneous NeoplasmsKarina CarlinNo ratings yet
- Malignant Melanoma of Oral Cavity PDFDocument3 pagesMalignant Melanoma of Oral Cavity PDFahmed shimalNo ratings yet
- Celulitis Odontogenica en Niños Caso Clinico 2Document6 pagesCelulitis Odontogenica en Niños Caso Clinico 2ana mariaNo ratings yet
- Complications of An Unrecognized Cheek Biting Habit Following A Dental VisitDocument3 pagesComplications of An Unrecognized Cheek Biting Habit Following A Dental VisitChintya Monica AmelindaNo ratings yet
- Lec. 13 &14 Epithelial DisordersDocument10 pagesLec. 13 &14 Epithelial DisordersZainab AlshamaryNo ratings yet
- PV 1Document4 pagesPV 1Aing ScribdNo ratings yet
- Pseudoepitheliomatous Hyperplasia in Oral Lesions: A ReviewDocument5 pagesPseudoepitheliomatous Hyperplasia in Oral Lesions: A ReviewBrian EnamoradoNo ratings yet
- Black and Brown LesionDocument5 pagesBlack and Brown LesionGhada AlqrnawiNo ratings yet
- Neutrophils: in Health and DiseaseDocument65 pagesNeutrophils: in Health and DiseaseKush Pathak100% (1)
- AmalgamDocument3 pagesAmalgamMira AnggrianiNo ratings yet
- Jurnal Lentigo 1Document17 pagesJurnal Lentigo 1Nungky NadyaNo ratings yet
- Melanocytic Lesions of The ConjunctivaDocument8 pagesMelanocytic Lesions of The ConjunctivaR.m. IrsanNo ratings yet
- SCMS V34i4 White Lesions in The Oral CavityDocument10 pagesSCMS V34i4 White Lesions in The Oral CavityTasneem Hussiny AbdallahNo ratings yet
- White Sponge NevusDocument3 pagesWhite Sponge NevusMuhammad Hilmy ZNo ratings yet
- Contents 2020 Dermatologic-ClinicsDocument3 pagesContents 2020 Dermatologic-Clinicsandifarra281002No ratings yet
- Arduino 2017Document8 pagesArduino 2017neetika guptaNo ratings yet
- Introduction and Journal Peak Pigmented Lesions of Oral CavityDocument21 pagesIntroduction and Journal Peak Pigmented Lesions of Oral CavityMoses ObedNo ratings yet
- Melanoma of The Oral Cavity: Pathogenesis, Dermoscopy, Clinical Features, Staging and ManagementDocument7 pagesMelanoma of The Oral Cavity: Pathogenesis, Dermoscopy, Clinical Features, Staging and Managementagung permanaNo ratings yet
- Oral Pathology in Paediatric Patients-Mini-Systematic ReviewDocument7 pagesOral Pathology in Paediatric Patients-Mini-Systematic ReviewYuganya SriNo ratings yet
- 1-Malignant Melanoma of The Oral Cavity A ReviewDocument3 pages1-Malignant Melanoma of The Oral Cavity A ReviewPaomo Zhixia EarlyNo ratings yet
- 494 PDFDocument6 pages494 PDFranz ibonkNo ratings yet
- Oral Leukoplakia: Clinical, Histopathologic, and Molecular Features and Therapeutic ApproachDocument16 pagesOral Leukoplakia: Clinical, Histopathologic, and Molecular Features and Therapeutic ApproachVy KýNo ratings yet
- A Large Oral Melanoma - A Case ReportDocument5 pagesA Large Oral Melanoma - A Case Reportfitri handayaniNo ratings yet
- Enfermedades InmunologicasDocument14 pagesEnfermedades InmunologicasKarina OjedaNo ratings yet
- Neurofibromatosis Type 1 Review and Update On.10Document11 pagesNeurofibromatosis Type 1 Review and Update On.10claudio RivasNo ratings yet
- Melanin: The Biophysiology of Oral Melanocytes and Physiological Oral PigmentationDocument21 pagesMelanin: The Biophysiology of Oral Melanocytes and Physiological Oral PigmentationTín Nguyễn ThịNo ratings yet
- Applied Sciences: The Pseudolesions of The Oral Mucosa: Di Diagnosis and Related Systemic ConditionsDocument8 pagesApplied Sciences: The Pseudolesions of The Oral Mucosa: Di Diagnosis and Related Systemic Conditionssiti baiq gadishaNo ratings yet
