Professional Documents
Culture Documents
Comparison of Cervical Cancer Screening Strategies Incorporating Different Combinatioon PDF
Comparison of Cervical Cancer Screening Strategies Incorporating Different Combinatioon PDF
Uploaded by
Imanuel Far-FarOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Comparison of Cervical Cancer Screening Strategies Incorporating Different Combinatioon PDF
Comparison of Cervical Cancer Screening Strategies Incorporating Different Combinatioon PDF
Uploaded by
Imanuel Far-FarCopyright:
Available Formats
Research www. AJOG.
org
GENERAL GYNECOLOGY
Comparison of cervical cancer screening strategies
incorporating different combinations of cytology,
HPV testing, and genotyping for HPV 16/18:
results from the ATHENA HPV study
J. Thomas Cox, MD; Phillip E. Castle, PhD, MPH; Catherine M. Behrens, MD, PhD; Abha Sharma, PhD;
Thomas C. Wright Jr, MD; Jack Cuzick, PhD; and the Athena HPV Study Group
OBJECTIVE: The objective of the study was to compare 9 cervical can- cotesting with cytology increased sensitivity but did so by increasing
cer screening strategies to the current screening standard (cytology testing. Strategies that included integrated HPV16/18 testing provided
with human papillomavirus [HPV] triage of atypical squamous cells of more efficient referral to colposcopy.
undetermined significance) for the detection of high-grade cervical
CONCLUSION: Strategies that maximize detection of women at greatest
disease.
risk of cervical intraepithelial neoplasia grade 3 or greater by immediate
STUDY DESIGN: Women (n ⫽ 34,254) aged 30 years or older from the referral to colposcopy, with follow-up testing of women at intermediate
Addressing the Need for Advanced HPV Diagnostics (ATHENA) study risk, maximize the benefits of cervical cancer screening while decreas-
underwent screening with cytology and HPV testing with simultaneous ing the potential harm. Incorporating screening with HPV and triage of
HPV16/18 genotyping; those with atypical squamous cells of undeter- HPV-positive women by a combination of genotyping for HPV16/18 and
mined significance cytology or greater or HPV-positive status were re- cytology provided a good balance between maximizing sensitivity (ben-
ferred for colposcopy. efit) and specificity by limiting the number of colposcopies (potential
harm).
RESULTS: In general, screening strategies that offered greater sensitiv-
ity also required more referral to colposcopy. HPV testing was more Key words: Addressing the Need for Advanced HPV Diagnostics,
sensitive than cytology for detection of cervical intraepithelial neoplasia atypical squamous cells of undetermined significance, cotesting,
grade 2 or greater, but strategies that depended on cytology for triage of human papillomavirus, human papillomavirus 16/18, low-grade
HPV-positive women decreased this sensitivity. Various strategies of squamous intraepithelial lesion
Cite this article as: Cox JT, Castle PE, Behrens CM, et al. Comparison of cervical cancer screening strategies incorporating different combinations of cytology, HPV
testing, and genotyping for HPV 16/18: results from the ATHENA HPV study. Am J Obstet Gynecol 2013;208:184.e1-11.
I n March 2012, new primary cervical
screening guidelines were jointly is-
sued by the US Preventative Services
Task Force (USPSTF)1 and a consortium
of the American Cancer Society (ACS),
the American Society for Colposcopy
and Cervical Pathology (ASCCP), and
the American Society of Clinical Pathol-
ogists (ASCP).2 Based on the evidence
From Student Health, University of California, Santa Barbara (retired), Santa Barbara, CA (Dr Cox); Albert Einstein College of Medicine, Bronx, NY (Dr
Castle); Roche Molecular Systems, Pleasanton, CA (Drs Behrens and Sharma); the Department of Pathology, Columbia University Medical Center,
New York, NY (Dr Wright); and the Center for Cancer Prevention, Wolfson Institute of Preventive Medicine, Queen Mary University of London,
London, UK (Dr Cuzick).
Received July 20, 2012; revised Oct. 12, 2012; accepted Nov. 14, 2012.
This study was supported by Roche Molecular Systems.
J.T.C. and P.E.C. are compensated for their services as members of a Data Monitoring Board for HPV vaccines for Merck. J.T.C. has received
honoraria from Roche for assistance in the development of an educational slide set and for speaking on the cobas HPV Test. He has also received
honoraria for service on the scientific advisory board for Gen-Probe and advisory boards for Graceway and Bradley Pharmaceuticals. P.E.C. has
received HPV tests and testing for research at a reduced or no cost from Roche and Qiagen. T.C.W. is compensated for his services as a reference
pathologist, clinical adviser, and speaker for Roche, Gen-Probe, BD Diagnostics, and Ikonisys. He has received honoraria for serving on a scientific
advisory board for HPV vaccines for Merck. J.C. has served on advisory boards for Roche, Gen-Probe, Abbott, and Qiagen. C.M.B. and A.S. are
employees of Roche Molecular Systems.
Presented at EUROGIN 2012, Prague, Czech Republic, July 8-11, 2011.
Reprints: J. Thomas Cox, MD, 3345 Numancia St., Santa Ynez, CA 93460. tomcoxmd@aol.com.
0002-9378/$36.00 • © 2013 Mosby, Inc. All rights reserved. • http://dx.doi.org/10.1016/j.ajog.2012.11.020
See Journal Club, page 235
184.e1 American Journal of Obstetrics & Gynecology MARCH 2013
www.AJOG.org General Gynecology Research
that human papillomavirus (HPV) test- screening strategies to those endorsed by women with adequate colposcopy in
ing is more sensitive and therefore pro- the most recent US cervical cancer whom no lesion was seen; patients and
vides better negative predictive values screening guidelines. Ten different cervi- colposcopists were blinded to the cytol-
(NPV) than cytology, these new guide- cal cancer screening strategies, including ogy and HPV results.
lines recommend that women aged 30 several that use HPV testing alone as the An expert central pathology review
years and older be screened every 3 years initial screening method, were investi- (CPR) panel of 3 pathologists read all bi-
using cervical cytology alone or every 5 gated. The performance of each strategy opsies masked to any clinical data.
years using a combination of cervical cy- for detection of cervical intraepithelial Women achieving the study endpoint of
tology and high-risk HPV testing (re- neoplasia grade 2 (CIN2) or more severe CIN2 or more severe by CPR exited the
ferred to as cotesting). or CIN3 or more severe was explored, as study; those who did not reach this end-
The better NPV of HPV testing per- was the potential harm estimated by the point proceeded to the 3 year follow-up
mits a safe extension of the screening in- number of tests and the number of col- phase of the study, scheduled to con-
terval, thereby reducing harms caused poscopies (a metric used by the recent clude December 2012. The current anal-
by screening. The ACS/ASCCP/ASCP guideline process) needed to detect each ysis is restricted to disease detected at en-
guidelines endorsed the cotesting option high-grade lesion at baseline. These rollment; disease detected over the
as the preferred approach for women strategies included results of testing with subsequent 3 years of follow-up will be
aged 30 years and older,2 whereas the cytology and/or various combinations of analyzed separately.
