You might also like
- Chi Et Al - 2013 - An Update On Pulmonary Complications of Hematopoietic Stem Cell TransplantationDocument10 pagesChi Et Al - 2013 - An Update On Pulmonary Complications of Hematopoietic Stem Cell TransplantationRutvik ShahNo ratings yet
- 1 s2.0 S1878788616300297 MainDocument10 pages1 s2.0 S1878788616300297 Mainsarahloba100No ratings yet
- Delay in Diagnosis of Extra-Pulmonary Tuberculosis by Its Rare Manifestations: A Case ReportDocument5 pagesDelay in Diagnosis of Extra-Pulmonary Tuberculosis by Its Rare Manifestations: A Case ReportSneeze LouderNo ratings yet
- Research Article: Neutropenic Sepsis in The ICU: Outcome Predictors in A Two-Phase Model and Microbiology FindingsDocument9 pagesResearch Article: Neutropenic Sepsis in The ICU: Outcome Predictors in A Two-Phase Model and Microbiology Findings28121998No ratings yet
- Ijhbr January 2018 23-30Document8 pagesIjhbr January 2018 23-30farhanomeNo ratings yet
- Central Nervous System Infection Following Allogeneic Hematopoietic Stem Cell TransplantationDocument7 pagesCentral Nervous System Infection Following Allogeneic Hematopoietic Stem Cell Transplantationadilla kusumaNo ratings yet
- Venous Thromboembolism in The ICU: Main Characteristics, Diagnosis and ThromboprophylaxisDocument9 pagesVenous Thromboembolism in The ICU: Main Characteristics, Diagnosis and ThromboprophylaxisCourtneykdNo ratings yet
- Thromboembolic Complications After Splenectomy For Hematologic DiseasesDocument5 pagesThromboembolic Complications After Splenectomy For Hematologic DiseasesDipen GandhiNo ratings yet
- Journal of Cardiovascular Medicine and CardiologyDocument2 pagesJournal of Cardiovascular Medicine and CardiologyPeertechz Publications Inc.No ratings yet
- 2017 Article 996-2Document8 pages2017 Article 996-2chameleonNo ratings yet
- Diagnostic Challenges in CervicalDocument6 pagesDiagnostic Challenges in CervicalOgi Y. Casesarando PurbaNo ratings yet
- 1 TransplantationDocument26 pages1 TransplantationAhmed SaeedNo ratings yet
- Fichamento para Introduçao: Thromboembolism: A Public Health Concern. American Journal of Preventive Medicine, DefiniçãoDocument20 pagesFichamento para Introduçao: Thromboembolism: A Public Health Concern. American Journal of Preventive Medicine, Definiçãolarissam123No ratings yet
- First - in - Man Observation of Talaromyces Marneffei-Transmission by Organ TransplantationDocument5 pagesFirst - in - Man Observation of Talaromyces Marneffei-Transmission by Organ TransplantationAnonymous oQtve4oNo ratings yet
- Radiologic Manifestations of Pulmonary Tuberculosis in Patients of Intensive Care UnitsDocument6 pagesRadiologic Manifestations of Pulmonary Tuberculosis in Patients of Intensive Care UnitsAnonymous qwH3D0KrpNo ratings yet
- Clinical Cases in Chronic Thromboembolic Pulmonary HypertensionFrom EverandClinical Cases in Chronic Thromboembolic Pulmonary HypertensionWilliam R. AugerNo ratings yet
- PneumoniaDocument30 pagesPneumoniacasemix rsummNo ratings yet
- 4Document16 pages4Ihsanul Ma'arifNo ratings yet
- DVT in India PDFDocument6 pagesDVT in India PDFKarthik KoneruNo ratings yet
- Benefit of CT Scanning For Assessing Pulmonary Disease in The Immunodepressed PatientDocument6 pagesBenefit of CT Scanning For Assessing Pulmonary Disease in The Immunodepressed PatienthilalNo ratings yet
- Periodontal TreatmentDocument21 pagesPeriodontal TreatmentAdyas AdrianaNo ratings yet
- Pi Is 0140673621016081Document10 pagesPi Is 0140673621016081Ahmed BahloulNo ratings yet
- Trali, Taco and TadDocument45 pagesTrali, Taco and Taddr AmitNo ratings yet
- Pulmonary Miliary Tuberculosis Complicated With Tuberculous Spondylitis An Extraordinary Rare Association: A Case ReportDocument5 pagesPulmonary Miliary Tuberculosis Complicated With Tuberculous Spondylitis An Extraordinary Rare Association: A Case ReportIsmail Eko SaputraNo ratings yet
- Jasim2018 PDFDocument8 pagesJasim2018 PDFCorona FingerNo ratings yet
- GV1111HDDocument16 pagesGV1111HDgabrielnavarretefNo ratings yet
- CNS InfectionDocument6 pagesCNS InfectionAnonymous nruHyuwtJNo ratings yet