- المستندDocument3 pagesالمستندftoom MohamedNo ratings yet
- Bone and Soft Tissue PathologyDocument74 pagesBone and Soft Tissue PathologyBayan HamedNo ratings yet
- Desquamative Gingivitis: A Sign of Mucocutaneous Disorders - A ReviewDocument6 pagesDesquamative Gingivitis: A Sign of Mucocutaneous Disorders - A Reviewsidra malikNo ratings yet
- Ijdr 201723 01Document3 pagesIjdr 201723 01lily oktarizaNo ratings yet
- Lymphangioma of The Dorsal TongueDocument4 pagesLymphangioma of The Dorsal TongueLaila FortunatoNo ratings yet
- Scientific Dental Journal: Pigmented Oral Lichen Planus: A Case ReportDocument6 pagesScientific Dental Journal: Pigmented Oral Lichen Planus: A Case ReportSasa AprilaNo ratings yet
- Investigations For Diseases of The Tongue A Review PDFDocument6 pagesInvestigations For Diseases of The Tongue A Review PDFShantanu DixitNo ratings yet
- Refen 3 PDFDocument8 pagesRefen 3 PDFSiti Aulia Rahma SyamNo ratings yet
- Oral Lichenoid Lesions - Distinguishing The Benign From The Deadly (2017)Document14 pagesOral Lichenoid Lesions - Distinguishing The Benign From The Deadly (2017)JohnNo ratings yet
- Palatal SwellingsDocument6 pagesPalatal Swellingsopi akbarNo ratings yet
- 1 - Lesi Pigmentasi - Mifthaqul Istikhomah (40620124) KelompokDocument5 pages1 - Lesi Pigmentasi - Mifthaqul Istikhomah (40620124) KelompokAnggun PratiwiNo ratings yet
- Passeron 2016Document23 pagesPasseron 2016GÜLSÜM GÜNEŞNo ratings yet
- OM Lecture 1Document12 pagesOM Lecture 1abood kofahiNo ratings yet
- 4gauging GTXDocument1 page4gauging GTXZulfahmi NurdinNo ratings yet
- Brochure-Gc Fuji ViiDocument16 pagesBrochure-Gc Fuji ViiZulfahmi NurdinNo ratings yet
- Indications and Case Series of Intentional Replantation of TeethDocument8 pagesIndications and Case Series of Intentional Replantation of TeethZulfahmi NurdinNo ratings yet
- SonicFill 2 Technique GuideDocument1 pageSonicFill 2 Technique GuideZulfahmi NurdinNo ratings yet
- SonicFill Handpiece Instructions For UseDocument58 pagesSonicFill Handpiece Instructions For UseZulfahmi NurdinNo ratings yet
- Dentj 39 2 04Document4 pagesDentj 39 2 04Zulfahmi NurdinNo ratings yet
- Effect of Refrigeration On Bond Strength of Self-Etching Adhesive SystemsDocument5 pagesEffect of Refrigeration On Bond Strength of Self-Etching Adhesive SystemsZulfahmi NurdinNo ratings yet
- Ludwig's Angina - An Emergency: A Case Report With Literature ReviewDocument7 pagesLudwig's Angina - An Emergency: A Case Report With Literature ReviewZulfahmi NurdinNo ratings yet
- Ellagic Acid Information & ReferencesDocument6 pagesEllagic Acid Information & ReferencesZulfahmi NurdinNo ratings yet
- Cariesactivitytests 090722115427 Phpapp01Document14 pagesCariesactivitytests 090722115427 Phpapp01Zulfahmi NurdinNo ratings yet
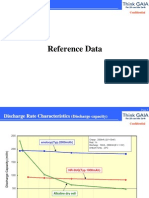
- Discharge Characteristics 3UQDocument5 pagesDischarge Characteristics 3UQZulfahmi NurdinNo ratings yet
- Jurnal Bagus GunDocument10 pagesJurnal Bagus GunPutrina SiregarNo ratings yet
- Anemii HemoliticeDocument74 pagesAnemii HemoliticeCNo ratings yet
- Clinical Presentation of Varicose VeinsDocument8 pagesClinical Presentation of Varicose VeinslucyishakNo ratings yet
- Rosilla, Leandro AGE: 5 Yrs Old Diagnosis: DHF IiiDocument4 pagesRosilla, Leandro AGE: 5 Yrs Old Diagnosis: DHF IiiAlexander Rodriguez OlipasNo ratings yet