USPSTF endorsed it as acceptable,1 and HPV testing, including HPV genotyping
the American College of Obstetricians for HPV 16 and HPV 18. Screening strategies
and Gynecologists (ACOG) expressed The 10 screening strategies were evalu-
support of these recommendations.3 ated based on review of the published
The ACS/ASCCP/ASCP guidelines rec- M ATERIALS AND M ETHODS cervical cancer screening literature and
ommend that cytology-negative/HPV- Study protocol appear to be the strategies most likely to
positive women undergo follow-up in 12 As previously described, the ATHENA be considered potentially attractive by
months with repeat cytology and HPV HPV study enrolled more than 47,000 the clinical and public health commu-
testing or, alternatively, cytology-negative/ women aged 21 years and older who pre- nities. Strategies 1 and 2 are cytology
HPV-positive women can be genotyped sented for cervical cancer screening; all screening strategies (Figure 1). Strategy
for HPV 16 and HPV 18.2 With the latter eligible participants had both Papanico- 1 consists of screening with cytology
option, women who are found to have ei- laou testing (by liquid-based cytology, with reflex HPV testing (pooled high-
ther HPV 16 or HPV 18 are referred for ThinPrep; Hologic, Bedford, MA) and risk HPV test for 14 genotypes) of
colposcopy, whereas those without these HPV testing (by Amplicor HPV test, Lin- ASC-US and referral of all women with
highest-risk HPV types are cotested again ear Array high-risk HPV genotyping test, HPV-positive ASC-US or low-grade
in 12 months. and the cobas HPV Test, all from Roche squamous intraepithelial lesion (LSIL)
The Addressing the Need for Ad- Molecular Systems).6 The protocol was or greater to colposcopy. Because this is
vanced HPV Diagnostics (ATHENA) approved by the institutional review the strategy most widely used in the
HPV study is a prospective 3 year cervi- boards at all study sites, and all women United States, it serves as the comparator
cal cancer screening trial designed to provided written informed consent be- for the other 9 strategies.
compare the performance of the newly fore undergoing any study procedures. Strategy 2 consists of screening with
introduced cobas HPV Test (Roche Mo- The current analysis focuses only on the cytology alone, with referral of all
lecular Diagnostics, Pleasanton, CA) subset of women aged 30 years old and women with ASC-US or greater to col-
both alone and in combination with cer- older to compare alternative manage- poscopy. Strategies 3, 4, and 5 (Figure 2)
vical cytology among women aged 21 ment strategies with those endorsed in incorporate cotesting with both cytology
years and older in the United States. the current guidelines. and HPV testing. They vary as to
Based on the cross-sectional data from All women in this subset who had ei- whether genotyping for HPV 16 and
the ATHENA trial, the US Food and ther abnormal cytology (atypical squa- HPV 18 is used and by the cytological
Drug Administration recently approved mous cells of undetermined significance threshold for referral to colposcopy.
for use in the United States the cobas [ASC-US] or greater) or who tested pos- Strategies 6 through 10 (Figure 3) use
HPV Test, which detects 11 pooled high- itive for HPV (by Amplicor or Linear Ar- HPV testing alone (pooled high-risk
risk HPV genotypes (HPV 31, 33, 35, 39, ray test) were scheduled for colposcopy. HPV test with, or without, genotyping
45, 51, 52, 56, 58, 59, and 68) and 1 pos- In addition, to adjust for ascertainment for HPV 16/18) as the initial screening
sible high-risk type (HPV 66) and con- bias, a randomly selected subset of test and differ by which triage tests are
currently provides separate results for women who tested negative for both cy- used to evaluate HPV-positive women.
HPV 16 and HPV 18.4-7 tology and HPV had colposcopy. Colpo- In the strategies described, women who
The current manuscript further ana- scopic biopsies were performed accord- did not meet the criteria for either imme-
lyzes the enrollment results of the ing to a standardized protocol, and a diate colposcopy or return to routine
ATHENA trial to investigate alternative random biopsy was required in all screening would be deferred to a 1 year
MARCH 2013 American Journal of Obstetrics & Gynecology 184.e2
Research General Gynecology www.AJOG.org
follow-up per the current guidelines2 as
FIGURE 1
indicated in Figures 2 and 3.
Cytology primary screening options
Statistical analysis Strategy 1: Cytology with reflex HPV (ASC-US triage)
For each screening strategy, the number
of tests (cytology and/or HPV test with Routine follow-up
or without integrated HPV 16/18 geno- NILM
type detection) required at baseline was >ASC-US
Pap Test Colposcopy
calculated, as was the number of colpos- Routine
Neg
copies required to detect 1 case of CIN2 ASC-US follow-up
or more severe or CIN3 or more severe. HPV Test
From the total catchment of CIN2 or Pos Colposcopy
more severe and CIN3 or more severe
detected, the number of cases not iden- Strategy 2: Cytology Alone
tified at baseline, and an estimate of the
number that could potentially be identi- NILM Routine screening
fied by each strategy at 12 month fol- Pap Test
low-up were calculated. The crude sensi- Colposcopy
ASC-US
tivity and specificity for detection of
CIN2 or more severe or CIN3 or more Strategies 1 and 2 screened initially with cytology only. Strategy 1, a recommended screening option
severe and its sensitivity and specificity for women aged 21 years or older, triages ASC-US by reflex HPV testing, sending to colposcopy
relative to strategy 1 were also deter- ASC-US/HPV positive and more severe than ASC-US (ie, ASC with possible HSIL [ASC-H], LSIL,
mined (Tables 2 and 3). atypical glandular cells [AGC], and HSIL). Women with normal cytology or ASC-US/HPV negativity
The cobas HPV Test results were cate- continued with routine screening. Strategy 2 sent all women with any abnormal cytology (ie, ASC-US
gorized as follows: HPV positive (posi- or more severe) to colposcopy, and all women with normal cytology continued with routine screening.
tive for any of 14 high-risk HPV types); This is not a recommended screening option but is included in this study for comparison with other
HPV negative (negative for all 14 high- options.
ASC-US, atypical squamous cells of undetermined significance; HPV, human papillomavirus; HSIL, high-grade squamous intraepithelial
risk HPV types); HPV 16/18 positive lesion; LSIL, low-grade squamous intraepithelial lesion.
(positive for HPV 16 and/or HPV 18, re- Cox. Cervical cancer screening strategies: evaluation of results from the ATHENA HPV study. Am J Obstet Gynecol 2013.
gardless of the presence or absence of 12
other HPV types); positive for 12 other
HPV types (positive for 1 or more of the more severe and 189 with CIN3 or more more severe. These included cytology
12 other HPV types and negative for severe. The most sensitive screening with HPV triage of ASC-US (strategy 1;
HPV 16 and HPV 18). strategy was screening with HPV alone 51.4% and 56.1%, respectively) and cy-
For calculations of sensitivity and (pooled 14 high-risk types) with referral tology alone (strategy 2; 53.2% and
specificity, only those cases in which col- of all HPV-positive women to colpos- 57.7%, respectively). Strategy 3 was also
poscopy was performed and a valid bi- copy (strategy 6), detecting 242 of CIN2 cytology based because it screened with
opsy result was obtained were consid- or more severe lesions (86.4%) and 170 cytology and HPV testing (cotesting) but
ered. Crude estimates are given because (89.9%) of the CIN3 or more severe le- used only the results of cytology and re-
the intent was to report on the utility of sions (Tables 2 and 3). However, this flex HPV testing of ASC-US to deter-
the strategies as would be observed in a strategy also had the highest false-posi- mine immediate referral to colposcopy.
clinical situation. Verification bias ad- tive rate for CIN3 or more severe Therefore, this strategy had an identical
justment would not change the relative (38.0%). In terms of the utilization of performance to strategy 1 during the first
sensitivities or specificities of the various colposcopy resources, it was almost as round of screening, except that cotesting
strategies or represent what happens in inefficient as the strategy of screening also identified cytology-negative/HPV-
clinical practice. with cytology alone and referring all positive women in need of additional
woman with ASC-US or more severe to follow-up in 12 months2 from which 72
R ESULTS colposcopy (strategy 2) since it required additional cases of CIN3 or more severe
A total of 34,254 women aged 30 years or 9.7 colposcopic evaluations to find a sin- could potentially be detected (subse-
older were eligible for this analysis; the gle case of CIN2 or more severe and 13.8 quently described as “cases identified for
mean age was 44.7 years, and the demo- to find a single case of CIN3 or more 12 month f/u” [Tables 2 and 3]). HPV
graphics are shown in Table 1. Among severe. alone with cytology triage of HPV-posi-
the eligible women, 2872 (8.4%) tested All strategies depending on cytology tive women (strategy 7) had the lowest
positive with the cobas HPV Test, and alone or on cytology as the sole reflex test cross-sectional sensitivity because the
1966 (5.7%) had abnormal cytology; 280 had the lowest sensitivities for detection triage test negates the increased sensitiv-
women were diagnosed with CIN2 or of CIN2 or more severe and CIN3 or ity of HPV testing. In contrast to the
184.e3 American Journal of Obstetrics & Gynecology MARCH 2013
www.AJOG.org General Gynecology Research
lower sensitivity of each of these strate-
FIGURE 2
gies, all but strategy 2 were among the
Cotesting primary screening options most specific, with false-positive rates
Strategy 3: Cotesting with reflex for ASC-US for detection of CIN3 or more severe be-
tween 8.7 (strategy 7) and 12.4 (strate-
Both Negative or Routine screening gies 1 and 3).
