You might also like
- (Zafar Iqba) An Islamic Perspect On GovernanceDocument28 pages(Zafar Iqba) An Islamic Perspect On GovernancenazeerahmadNo ratings yet
- Vaginal Delivery of TwinsDocument63 pagesVaginal Delivery of Twinsrake sardevaNo ratings yet
- Recurrent Pregnancy LossDocument61 pagesRecurrent Pregnancy LossHerman FiraNo ratings yet
- Deense Studie PDFDocument12 pagesDeense Studie PDFBas HermansNo ratings yet
- CTG - Kuliah PpdsDocument39 pagesCTG - Kuliah PpdsSyarif Hadi AssegafNo ratings yet
- Preterm Birth PreventionDocument10 pagesPreterm Birth PreventionEdwin Fabian Paz UrbanoNo ratings yet
- A Study of Intrauterine Fetal Death in A Tertiary Care HospitalDocument4 pagesA Study of Intrauterine Fetal Death in A Tertiary Care HospitalintanNo ratings yet
- Tocolysis Review: Clinically Based Insights on Preterm Labor ManagementDocument29 pagesTocolysis Review: Clinically Based Insights on Preterm Labor ManagementAulya Adha DiniNo ratings yet
- Articles: BackgroundDocument13 pagesArticles: BackgroundHartanto LieNo ratings yet
- PIIS2210778916303701Document2 pagesPIIS2210778916303701Fatimah AssagafNo ratings yet
- Practice Bulletin No 144 Multifetal Gestations .40Document15 pagesPractice Bulletin No 144 Multifetal Gestations .40Jose Luis Morales Bautista100% (1)
- PrematuritylabordeliveryDocument32 pagesPrematuritylabordeliverySachin GeorgeNo ratings yet
- The Management of Preterm Labor: Robert L. GoldenbergDocument18 pagesThe Management of Preterm Labor: Robert L. GoldenbergMarjorie Eliana MorejónNo ratings yet
- Intrapartum Fetal Monitoring PDFDocument4 pagesIntrapartum Fetal Monitoring PDFelda zulkarnainNo ratings yet
- Recurrent Pregnancy LossDocument71 pagesRecurrent Pregnancy LossshashankiswaitingNo ratings yet
- ESHRE Meeting AbstractsDocument1 pageESHRE Meeting AbstractsAby SuryaNo ratings yet
- Acog Practice Bulletin Summary: Multifetal Gestations: Twin, Triplet, and Higher-Order Multifetal PregnanciesDocument4 pagesAcog Practice Bulletin Summary: Multifetal Gestations: Twin, Triplet, and Higher-Order Multifetal PregnanciesMariana Hernandez100% (3)
- Dr. Sharda Jain: Director: Secretary GeneralDocument91 pagesDr. Sharda Jain: Director: Secretary GeneraljijaniNo ratings yet
- 11 Update Use of Progestogen in Miscarriage ManagementDocument35 pages11 Update Use of Progestogen in Miscarriage Managementasshagab04No ratings yet
- New Insights Into Mechanisms Behind Miscarriage: Review Open AccessDocument10 pagesNew Insights Into Mechanisms Behind Miscarriage: Review Open AccessindriannanhNo ratings yet
- Recurrent Pregnancy Loss Consesutive Vs Non ConsecutiveDocument7 pagesRecurrent Pregnancy Loss Consesutive Vs Non ConsecutiveAsociatia Embriologilor AerNo ratings yet
- Karakteristik Dan Luaran Preeklampsi Di Rsup Prof. Dr. R.D. Kandou ManadoDocument5 pagesKarakteristik Dan Luaran Preeklampsi Di Rsup Prof. Dr. R.D. Kandou ManadoMegHa Pisc'girLzNo ratings yet
- AHD Dec 15 10 - Women's Issues in Neurology - YuDocument55 pagesAHD Dec 15 10 - Women's Issues in Neurology - YuoliveroslovelynNo ratings yet
- ACOG SMFM Joint Practice Bulletin Multiple Gestation 2004Document15 pagesACOG SMFM Joint Practice Bulletin Multiple Gestation 2004Reza ZulkarnainNo ratings yet
- 10 1111@jog 13886Document5 pages10 1111@jog 13886Septian WidiantoNo ratings yet
- The NeoUpdates - DecDocument7 pagesThe NeoUpdates - DecDr Satish MishraNo ratings yet