- 10.1007@s00330 019 06235 3Document11 pages10.1007@s00330 019 06235 3Ysik KbreraNo ratings yet
- London F, Acta Neurol Belg, 2023Document4 pagesLondon F, Acta Neurol Belg, 2023Fabrizio Quiñonez FlorentinNo ratings yet
- Extrapulmonary Tuberculosis: Key PointsDocument6 pagesExtrapulmonary Tuberculosis: Key PointsRetno ManggalihNo ratings yet
- Prediction of Thrombotic and Hemorrhagic Events During Polycythemia TR 2015Document6 pagesPrediction of Thrombotic and Hemorrhagic Events During Polycythemia TR 2015amara.ablaNo ratings yet
- HemoptysisDocument3 pagesHemoptysisjerwin01041No ratings yet
- Risk Factors For Intraoperative Massive Transfusion in Pediatric Liver Transplantation: A Multivariate AnalysisDocument8 pagesRisk Factors For Intraoperative Massive Transfusion in Pediatric Liver Transplantation: A Multivariate AnalysisSanti ParambangNo ratings yet
- C PDFDocument9 pagesC PDFSasqia Rakhmi LeonyNo ratings yet
- Neutrophil Dysregulation During SepsisDocument11 pagesNeutrophil Dysregulation During SepsisUntuk DownloadNo ratings yet
- Outcome of The Treatment of Hydatid Disease in Children Over A Period of 8 YearsDocument8 pagesOutcome of The Treatment of Hydatid Disease in Children Over A Period of 8 YearsSabrina JonesNo ratings yet
- Epoc y TEPDocument9 pagesEpoc y TEPHernan GonzalezNo ratings yet
- Malignancies of The Colorectum and Anus in Solid Organ RecipientsDocument8 pagesMalignancies of The Colorectum and Anus in Solid Organ RecipientsDaniel Alfonso GamezNo ratings yet
- Akci̇ğer TransplantasyonuDocument17 pagesAkci̇ğer TransplantasyonuAhmet PinarbasiNo ratings yet
- Early Ambulation and Prevention of Post-Operative Thrombo-Embolic RiskDocument4 pagesEarly Ambulation and Prevention of Post-Operative Thrombo-Embolic RiskAnderson LondoñoNo ratings yet
- Vte Clinical Update Final - 190207 - 1 - LR FinalDocument6 pagesVte Clinical Update Final - 190207 - 1 - LR FinalSantosh SinghNo ratings yet
- Computed Tomography Findings of Community-Acquired Immunocompetent Patient: A Case ReportDocument4 pagesComputed Tomography Findings of Community-Acquired Immunocompetent Patient: A Case ReportDenta HaritsaNo ratings yet
- Tumor Liquid BiopsiesFrom EverandTumor Liquid BiopsiesFlorence SchaffnerNo ratings yet
- Burkit LymphomaDocument9 pagesBurkit LymphomaEva Paula Badillo SantosNo ratings yet
- Hemoptysis: A Symptom Not Well Explored in The Primary Care Setting in The Developing WorldDocument4 pagesHemoptysis: A Symptom Not Well Explored in The Primary Care Setting in The Developing WorldAditya RamdaniiNo ratings yet
- 移植总论Document88 pages移植总论Mohammed AlwadaiNo ratings yet
- Perikarditis TBDocument8 pagesPerikarditis TBSarah Dyaanggari AkipNo ratings yet
- Spinal Infections: Khoirunnisa Humairoh (702016075)Document31 pagesSpinal Infections: Khoirunnisa Humairoh (702016075)Khoirunnisa HumairohNo ratings yet
- Original Article: Early-And Late-Onset Severe Pneumonia After Renal TransplantationDocument9 pagesOriginal Article: Early-And Late-Onset Severe Pneumonia After Renal TransplantationAndra MariaNo ratings yet
- Challenges in The Diagnosis of Tuberculous MeningitisDocument8 pagesChallenges in The Diagnosis of Tuberculous MeningitisCylla RevataNo ratings yet
- Essentials in Lung TransplantationFrom EverandEssentials in Lung TransplantationAllan R. GlanvilleNo ratings yet
- Clinical Utility of The Band CountDocument36 pagesClinical Utility of The Band CountSergio Alejandro Perez SolisNo ratings yet
- Neu Motor AxDocument6 pagesNeu Motor AxZay SiagNo ratings yet
- Mesenteric Venous Thrombosis As A Complication of Appendicitis in An AdolescentDocument5 pagesMesenteric Venous Thrombosis As A Complication of Appendicitis in An AdolescentEma DianthiNo ratings yet
- Tid 13506Document5 pagesTid 13506Jenny Mundaca QuirozNo ratings yet
- Potential Harm of Prophylactic Platelet Transfusion in Adult Dengue PatientsDocument10 pagesPotential Harm of Prophylactic Platelet Transfusion in Adult Dengue PatientsReynaldo Rahima PutraNo ratings yet