ASC-US/HPV- All 3 cotesting options approximately
HPV and ASC-US/HPV+
doubled the number of initial screening
Pap Test & >ASC-US
Colposcopy tests compared with the remaining
(Cotesting) strategies. Of the cotesting options,
NILM/HPV+ cotesting with genotyping triage and
Repeat cotest an ASC-US threshold (strategy 4) de-
in 12 mo. tected the most CIN2 or more severe
and CIN3 or more severe, with the
highest sensitivity (67.5% and 76.2%,
Strategy 4: Cotesting with genotyping and cytology triage:
respectively). However, because this
HPV 16/18 & ASC-US HPV+ threshold option required 32% more colposco-
pies than cotesting alone (strategy 3),
Both Negative or Routine screening the number of colposcopic evaluations
ASC-US/HPV- to detect 1 CIN2 or more severe (ap-
HPV with proximately 6) and 1 CIN3 or more se-
16/18 ASC-US/HPV+ or
>ASC-US or vere (approximately 8) was similar. Of
genotyping Colposcopy the cotesting options, strategy 4 also
and Pap Test NILM HPV16/18+
had the highest relative sensitivity for
(Cotesting)
NILM/HPV+ CIN2 or more severe and CIN3 or
but not 16/18 Repeat cotest more severe (1.31 and 1.36, respec-
in 12 mo. tively) but also had the highest false-
positive rate for CIN3 or more severe
(18.5%). Strategy 5 was similar to
Strategy 5: Cotesting with genotyping and cytology triage: strategy 4 but triaged non-HPV 16/
HPV 16/18 & LSIL threshold HPV 18 pooled positive women to col-
poscopy using an LSIL threshold rather
Both Negative or Routine screening than an ASC-US threshold; this strat-
HPV-/ASC-US egy was 5.3% less sensitive for CIN3 or
HPV with more severe than strategy 4 but re-
16/18 ≥LSIL or NILM
or ASC-US duced the number of colposcopies by
genotyping Colposcopy 14.3% (1030 vs 1202). The cotesting
and Pap Test HPV16/18+
strategies required between 5 and 6
(Cotesting) colposcopies to detect 1 CIN2 or more
ASC-US or
NILM/HPV+ severe, approximately the same as cy-
Repeat cotest
but not 16/18 tology with HPV triage of ASC-US
in 12 mo.
(strategy 1).
Strategies 3-5 screened initially with both cytology and testing for high-risk HPV. Strategies 4 and 5 All of the screening strategies based on us-
also utilized the information provided when the HPV test also included separate results for HPV 16 and ing HPV alone (pooled 14 high-risk types,
HPV 18 genotyping or, if not, when reflex genotyping could be done. Strategy 3, 1 of 2 recommended with or without HPV 16/18 genotyping) as
cotesting options for women aged 30 years or older, referred to colposcopy women with ASC-US HPV the initial test required similar numbers of
positivity and LSIL or more severe, irrespective of HPV result, whereas women with cytology-nega- testscomparedwiththecytology-basedstrat-
tivity/HPV positivity had repeat cotesting in 12 months and women who were cytology negative/HPV egies (from 34,254 to 37,126). Of the 5 HPV
negative and ASC-US/HPV negative continued routine screening. Strategy 4, also a recommended
cotesting strategy, referred to colposcopy women who were ASC-US/HPV positive and LSIL or more 4™™™™™™™™™™™™™™™™™™™™™™™
severe irrespective of HPV result, as well as all women who were cytology negative/HPV 16/HPV 18 not HPV 16/HPV 18 positive had 12 month fol-
positive. Women who were cytology negative/HPV positive but not positive for HPV 16 or HPV 18 had low-up.
repeat cotesting in 12 months, and women who were cytology negative/HPV negative and ASC-US/ ASC-US, atypical squamous cells of undetermined significance;
HPV negative continued with routine screening. Strategy 5 was similar to strategy 4 except that the HPV, human papillomavirus; LSIL, low-grade squamous intraepi-
thelial lesion.
threshold for referral to colposcopy was LSIL or more severe or cytology negative/HPV 16/HPV 18 Cox. Cervical cancer screening strategies: evaluation of results
positive or ASC-US/HPV 16/HPV 18 positive, whereas ASC-US or negative cytology/HPV positive but from the ATHENA HPV study. Am J Obstet Gynecol 2013.
MARCH 2013 American Journal of Obstetrics & Gynecology 184.e4
Research General Gynecology www.AJOG.org
strategies, HPV alone (strategy 6) had the
FIGURE 3
highest relative sensitivity and lowest relative
HPV screening algorithms specificity for CIN2 or more severe (1.68 and
Strategy 6: HPV alone 0.71, respectively), whereas HPV with cytol-
ogy triage (strategy 7) and HPV with geno-
Neg Routine screening typing triage (strategy 8) had the highest rel-
HPV Test ative specificity (each 1.04) but the lowest
Pos Colposcopy relative sensitivity (0.92 and 0.85, res-
pectively).
Strategy 7: HPV with reflex to cytology Using genotyping to triage HPV-pos-
itive women to colposcopy (strategy 8)
slightly decreased sensitivity for CIN2 or
Neg Routine screening
Follow-up more severe compared with using cytol-
HPV Test NILM in 12 mo. ogy at an ASC-US threshold (strategy 7;
Pos Pap Test 43.6% vs 47.5%) but increased sensitiv-
≥ASC-US Colposcopy ity for CIN3 or more severe (53.4% vs
51.9%), indicating a trend toward in-
Strategy 8: HPV with genotyping creased predictive value of HPV 16/HPV
18 genotyping as a triage test compared
Routine screening with cytology.
Neg Of all the screening strategies, HPV
HPV Test with cytology triage (strategy 7) and
and 16/18 Colposcopy
Genotyping HPV16+/18+ HPV with genotyping triage (strategy 8)
12 Other
required both the least number of col-
HR+ Follow-up poscopies (596 and 580, respectively)
in 12 mo.
and the least number of colposcopies to
detect 1 CIN2 or more severe (approxi-
Strategy 9: HPV with genotyping and reflex cytology: ASC-US threshold
mately 5). However, both strategies had
relatively low baseline sensitivity.