- Arabin Pessary to Prevent Adverse Perinatal Outcomes in Twin Pregnancies With a Short Cervix, PESSARONE. Marion GroussollesDocument13 pagesArabin Pessary to Prevent Adverse Perinatal Outcomes in Twin Pregnancies With a Short Cervix, PESSARONE. Marion GroussollesqmfddnhdjmNo ratings yet
- Adekanle Et AlDocument5 pagesAdekanle Et AlI_Ketut_Wahyu_MerthaNo ratings yet
- Multifetal PregnancyDocument33 pagesMultifetal PregnancyGina Magda RianaNo ratings yet
- Antenatal Corticosteroids For Accelerating Fetal Lung Maturation For Women at Risk of Preterm Birth - McGoldrick, E - 2020 Cochrane LibraryDocument88 pagesAntenatal Corticosteroids For Accelerating Fetal Lung Maturation For Women at Risk of Preterm Birth - McGoldrick, E - 2020 Cochrane Libraryjavier dauvergneNo ratings yet
- Prevention of Spontaneous Preterm Birth: Universal Cervical Length Assessment and Vaginal Progesterone in Women With A Short Cervix: Time For Action!Document8 pagesPrevention of Spontaneous Preterm Birth: Universal Cervical Length Assessment and Vaginal Progesterone in Women With A Short Cervix: Time For Action!Carmen BarbozaNo ratings yet
- Maternal and Fetal Outcomes in Grand Multiparous WomenDocument2 pagesMaternal and Fetal Outcomes in Grand Multiparous WomenYoser ThamtonoNo ratings yet
- Multifetal Pregnancy: Early Diagnosis and ManagementDocument33 pagesMultifetal Pregnancy: Early Diagnosis and ManagementjasmniaNo ratings yet
- Gestational Diabetes Mellitus in Teenage Pregnancy: A Case-Control StudyDocument3 pagesGestational Diabetes Mellitus in Teenage Pregnancy: A Case-Control StudySarly FebrianaNo ratings yet
- Stillbirth C1 PPT - LectureDocument35 pagesStillbirth C1 PPT - LectureHenok Y KebedeNo ratings yet
- External Cephalic VersionDocument15 pagesExternal Cephalic VersionDiegoNo ratings yet
- Preterm Labor: Dr.H.M.Hatta Ansyori Spog (K) Sriwijaya University Faculty of MedicineDocument43 pagesPreterm Labor: Dr.H.M.Hatta Ansyori Spog (K) Sriwijaya University Faculty of MedicineiqiqiqiqiqNo ratings yet
- Pre and Post Conception Risk Factors in PROM: Research ArticleDocument5 pagesPre and Post Conception Risk Factors in PROM: Research ArticleNurul ImaniarNo ratings yet
- Prolonged Latency of Preterm Premature Rupture of Membranes and Risk of Neonatal SepsisDocument6 pagesProlonged Latency of Preterm Premature Rupture of Membranes and Risk of Neonatal SepsisYudhi AuliaNo ratings yet
- Malignancies in Pregnancy Multiple 2016 Best Practice Research ClinicalDocument8 pagesMalignancies in Pregnancy Multiple 2016 Best Practice Research ClinicalorriNo ratings yet
- Nejme2032499 PDFDocument2 pagesNejme2032499 PDFBladimir CentenoNo ratings yet
- Screening For Fetal Growth Restriction Using Ultrasound and The Sflt1/Plgf Ratio in Nulliparous Women: A Prospective Cohort StudyDocument13 pagesScreening For Fetal Growth Restriction Using Ultrasound and The Sflt1/Plgf Ratio in Nulliparous Women: A Prospective Cohort StudynicolasdlcaNo ratings yet
- Preterm Labor - AAFPDocument21 pagesPreterm Labor - AAFPfirdaus zaidiNo ratings yet
- W 3 RT 2 QwfcavfgsbszDocument6 pagesW 3 RT 2 QwfcavfgsbszkennydimitraNo ratings yet
- 10 Bellcross Genetics NIPS CLIAC Nov2015Document30 pages10 Bellcross Genetics NIPS CLIAC Nov2015felicia susantoNo ratings yet
- Embarazo MultipleDocument15 pagesEmbarazo MultipleLina E. ArangoNo ratings yet