- Postgraduate Course 3 Radiological-Pathological Correlation of Tumoural and Non-Tumoural Pathology: An Interdisciplinary ApproachDocument31 pagesPostgraduate Course 3 Radiological-Pathological Correlation of Tumoural and Non-Tumoural Pathology: An Interdisciplinary ApproachBulborea MihaelaNo ratings yet
- Pulmonary Infiltrates in The Non-HIV-Infected Immunocompromised PatientDocument12 pagesPulmonary Infiltrates in The Non-HIV-Infected Immunocompromised PatientAri KuncoroNo ratings yet
- Kuter DJ - Thrombotic Complications of Central Venous Catheters in Cancer PatientsDocument10 pagesKuter DJ - Thrombotic Complications of Central Venous Catheters in Cancer PatientsFarid RakhmanNo ratings yet
- Trends in Patient Outcome Over The Past Two DecadesDocument12 pagesTrends in Patient Outcome Over The Past Two Decadesfransiskus rendyNo ratings yet
- Improve On-Time DeliveriesDocument24 pagesImprove On-Time DeliveriesUdayNo ratings yet
- Course Registration SlipDocument2 pagesCourse Registration SlipMics EntertainmentNo ratings yet
- Pediatric EmergenciesDocument47 pagesPediatric EmergenciesahmedNo ratings yet
- Passenger Lift Alert - Health and Safety AuthorityDocument4 pagesPassenger Lift Alert - Health and Safety AuthorityReginald MaswanganyiNo ratings yet
- JRC JFE-680 Instruct ManualDocument86 pagesJRC JFE-680 Instruct ManualMark Dominic FedericoNo ratings yet
- Scott 2001Document20 pagesScott 2001Mariana CatiniNo ratings yet
- SSDsDocument3 pagesSSDsDiki Tri IndartaNo ratings yet
- Biology Accel Syllabus 2011-2012Document3 pagesBiology Accel Syllabus 2011-2012Mike DeleonNo ratings yet
- tGr12OM CheResoBookU78910Document110 pagestGr12OM CheResoBookU78910Jamunanantha PranavanNo ratings yet
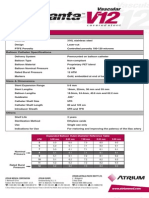
- Advanta V12 Data SheetDocument2 pagesAdvanta V12 Data SheetJuliana MiyagiNo ratings yet
- Flow Chart - QCDocument2 pagesFlow Chart - QCKarthikeyan Shanmugavel100% (1)
- TM-8000 HD Manual PDFDocument37 pagesTM-8000 HD Manual PDFRoxana BirtumNo ratings yet
- Kinematics in One DimensionDocument4 pagesKinematics in One DimensionAldrin VillanuevaNo ratings yet
- Fundamentals of Pain Medicine: Jianguo Cheng Richard W. RosenquistDocument346 pagesFundamentals of Pain Medicine: Jianguo Cheng Richard W. RosenquistMayNo ratings yet
- Digging Deeper: Can Hot Air Provide Sustainable Source of Electricity?Document2 pagesDigging Deeper: Can Hot Air Provide Sustainable Source of Electricity?Рустам ХаджаевNo ratings yet
- Bomba MixerDocument2 pagesBomba MixerBinelli79No ratings yet
- Flight Vehicle Design:: Example 2 (Uav)Document43 pagesFlight Vehicle Design:: Example 2 (Uav)Anmol KumarNo ratings yet
- 12 Key Principles On Bhava AnalysisDocument28 pages12 Key Principles On Bhava AnalysisDhineshNo ratings yet
- Study The Effect of Postharvest Heat Treatment On Infestation Rate of Fruit Date Palm (Phoenix Dactylifera L.) Cultivars Grown in AlgeriaDocument4 pagesStudy The Effect of Postharvest Heat Treatment On Infestation Rate of Fruit Date Palm (Phoenix Dactylifera L.) Cultivars Grown in AlgeriaJournal of Nutritional Science and Healthy DietNo ratings yet
- SAT Practice TestDocument77 pagesSAT Practice TestfhfsfplNo ratings yet
- Manual PipsDocument5 pagesManual PipsOzzyNo ratings yet
- Implicit Explicit SignalsDocument8 pagesImplicit Explicit SignalsVersoza Nel100% (2)
- Main Girders: CrossDocument3 pagesMain Girders: Crossmn4webNo ratings yet
- Learning Activity Sheets Introduction To World Religions and Belief SystemDocument56 pagesLearning Activity Sheets Introduction To World Religions and Belief SystemAngelica Caranzo LatosaNo ratings yet
- Nivel VV-VW Board User Guide enDocument5 pagesNivel VV-VW Board User Guide enHarveyWishtartNo ratings yet
- Fines Reduction Project at Wendling Bowser QuarryDocument2 pagesFines Reduction Project at Wendling Bowser QuarryMarcos Antonio ParoliniNo ratings yet
- Shree New Price List 2016-17Document13 pagesShree New Price List 2016-17ontimeNo ratings yet
- GROSS Mystery of UFOs A PreludeDocument309 pagesGROSS Mystery of UFOs A PreludeTommaso MonteleoneNo ratings yet
- Introduction To LCCDocument32 pagesIntroduction To LCCGonzalo LopezNo ratings yet
- Cargo ManagementDocument45 pagesCargo ManagementShubham Chaurasia75% (8)