Routine screening Strategies 8, 9, and 10 used HPV alone
Neg
HPV Test as the initial screen and incorporated
and 16/18 Colposcopy genotyping triage for HPV-positive
HPV16+/18+
Genotyping Follow-up women. Strategies 9 and 10 added cytol-
12 Other NILM in 12 mo.
HR+ Pap Test ogy triage for HPV-positive women who
were HPV 16/HPV 18 negative to in-
≥ASC-US Colposcopy crease baseline detection of CIN2 or
more severe caused by the other 12 HPV
Strategy 10: HPV with genotyping and reflex cytology: LSIL threshold
4™™™™™™™™™™™™™™™™™™™™™™™
Routine screening Women with any abnormal cytology ASC-US or
Neg more severe were also referred to colposcopy,
HPV Test whereas women who were cytology negative/
and 16/18 Colposcopy
HPV16+/18+ NILM & HPV positive for non–HPV 16/HPV 18 had 12
Genotyping Follow-up
ASC-US
12 Other in 12 mo. month follow-up. Strategy 10 screened initially
HR+ Pap Test with a panel of HPV plus genotyping for HPV 16 and
≥LSIL Colposcopy HPV 18, referring all women who were HPV 16/HPV
18 positive to colposcopy and reflex testing by cy-
Strategies 6-10 screened initially with HPV testing. Strategy 6 referred all HPV-positive women to tology those HPV positive but not positive for HPV
colposcopy and all HPV-negative women to routine screening. Strategy 7 reflex tested all HPV- 16/HPV 18. Women with LSIL or more severe were
positive women with cytology, referring to colposcopy only those with ASC-US or more severe, also referred to colposcopy, whereas women who
whereas those with negative cytology had follow-up in 12 months. Strategy 8 screened initially with were cytology negative/HPV positive and ASC-US/
a panel of HPV plus genotyping for HPV 16 and HPV 18, referring to colposcopy all women testing HPV positive for non–HPV 16/HPV 18 had 12
positive for HPV 16 and/or HPV 18 and to 12 month follow-up women positive for other HPV month follow-up.
genotypes but not positive for HPV 16/HPV 18. Strategy 9 screened initially with a panel of HPV plus ASC-US, atypical squamous cells of undetermined significance;
genotyping for HPV 16 and HPV 18, referring all women who were HPV 16/HPV 18 positive to HPV, human papillomavirus.
Cox. Cervical cancer screening strategies: evaluation of results
colposcopy and reflex testing by cytology those HPV positive but not positive for HPV 16/HPV 18. from the ATHENA HPV study. Am J Obstet Gynecol 2013.
184.e5 American Journal of Obstetrics & Gynecology MARCH 2013
www.AJOG.org General Gynecology Research
The 4 strategies in the middle group
TABLE 1 (strategies 4, 5, 9, and 10) demonstrated
Demographic and clinical characteristics of ATHENA a narrow range of sensitivity (66.7–
population aged 30 years or older at baseline 76.2%) but varied by 33% in the number
Evaluable subjects of colposcopies (810 –1202). Within this
Characteristics (n ⴝ 34,254) group, cotesting with genotyping and cy-
Age, y tology triage at the ASC-US HPV-posi-
...................................................................................................................................................................................................................................
Mean ⫾ (SD) 44.7 ⫾ (10.1) tive threshold (strategy 4) was the most
...................................................................................................................................................................................................................................
sensitive but also required the most col-
30-39, n (%) 12,248 (35.8)
................................................................................................................................................................................................................................... poscopies. HPV with genotyping and cy-
ⱖ40, n (%) 22,006 (64.2) tology triage at the LSIL threshold (strat-
............................................................................................................................................................................................................................................
Race, n (%) egy 10) was the least sensitive and
...................................................................................................................................................................................................................................
White 28,821 (84.1) required the fewest colposcopies. Cotest-
...................................................................................................................................................................................................................................
ing with genotyping and cytology triage
Black or African American 4503 (13.1)
................................................................................................................................................................................................................................... with LSIL (strategy 5) and HPV with
Asian 503 (1.5) genotyping and reflex cytology triage
...................................................................................................................................................................................................................................
American Indian or Alaskan native 184 (0.5) with ASC-US (strategy 9) were very sim-
...................................................................................................................................................................................................................................
Native Hawaiian or other Pacific 78 (0.2) ilar in both sensitivity and number of
Islander colposcopies, but strategy 5 required
...................................................................................................................................................................................................................................
a nearly twice the number of initial screen-
Any combination/missing 165 (0.5)
............................................................................................................................................................................................................................................ ing tests (Tables 2 and 3).
Ethnicity, n (%)
...................................................................................................................................................................................................................................
Hispanic or Latino 6144 (17.9)
...................................................................................................................................................................................................................................
C OMMENT
Postmenopausal, n (%) 12,743 (37.2)
...................................................................................................................................................................................................................................
The ideal cervical cancer screening strat-
HPV vaccine, n (%) 50 (0.1)
............................................................................................................................................................................................................................................ egy would provide maximum sensitivity
Immunocompromised or 224 (0.7) to minimize missing disease as well as
immunosuppressed, n (%)
............................................................................................................................................................................................................................................ maximum specificity to minimize false
Family history of cervical disease positive results and overreferral. Unfor-
related to cervical cancer, n (%)
................................................................................................................................................................................................................................... tunately, cervical cancer screening strat-
Yes 1920 (5.6) egies that maximize both sensitivity and
...................................................................................................................................................................................................................................
No 31,988 (93.4) specificity have proven elusive because
...................................................................................................................................................................................................................................
Unknown 346 (1.0) strategies that maximize sensitivity have
............................................................................................................................................................................................................................................
typically produced relatively poor speci-
Pap cytology test in past 5 y, n (%) 31,089 (90.8)
............................................................................................................................................................................................................................................ ficity. The development of invasive cer-
ATHENA, Addressing the Need for Advanced HPV Diagnostics; Pap, Papanicolaou. vical cancer is typically a slow process
a
“Any combination/missing” refers to participants who selected more than 1 race or for whom the information was missing.
that takes decades rather than years to
Cox. Cervical cancer screening strategies: evaluation of results from the ATHENA HPV study. Am J Obstet Gynecol
2013. occur.8 This fact reduces the relative
benefits of achieving maximum sensitiv-
ity if poor specificity can lead to potential
types, thereby reducing the number of Figure 4 demonstrates in graphical harm.
cases deferred for identification to 12 form the trade-offs between sensitivity The recent ACS/ASCCP/ASCP cervi-
month follow-up. This produced a gain for CIN3 or more severe and the number cal cancer screening guidelines specifi-
in sensitivity of approximately 14-20% of colposcopies that each strategy would cally acknowledge that the benefits of
when compared with that achieved by produce. Presenting the data in this screening should be balanced against the
strategy 8. Of these 2 strategies, strategy 9 manner delineates 3 groups. One in- potential harms, with the total number
cludes a single strategy, HPV alone, of colposcopies serving as the primary
was more sensitive than strategy 10 for
which was significantly more sensitive measure of harm.2 Colposcopy was cho-
CIN2 or more severe (63.6% vs 57.9%)
than all the other strategies but is also the sen as the measure of harm because it has
and CIN3 or more severe (72.0% vs
least efficient, as measured by the num- been shown to be associated with consid-
66.7%) but slightly less specific (85.2% ber of colposcopies. In contrast, the 5 erable psychological distress, physical
vs 88.0% and 85.7% vs 88.5%, respec- strategies grouped with the lowest sensi- discomfort during the procedure, and
tively, for CIN2 or more severe and CIN3 tivity for CIN3 or more severe (strategies the potential to lead to more invasive
or more severe) because of the lower 1, 2, 3, 7, and 8) required the lowest treatments with short- and long-term
threshold for referral to colposcopy of number of colposcopies overall, with the risks.2 The baseline data from the
ASC-US, as opposed to LSIL. exception of cytology alone (strategy 2). ATHENA study provide us with an ex-
MARCH 2013 American Journal of Obstetrics & Gynecology 184.e6
Research General Gynecology www.AJOG.org
TABLE 2
Clinical outcomes of different strategies for detection of CIN2 or more severe
Colposcopies Cases identified Sensitivity Specificity
Tests to detect 1 CIN2 or more for 12 month relative to False- relative to
Strategy number and performed, Colposcopies CIN2 or more severe cases follow-up Sensitivity, ASC-US positive ASC-US
name n performed, n severe, n identified, n (estimated), n % triage rate, % triage
1 Cytology with reflex 35,546 816 5.7 144 0 51.4 1.00 12.0 1.00
HPV (ASC-US triage)
................................................................................................................................................................................................................................................................................................................................................................................
2 Cytology alone 34,254 1644 11.0 149 0 53.2 1.03 26.6 0.83
................................................................................................................................................................................................................................................................................................................................................................................
3 Cotesting with reflex 68,508 816 5.7 144 109 51.4 1.00 12.0 1.00
for ASC-US
................................................................................................................................................................................................................................................................................................................................................................................