- Classification of Malnutrition in ChildrenDocument2 pagesClassification of Malnutrition in ChildrenJai Jai MaharashtraNo ratings yet
- Ectopic Pregnancy Case StudyDocument81 pagesEctopic Pregnancy Case Studyjefroc90% (30)
- Supplementary Materials Supplementary Table Complications Meddra Preferred Term, N (%) Working Ability Recovered N 122 Working Ability Not Recovered N 91Document9 pagesSupplementary Materials Supplementary Table Complications Meddra Preferred Term, N (%) Working Ability Recovered N 122 Working Ability Not Recovered N 91Perdana SihiteNo ratings yet
- Split Brain TheoryDocument1 pageSplit Brain TheoryTezza Keizel FutalanNo ratings yet
- (13142143 - Folia Medica) Pharmacoeconomics of Bronchial AsthmaDocument9 pages(13142143 - Folia Medica) Pharmacoeconomics of Bronchial AsthmaChristinaNo ratings yet
- Fpgee SummaryDocument10 pagesFpgee SummaryDr-Ram ChowdharyNo ratings yet
- Oet Medicine Official Oet Practice Book 1 Cambridge TEST 1 FDocument42 pagesOet Medicine Official Oet Practice Book 1 Cambridge TEST 1 FP.K.No ratings yet
- APRIL 2018 Arba Minch, EthiopiaDocument54 pagesAPRIL 2018 Arba Minch, EthiopiaTesfahun TesfuNo ratings yet
- Treatment of Diabetes Mellitus T2 - Samir RaflaDocument35 pagesTreatment of Diabetes Mellitus T2 - Samir Raflasamir raflaNo ratings yet
- Critical Appraisal: On Article of Diagnostic Test (EBM-Diagnostic)Document28 pagesCritical Appraisal: On Article of Diagnostic Test (EBM-Diagnostic)Giovan GaulNo ratings yet
- RRT PT AssessmentDocument39 pagesRRT PT AssessmentRam NasaluddinNo ratings yet
- LTI A ReviewDocument22 pagesLTI A Reviewamamùra maamarNo ratings yet
- Medical Laboratory Technician or Clinical Laboratory TechnicianDocument2 pagesMedical Laboratory Technician or Clinical Laboratory Technicianapi-77503440No ratings yet
- Bacterial Quantification MCQsDocument3 pagesBacterial Quantification MCQsMahi ShafiqueNo ratings yet
- Policies On Continue Interval To Act An Orders For TreatmentDocument197 pagesPolicies On Continue Interval To Act An Orders For TreatmentMk Salamat Remoquillo100% (1)
- I S B A R: Nursing/Midwifery Shift To Shift Bedside Handover - Process FlowchartDocument1 pageI S B A R: Nursing/Midwifery Shift To Shift Bedside Handover - Process FlowchartAyu PurbaNo ratings yet
- Cell Salts William BoerickDocument525 pagesCell Salts William BoerickSorabh Sharma100% (1)
- 50 Studies Every Obstetrician-Gynecologist Should Know 1Document70 pages50 Studies Every Obstetrician-Gynecologist Should Know 1Deepak Sugumar100% (2)
- 25 New Single Herbs: 6. Clear Toxic-HeatDocument4 pages25 New Single Herbs: 6. Clear Toxic-HeatyayanicaNo ratings yet
- Prevention and Management of Diabetic Foot Ulcers PDFDocument68 pagesPrevention and Management of Diabetic Foot Ulcers PDFJianhua Shi100% (2)
- Physical Assessment: General AppearanceDocument2 pagesPhysical Assessment: General AppearanceSheryl Ann Barit PedinesNo ratings yet
- Ks Hospital, Hospital Road, Distt Mandi, Himachal Pradesh MANDI, 175001Document2 pagesKs Hospital, Hospital Road, Distt Mandi, Himachal Pradesh MANDI, 175001Anurag UniyalNo ratings yet
- English For Hospital StaffDocument6 pagesEnglish For Hospital StaffВолодимир ТатарінNo ratings yet
- Drug Study 2Document9 pagesDrug Study 2Justin PasaronNo ratings yet
- Case Based DiscussionDocument62 pagesCase Based DiscussionNeni SetyowatiNo ratings yet
- Therapeutic Massage and AcupressureDocument2 pagesTherapeutic Massage and AcupressureMagic LifeNo ratings yet