4 Cotesting with 68,508 1202 6.4 189 64 67.5 1.31 18.0 0.93
genotyping and
cytology triage: HPV
16/HPV 18 and ASC-
US HPV-positive
threshold
................................................................................................................................................................................................................................................................................................................................................................................
5 Cotesting with 68,508 1030 6.0 173 80 61.8 1.20 15.2 0.96
genotyping and
cytology triage: HPV
16/HPV 18 and LSIL
threshold
................................................................................................................................................................................................................................................................................................................................................................................
6 HPV alone 34,254 2341 9.7 242 0 86.4 1.68 37.3 0.71
................................................................................................................................................................................................................................................................................................................................................................................
7 HPV with reflex to 37,126 596 4.5 133 109 47.5 0.92 8.2 1.04
cytology
................................................................................................................................................................................................................................................................................................................................................................................
8 HPV with genotyping 34,254 580 4.8 122 120 43.6 0.85 8.1 1.04
................................................................................................................................................................................................................................................................................................................................................................................
9 HPV with genotyping 36,423 982 5.5 178 64 63.6 1.24 14.3 0.97
and reflex cytology:
ASC-US threshold
................................................................................................................................................................................................................................................................................................................................................................................
10 HPV with genotyping 36,423 810 5.0 162 80 57.9 1.13 11.5 1.00
and reflex cytology:
LSIL threshold
................................................................................................................................................................................................................................................................................................................................................................................
ASC-US, atypical squamous cells of undetermined significance; CIN, cervical intraepithelial neoplasia; HPV, human papillomavirus; LSIL, low-grade squamous intraepithelial lesion.
Cox. Cervical cancer screening strategies: evaluation of results from the ATHENA HPV study. Am J Obstet Gynecol 2013.
ceptional opportunity to evaluate both more severe and potential for harm be- CIN3 or more severe with only a modest
the benefit and potential harms that cause it results in 2-3 times more colpos- (less than 2-fold) increase in the required
would be produced during a single copies than the other strategies. Like- number of colposcopies compared with
round of screening using cervical cancer wise, the 5 strategies in the lowest tier the less sensitive strategies. All 4 of the
screening strategies based on various that are the least sensitive for detection of strategies that occupy the middle portion
combinations of cytology, pooled testing CIN3 or more severe would appear to be of the scatterplot use HPV testing with
for 12 high-risk HPV types, and geno- less attractive options for clinicians and genotyping for HPV 16/HPV 18, and 2
typing for HPV 16 and HPV 18. policy makers, despite the fact that all are cotesting strategies. Of these, cotest-
To evaluate trade-offs between sensi- but 1 strategy (cytology alone) offer the ing with genotyping triage (strategy 4)
tivity and potential harms of the differ- least potential for harm by requiring the is the most sensitive strategy but re-
ent screening strategies, we used a scat- lowest number of colposcopies. How- quires the most colposcopies and twice
terplot of each strategy’s sensitivity for ever, the low sensitivity of these strate- the initial tests as the non– cotesting
CIN3 or more severe vs the number of gies for detection of CIN3 or more severe options in this group, strategies 9 and
colposcopies required. The scatterplot at baseline increases the burden of cases 10. HPV with genotyping and cytology
delineates 3 tiers in the balance between that are missed at baseline and that bur- triage with LSIL (strategy 10) requires
sensitivity for CIN3 or more severe, or den would depend on potential identifi- the fewest colposcopies and therefore
benefit of each screening strategy, and cation for those strategies that have 12 would be most applicable in settings in
the number of colposcopies, a measure month follow-up. which potential harm from colposcopy
of potential harm. The most attractive strategies from the is of greater concern than benefit.
The most sensitive strategy, HPV perspective of a benefit-vs-harm analysis The 2 strategies within this tier that
alone with referral of all HPV-positive appear to be the 4 strategies occupying seem to optimize the balance between
women to colposcopy (strategy 6), does the middle portion of the scatterplot. sensitivity and specificity are cotesting
not appear to offer the right balance be- These strategies all combine what we with genotyping and cytology triage with
tween maximum detection of CIN3 or consider to be a reasonable sensitivity for LSIL (strategy 5) and HPV with genotyp-
184.e7 American Journal of Obstetrics & Gynecology MARCH 2013
www.AJOG.org General Gynecology Research
TABLE 3
Clinical outcomes of different strategies for the detection of CIN3 or more severe
Colposcopies Cases identified Sensitivity Specificity
Tests to detect 1 CIN3 or more for 12 month relative to False- relative to
Strategy number and performed, Colposcopies CIN3 or more severe cases follow-up Sensitivity, ASC-US positive ASC-US
name n performed, n severe, n identified, n (estimated), n % triage rate, % triage
1 Cytology with reflex 35,546 816 7.7 106 0 56.1 1.00 12.4 1.00
HPV (ASC-US
triage)
................................................................................................................................................................................................................................................................................................................................................................................
2 Cytology alone 34,254 1644 15.1 109 0 57.7 1.03 26.8 0.84
................................................................................................................................................................................................................................................................................................................................................................................
3 Cotesting with 68,508 816 7.7 106 72 56.1 1.00 12.4 1.00
reflex for ASC-US
................................................................................................................................................................................................................................................................................................................................................................................
4 Cotesting with 68,508 1202 8.3 144 34 76.2 1.36 18.5 0.93
genotyping and
cytology triage: HPV
16/HPV 18 and
ASC-US HPV-
positive threshold
................................................................................................................................................................................................................................................................................................................................................................................
5 Cotesting with 68,508 1030 7.7 134 44 70.9 1.26 15.7 0.96
genotyping and
cytology triage: HPV
16/HPV 18 and LSIL
threshold
................................................................................................................................................................................................................................................................................................................................................................................
6 HPV alone 34,254 2341 13.8 170 0 89.9 1.60 38.0 0.71
................................................................................................................................................................................................................................................................................................................................................................................
7 HPV with reflex to 37,126 596 6.1 98 72 51.9 0.92 8.7 1.04
cytology
................................................................................................................................................................................................................................................................................................................................................................................
8 HPV with 34,254 580 5.7 101 69 53.4 0.95 8.4 1.05
genotyping
................................................................................................................................................................................................................................................................................................................................................................................
9 HPV with 36,423 982 7.2 136 34 72.0 1.28 14.8 0.97
genotyping and
reflex cytology:
ASC-US threshold
................................................................................................................................................................................................................................................................................................................................................................................
10 HPV with 36,423 810 6.4 126 44 66.7 1.19 12.0 1.01
genotyping and
reflex cytology:
LSIL threshold
................................................................................................................................................................................................................................................................................................................................................................................
ASC-US, atypical squamous cells of undetermined significance; CIN, cervical intraepithelial neoplasia; HPV, human papillomavirus; LSIL, low-grade squamous intraepithelial lesion.
Cox. Cervical cancer screening strategies: evaluation of results from the ATHENA HPV study. Am J Obstet Gynecol 2013.
ing and cytology triage with ASC-US at enrollment by a given screening test with cytology alone almost doubling the
(strategy 9). The latter strategy results in would be detected on subsequent screen- number of required colposcopies.
a 50% reduction in the number of re- ing or follow-up. Multiple cost-effectiveness analyses
quired screening tests and is also slightly In a setting in which it would be consid- and metaanalyses have previously docu-
more sensitive and requires slightly ered unethical to follow up women with mented the attractiveness of cytology
fewer colposcopies to detect 1 CIN3 or known CIN3 or more severe lesions, a ran- with triage of ASC-US by HPV over a
more severe case. domized trial in which women are as- strategy of cytology with referral of all
An obvious limitation of this analysis signed to each of the different screening women with abnormal cytology results
is that it uses only the baseline data from strategies would be required to determine
to colposcopy.9-12 Likewise, the group of
the ATHENA trial and does not include exactly how subsequent rounds of fol-
screening strategies that appear to be the
the results of those women identified as low-up or screening would perform. We
most attractive after comparing benefits
needing 12 month follow-up. Because therefore consider it reassuring that our
the design of the ATHENA study re- approach of comparing benefits and and harms includes the strategy recently
ferred all women with abnormal screen- harms of different screening strategies ar- classified by the ACS as the preferred
ing test results at enrollment for colpos- rived at many of the same conclusions as strategy when screening women aged 30
copy, many women with CIN2 or more have analyses incorporating multiple years or older (cotesting).2
severe lesions missed by a given screen- rounds of screening and mathematical However, of the 2 cotesting strategies
ing test were identified by the other modeling studies. For example, in this recommended by the ACS/ASCCP/ASCP,
screening test, and their CIN2 or more analysis, a strategy of cytology with HPV cotesting with genotyping triage (strategy
severe lesions were treated. Therefore, it triage of ASC-US (strategy 1) is clearly su- 4) detects 26.4% more CIN3 or more se-
is impossible to know what percentage of perior to cytology alone (strategy 2) be- vere than cotesting with 12 month fol-
the CIN2 or more severe lesions missed cause both have similar sensitivities but low-up of all cytology-negative/HPV-posi-
MARCH 2013 American Journal of Obstetrics & Gynecology 184.e8
Research General Gynecology www.AJOG.org
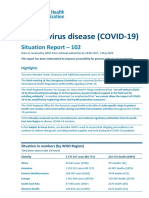
FIGURE 4
Sensitivity for CIN3 or more severe and number of colposcopies
Primary Screening Strategies For CIN3+ Endpoint
100.0
90.0 Strategy 6
80.0
Strategy 4
Strategy 9
70.0 Strategy 5
Strategy 10
60.0
Sensitivity (%)
Strategy 2
Strategy 1 or 3
Strategy 8
Strategy 7
50.0
40.0 Colposcopies, Initial tests
Strategy n Sensitivity, % performed, n
Strategy 1 816 56.1 35,546
30.0 Strategy 2 Cytology alone 1644 57.7 34,254
Strategy 3 816 56.1 68,508
Strategy 4 1202 76.2 68,508
20.0 Strategy 5 Cotesting with genotyping and cytology triage: HPV 16/18 and LSIL threshold 1030 70.9 68,508
Strategy 6 HPV alone 2341 89.9 34,254
Strategy 7 HPV with cytology triage 596 51.9 37,126
10.0 Strategy 8 HPV with genotyping triage 580 53.4 34,254
Strategy 9 HPV with genotyping and reflex cytology: ASC-US threshold 982 72.0 36,423
Strategy 10 HPV with genotyping and cytology (LSIL cut-off) triage 810 66.7 36,423
0.0
0 500 1000 1500 2000 2500
Number of Colposcopies
Scatterplot of sensitivity for CIN3 or more severe and number of colposcopies for each screening strategy. Clear outliers as measured by numbers of
colposcopies are in red. Strategies with the lowest sensitivity but also the lowest number of initial colposcopies are in black and those with intermediate
sensitivity and number of colposcopies are in blue. Strategies that are presently recommended in the American Society for Colposcopy and Cervical
Pathology guidelines are in bold.
ASC-US, atypical squamous cells of undetermined significance; CIN, cervical intraepithelial neoplasia; HPV, human papillomavirus; LSIL, low-grade squamous intraepithelial lesion.
Cox. Cervical cancer screening strategies: evaluation of results from the ATHENA HPV study. Am J Obstet Gynecol 2013.
tive women (strategy 3) but requires women who are followed up and un- but, in contrast to our results, was also
nearly 50% more colposcopies at the ini- dergo cotesting 12 months later will re- more sensitive.17 Naucler et al18 evaluated
tial round of screening. Although this quire colposcopy because of persistent 11 screening strategies using data from a
would appear to significantly increase high-risk HPV infections.15 Swedish screening trial and found that
potential harm when compared with Previous studies have shown other HPV with cytology triage and repeat HPV
cotesting without genotyping, this op- screening strategies to be effective.14,16-21 testing at 1 year of cytology-negative/
tion obviates the need for repeat cotest- Analysis of data from a Finnish screening HPV-positive women was the most feasi-
ing in 12 months for women positive for trial demonstrated that triage of HPV- ble of the screening strategies. Similarly, a
HPV 16/18 and reduces the risk of de- positive women by cytology (strategy 7), large population-based screening trial in
layed diagnosis and or loss to follow-up as in the ATHENA trial, was more spe- The Netherlands (VUSA-Screen Study)
of women with significant disease.13,14 cific than conventional cytology screen- also found HPV with cytology triage and 1
Moreover, approximately half of the ing and decreased colposcopy referrals year follow-up by repeat cytology of HPV-
184.e9 American Journal of Obstetrics & Gynecology MARCH 2013
www.AJOG.org General Gynecology Research
positive women to be a feasible alternative HPV types also need to be addressed, ACKNOWLEDGMENTS
to cytology screening.14 such as whether HPV 45, which shows a We thank Teresa Wright, MD, for her valuable
It is difficult to compare these analyses similar predilection for adenocarcinoma contributions to the design and execution of the
ATHENA HPV Study and for assistance in the
with ours because they are based on 1-5 as HPV 18, should be managed in the
analysis of data. The ATHENA study testing
year follow-up data, and each of these same way as HPV 18. sites and participants include the following:
studies had quite different study designs The strategies with 12 month follow-up United States, Comprehensive Clinical Trials,
compared with ATHENA. Moreover, for women at intermediate risk will in- West Palm Beach, FL; Green Clinic, Ruston,
neither the Finnish nor The Netherlands crease both the ultimate sensitivity of each LA; Philadelphia Clinical Research, Philadel-
trials evaluated strategies that included of these strategies as well as the total num- phia, PA; Visions Clinical Research, Boynton
Beach, FL; Women’s Health Specialist, Costa
HPV 16/HPV 18 genotyping. It should be ber of colposcopies and must also take into Mesa, CA; Mount Vernon Clinical Research, At-
stressed, however, that the ATHENA base- account loss to follow-up. Hence, any lanta, GA; Tennessee Women’s Care, Nash-
line data do not support a conclusion that strategy selected should consider the trade- ville, TN; Chattanooga Medical Research, Chat-
HPV with cytology triage is competitive offs of sensitivity and specificity in the con- tanooga, TN; OB/GYN Specialists of the Palm
with any of the HPV 16/HPV 18 genotyp- text of real-world clinical practice. As illus- Beaches, West Palm Beach, FL; Segal Institute
for Clinical Research, North Miami, FL; South
ing strategies that include cytology, unless trated by Kitchener et al,23 poor follow-up
Carolina Clinical Research Center, Columbia,
an absolute reduction in baseline colpos- of HPV-positive women not sent immedi- SC; Bluegrass Clinical Research, Louisville, KY;
copies is the primary goal. In addition, an- ately to colposcopy could negate some of Delaware Valley OB-GYN and Infertility Group,
other recent report from a large screening the benefits of HPV testing to identify Plainsboro, NJ; Advanced Research Associ-
population in The Netherlands (Popula- women at risk for CIN2 or more severe ates, Corpus Christi, TX; Advanced Clinical
tion-Based Screening Study Amsterdam while leaving unaffected the added safety Concepts, West Reading, PA; Miami Research
Associates, Miami, FL; Center for Women’s
[POBASCAM]) has documented that of a negative HPV test. Within the context Health of Lansdale, Lansdale, PA; Blue Skies
early detection of CIN3 or more severe as- of poor follow-up of screen-positive pa- Center for Women, Colorado Springs, CO; Vi-
sociated with HPV 16 was a major compo- tients, more sensitive methods of manag- sions Clinical Research, Tucson, AZ; Impact
nent of the benefit of testing for HPV.19 ing HPV-positive women may be pre- Clinical Trials, Las Vegas, NV; Physicians’ Re-
Other more complex HPV genotype– ferred over methods with increased search Options, Lakewood, CO; Four Rivers
Clinical Research, Paducah, KY; Medical Net-
based approaches may further improve specificity and PPV, so that the opportu-
work for Education and Research, Decatur, GA;
upon these strategies. In particular, sev- nity for immediate detection and treat- Women’s Health Research, Phoenix, AZ; Im-
eral studies, including ATHENA, have ment of precancerous lesions will not be pact Clinical Trials, Los Angeles, CA; HWC
shown that HPV 16 has a much higher missed. Women’s Research Center, Englewood, OH;
baseline positive predictive value (PPV) In conclusion, this analysis demon- Texas Medical Center, Houston, TX; Mobile
OB/GYN, Mobile, AL; Altus Research, Lake
than the other high-risk types and that, strates that multiple cervical cancer
Worth, FL; Tacoma Women’s Specialist, Ta-
at least cross-sectionally, HPV 18 has a screening strategies are more effective coma, WA; Phoenix OB-GYN Association,
similar PPV to the pool of 12 other high- than the present standard of cytology Moorestown, NJ; The Woman’s Clinic, Boise,
risk types.4,5,7 This raises the question as screening with ASC-US triage. Strategies ID; Impact Clinical Trials, Los Angeles, CA;
to whether HPV 18 –positive women that maximize early detection of CIN3 or eCast Corp, North Charleston, SC; State of
would be more efficiently managed by more severe without excessive increases Franklin Healthcare Associates Research,
Johnson City, TN; Quality of Life Medical and
short-term (6-12 months) repeat testing in initial screening tests and colposco- Research Center, Tucson, AZ; Eastern Carolina
for HPV 18 to establish persistence be- pies, yet also identify women at interme- Women’s Center, New Bern, NC; Tidewater
fore referral to colposcopy, similar to the diate risk in need of 12 month follow-up, Clinical Research, Virginia Beach, VA; St John’s
management of women positive for one would appear to provide optimal bal- Center for Clinical Research, Jacksonville, FL,
of the other 12 high-risk HPV types. ance between benefit and harms. Of R. Myers; M and O Clinical Research, Ft. Lau-
derdale, FL; Lyndhurst Gynecologic Associ-
However, HPV 18 is associated more these options, strategies that incorporate
ates, PA, Winston-Salem, NC; Enterprise
with cancer than these other types22 and initial screening with HPV and triage of Women’s Center, Enterprise, AL; Salt Lake Re-
also is associated with endocervical le- HPV-positive women by a combination search, Salt Lake City, UT; Women’s Health
sions that are difficult to detect. of genotyping for HPV 16/HPV 18 and Care at Frost Street, San Diego, CA; Atlanta
In ATHENA, 3 of the 6 cancers de- cytology may best fulfill these require- North Gynecology Center for Research, Ro-
tected at baseline were HPV 18 positive, ments for more balanced screening, al- swell, GA; Women’s Clinical Research, New-
burgh, IN; Jacksonville Center for Clinical Re-
as were 8 of the 16 adenocarcinoma in though other options may also be com- search, Jacksonville, FL; Women’s OB-GYN,
situ cases and 1 cancer detected in fol- pelling in different settings. When the 3 Saginaw, MI; Clinical Research Consultants,
low-up.6 So although the PPV for CIN3 year follow-up data from ATHENA be- Hoover, AL; Edinger Medical Group Research
or more severe of a positive HPV 18 test come available, formal cost-effectiveness Center, Fountain Valley, CA; Health Awareness,
at baseline is lower than typically recom- modeling can be performed to better de- Jupiter, FL; Physician Care Clinical Research,
Sarasota, FL; Woman’s Health Practice, Cham-
mended for immediate colposcopy, the termine the benefits of cervical cancer
paign, IL; Clinical Trials Management, Coving-
greater severity of the disease burden screening strategies that incorporate ton, LA; Advanced Research Associates, Dal-
substantiates this approach. Other ques- HPV with genotyping for HPV 16/HPV las, TX; Fellows Research Alliance, Savannah,
tions related to the behavior of different 18 and cytology. f GA; Fellows Research Alliance, Hilton Head,
MARCH 2013 American Journal of Obstetrics & Gynecology 184.e10
Research General Gynecology www.AJOG.org
SC; Women’s Care Florida, Tampa, FL; Ad- for the triage of women with high-risk HPV⫹ and implications for clinical focus on persistent
vanced Research Associates, McAllen, TX; Pre- cytology-negative results. Am J Clin Pathol infections. J Natl Cancer Inst 2008;100:513-7.
cision Trials, Phoenix, AZ; and Yassear Clinical 2011;136:578-86. 16. Cuzick J, Szarewski A, Mesher D, et al.
Research, Carmichael, CA. 8. McCredie MR, Sharples KJ, Paul C, et al. Long-term follow-up of cervical abnormalities
Natural history of cervical neoplasia and risk of among women screened by HPV testing and
invasive cancer in women with cervical intraepi- cytology-Results from the Hammersmith study.
REFERENCES thelial neoplasia 3: a retrospective cohort study. Int J Cancer 2008;122:2294-300.
1. Moyer VA, on behalf of the US Preventive Lancet Oncol 2008;9:425-34. 17. Leinonen M, Nieminen P, Kotaniemi-Tal-
Services Task Force. Screening for cervical 9. Kim JJ, Wright TC, Goldie SJ. Cost-effective- onen L, et al. Age-specific evaluation of primary
cancer: US Preventive Services Task Force ness of alternative triage strategies for atypical human papillomavirus screening vs conven-
Recommendation Statement. Ann Intern Med squamous cells of undetermined significance. tional cytology in a randomized setting. J Natl
2012;156:880-91, W312. JAMA 2002;287:2382-90. Cancer Inst 2009;101:1612-23.
2. Saslow D, Solomon D, Lawson HW, et al. Amer- 10. Kim JJ, Wright TC, Goldie SJ. Cost-effec- 18. Naucler P, Ryd W, Tornberg S, et al. Effi-
ican Cancer Society, American Society for Colpos- tiveness of human papillomavirus DNA testing cacy of HPV DNA testing with cytology triage
copy and Cervical Pathology, and American Society in the United Kingdom, The Netherlands, and/or repeat HPV DNA testing in primary cer-
for Clinical Pathology screening guidelines for the France, and Italy. J Natl Cancer Inst 2005; vical cancer screening. J Natl Cancer Inst
prevention and early detection of cervical cancer. 2009;101:88-99.
97:888-95.
Am J Clin Pathol 2012;137:516-42. 19. Rijkaart DC, Berkhof J, Rozendaal L, et al.
11. Kulasingam SL, Kim JJ, Lawrence WF, et
3. American College of Obstetrics and Gyne- Human papillomavirus testing for the detection
al. Cost-effectiveness analysis based on the
cology. Cervical cancer recommendations. of high-grade cervical intraepithelial neoplasia
atypical squamous cells of undetermined signif-
Available at: http://www.acog.org/About_ACOG/ and cancer: final results of the POBASCAM ran-
icance/low-grade squamous intraepithelial le-
Announcements/New_Cervical_Cancer_Screening_ domised controlled trial. Lancet Oncol 2012;
sion Triage Study (ALTS). J Natl Cancer Inst
recommendations. Accessed June 1, 2012. 13:78-88.
2006;98:92-100.
4. Stoler MH, Wright TC Jr, Sharma A, et al. 20. Ronco G, Giorgi-Rossi P, Carozzi F, et al.
12. Arbyn M, Sasieni P, Meijer CJ, Clavel C,
High-risk human papillomavirus testing in Efficacy of human papillomavirus testing for
Koliopoulos G, Dillner J. Chapter 9: clinical ap- the detection of invasive cervical cancers and
women with ASC-US cytology: results from the
ATHENA HPV study. Am J Clin Pathol 2011; plications of HPV testing: a summary of meta- cervical intraepithelial neoplasia: a ran-
135:468-75. analyses. Vaccine 2006;24(Suppl 3):S3/78, domised controlled trial. Lancet Oncol 2010;
5. Castle PE, Stoler MH, Wright TC Jr, Sharma S3/89. 11:249-57.
A, Wright TL, Behrens CM. Performance of car- 13. Kinney W, Fetterman B, Cox JT, Lorey T, 21. Sankaranarayanan R, Nene BM, Shastri
cinogenic human papillomavirus (HPV) testing Flanagan T, Castle PE. Characteristics of 44 SS, et al. HPV screening for cervical cancer in
and HPV16 or HPV18 genotyping for cervical cervical cancers diagnosed following Pap-neg- rural India. N Engl J Med 2009;360:1385-94.
cancer screening of women aged 25 years and ative, high risk HPV-positive screening in routine 22. de Sanjose S, Quint WG, Alemany L, et al.
older: a subanalysis of the ATHENA study. Lan- clinical practice. Gynecol Oncol 2011;121: Human papillomavirus genotype attribution in
cet Oncol 2011;12:880-9. 309-13. invasive cervical cancer: a retrospective cross-
6. Wright TC Jr, Stoler MH, Behrens CM, Apple 14. Rijkaart DC, Berkhof J, van Kemenade FJ, sectional worldwide study. Lancet Oncol
R, Derion T, Wright TL. The ATHENA human et al. HPV DNA testing in population-based cer- 2010;11:1048-56.
papillomavirus study: design, methods, and vical screening (VUSA-Screen study): results 23. Kitchener HC, Almonte M, Thomson C, et
baseline results. Am J Obstet Gynecol 2012; and implications. Br J Cancer 2012;106: al. HPV testing in combination with liquid-based
206:46.e1-11. 975-81. cytology in primary cervical screening (ARTIS-
7. Wright TC Jr, Stoler MH, Sharma A, et al. 15. Rodriguez AC, Schiffman M, Herrero R, et TIC): a randomised controlled trial. Lancet On-
Evaluation of HPV-16 and HPV-18 genotyping al. Rapid clearance of human papillomavirus col 2009;10:672-8.
184.e11 American Journal of Obstetrics & Gynecology MARCH 2013
You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (843)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5810)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (346)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Cesarean SectionDocument11 pagesCesarean SectionChristine SaliganNo ratings yet
- Safe Management of Wastes From Healthcare ActivitiesDocument330 pagesSafe Management of Wastes From Healthcare Activitiesrsia mitra husada100% (1)
- AFMC PrimerDocument523 pagesAFMC PrimerRahma100% (1)
- LESSON PLAN Waste DisposalDocument17 pagesLESSON PLAN Waste Disposalshaila100% (2)
- Shortness of BreathDocument4 pagesShortness of BreathImanuel Far-FarNo ratings yet
- Hypothyroid PIR 2009Document10 pagesHypothyroid PIR 2009Imanuel Far-FarNo ratings yet
- Familial NSDocument10 pagesFamilial NSImanuel Far-FarNo ratings yet
- Tolerance of Partially Hydrolyzed Whey Formula in Cow's Milk Allergic PatientsDocument1 pageTolerance of Partially Hydrolyzed Whey Formula in Cow's Milk Allergic PatientsImanuel Far-FarNo ratings yet
- Dhar, 2016 Food Allergy in Atopic DermatitisDocument6 pagesDhar, 2016 Food Allergy in Atopic DermatitisImanuel Far-FarNo ratings yet
- CASTRO-JUNIOR, Oral Tolerance Correlates With High Levels of Lymphocyte ActivityDocument11 pagesCASTRO-JUNIOR, Oral Tolerance Correlates With High Levels of Lymphocyte ActivityImanuel Far-FarNo ratings yet
- Dengue Fever and PregnancyDocument6 pagesDengue Fever and PregnancyImanuel Far-FarNo ratings yet
- Avian Influenza Case StudyDocument8 pagesAvian Influenza Case StudyAatif HussainNo ratings yet
- Module 2 National Immunization Program (Npi) - MihpDocument15 pagesModule 2 National Immunization Program (Npi) - MihpNurhaifa Mocadema100% (1)
- USFWS 2022 Avian Influenza FactsheetDocument2 pagesUSFWS 2022 Avian Influenza FactsheetinforumdocsNo ratings yet
- Long and Short Interpregnancy Intervals Increase Severe Maternal MorbidityDocument8 pagesLong and Short Interpregnancy Intervals Increase Severe Maternal Morbiditynurul asyikin abdullahNo ratings yet
- Hubungan Riwayat Pajanan Pestisida Dengan Kejadian Diabetes Melitus Tipe 2 Pada Petani Penyemprot Di Kecamatan Ngablak Kabupaten MagelangDocument10 pagesHubungan Riwayat Pajanan Pestisida Dengan Kejadian Diabetes Melitus Tipe 2 Pada Petani Penyemprot Di Kecamatan Ngablak Kabupaten MagelangATHIRA FAHRANI RISAL GiziNo ratings yet
- Thesis On Cervical CancerDocument8 pagesThesis On Cervical Cancerveronicapadillaalbuquerque100% (3)
- Health Assessment QuestionnaireDocument3 pagesHealth Assessment QuestionnaireAshoka1988No ratings yet
- A Technical Report On ITDocument34 pagesA Technical Report On ITFeddy Micheal FeddyNo ratings yet
- Emergency Use Authorization (EUA) For An Unapproved Product Review Memorandum Identifying InformationDocument57 pagesEmergency Use Authorization (EUA) For An Unapproved Product Review Memorandum Identifying InformationNicoleta Eugenia BursucNo ratings yet
- Head Boy 0-36Document1 pageHead Boy 0-36Almira ClaraNo ratings yet
- Journal of Public HealthDocument5 pagesJournal of Public HealthAhmad Muzakkir ZainaniNo ratings yet
- Breastfeeding Your Little OneDocument12 pagesBreastfeeding Your Little OneCalvin LooNo ratings yet
- 11 Form DR Write Up Rev July 2013.doc Revised 7 29 16Document1 page11 Form DR Write Up Rev July 2013.doc Revised 7 29 16Illya AnnesyNo ratings yet
- Reference: J. D. Robinson Formula (1983)Document1 pageReference: J. D. Robinson Formula (1983)muhammadkhirNo ratings yet
- Birthing PlanDocument6 pagesBirthing PlanLuna GrayNo ratings yet
- Exercise Guidelines Cancer Infographic PDFDocument1 pageExercise Guidelines Cancer Infographic PDFYina Marcela Quintero OrtegaNo ratings yet
- Annotated Bibliography Graphic OrganizerDocument4 pagesAnnotated Bibliography Graphic Organizerapi-348035481No ratings yet
- Case 1 - Pneumonia (Final)Document4 pagesCase 1 - Pneumonia (Final)Joegie ArioNo ratings yet
- Shetty Darshana NileshDocument1 pageShetty Darshana NileshBipin JenaNo ratings yet
- Moving Target Vaccines Thimerosol and AutismDocument25 pagesMoving Target Vaccines Thimerosol and AutismcirclestretchNo ratings yet
- Review Scrutiny Result ListDocument35 pagesReview Scrutiny Result ListSARKAR JAVED AKHTARNo ratings yet
- Analysis of Germ TheoryDocument6 pagesAnalysis of Germ TheorylucasvanderlaanNo ratings yet
- Coronavirus Disease (COVID-19) : Situation Report - 102Document16 pagesCoronavirus Disease (COVID-19) : Situation Report - 102CityNewsTorontoNo ratings yet
- Patogenesis Dan Manifestasi Klinik HepatitisDocument91 pagesPatogenesis Dan Manifestasi Klinik HepatitisFaulina Yosia PanjaitanNo ratings yet
- WHO - The Second Ten Years of The World Health OrganizationDocument456 pagesWHO - The Second Ten Years of The World Health OrganizationFloripondio19No ratings yet
- Appendix C3 - CT Application FormDocument4 pagesAppendix C3 - CT Application FormRuel Vincent AsubarNo ratings yet