- Is Fetal Growth Restriction Associated With A More Severe Maternal Phenotype in The Setting of Early Onset Pre-Eclampsia? A Retrospective StudyDocument6 pagesIs Fetal Growth Restriction Associated With A More Severe Maternal Phenotype in The Setting of Early Onset Pre-Eclampsia? A Retrospective StudyYessie ErNo ratings yet
- Original ArticleDocument4 pagesOriginal ArticlefeyzarezarNo ratings yet
- Cerclage For Women With Twin Pregnancies: A Systematic Review and MetaanalysisDocument16 pagesCerclage For Women With Twin Pregnancies: A Systematic Review and MetaanalysisSaira MendozaNo ratings yet
- Gestational Diabetes Mellitus Is Associated With Adverse Outcomes in Twin PregnanciesDocument8 pagesGestational Diabetes Mellitus Is Associated With Adverse Outcomes in Twin PregnanciesDwi OktaviliaNo ratings yet
- Spontaneous Preterm Birth Prevention in Multiple PregnancyDocument7 pagesSpontaneous Preterm Birth Prevention in Multiple PregnancyElias Melo JrNo ratings yet
- Best Practice in Abortion CareDocument27 pagesBest Practice in Abortion CareQaisar iqbalNo ratings yet
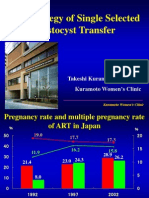
- The Strategy of Single Selected Blastocyst Transfer: Takeshi Kuramoto MD, PHD Kuramoto Women'S ClinicDocument43 pagesThe Strategy of Single Selected Blastocyst Transfer: Takeshi Kuramoto MD, PHD Kuramoto Women'S ClinicDian Isti AngrainiNo ratings yet
- Ultrasound in Obstet Gyne - 2019 - Litwinska - Outcome of Twin Pregnancy With Two Live Fetuses at 11 13 Weeks GestationDocument8 pagesUltrasound in Obstet Gyne - 2019 - Litwinska - Outcome of Twin Pregnancy With Two Live Fetuses at 11 13 Weeks GestationIsi Brito AstudilloNo ratings yet
- Hum. Reprod.-2004-Carp-191-5Document5 pagesHum. Reprod.-2004-Carp-191-5venkayammaNo ratings yet
- What's New in The Other Journals?: Screening For Ovarian Cancer Bilateral Salpingo-Oophorectomy at Hysterectomy or Not?Document2 pagesWhat's New in The Other Journals?: Screening For Ovarian Cancer Bilateral Salpingo-Oophorectomy at Hysterectomy or Not?Gladstone AsadNo ratings yet
- Lecture IV IIIDocument32 pagesLecture IV IIIMohamad Alsayed AlasaasNo ratings yet
- Intrauterine Growth Restriction IUGRDocument8 pagesIntrauterine Growth Restriction IUGRJyoti Prem UttamNo ratings yet
- Pregnancy Tests Explained (2Nd Edition): Current Trends of Antenatal TestsFrom EverandPregnancy Tests Explained (2Nd Edition): Current Trends of Antenatal TestsNo ratings yet
- Vol9 Issue1 06Document4 pagesVol9 Issue1 06annisaNo ratings yet
- Vocal Cord Paralysis and Its Etiologies A Prospective StudyDocument4 pagesVocal Cord Paralysis and Its Etiologies A Prospective StudySheilla KhonadaNo ratings yet
- You Are Not A Victim of CircumstancesDocument1 pageYou Are Not A Victim of CircumstancesSheilla KhonadaNo ratings yet
- Catalase Evaluation in Different Human Diseases Associated With Oxidative StressDocument5 pagesCatalase Evaluation in Different Human Diseases Associated With Oxidative StressSheilla KhonadaNo ratings yet
- The Safety of Ingested CaffeineDocument19 pagesThe Safety of Ingested CaffeineSheilla KhonadaNo ratings yet
- Daily lesson plans for MAPEH at SJPNHS-La PurisimaDocument10 pagesDaily lesson plans for MAPEH at SJPNHS-La PurisimaCharlene BorladoNo ratings yet
- Concept of unitive and procreative healthDocument5 pagesConcept of unitive and procreative healthDONITA DALUMPINESNo ratings yet
- Miscarriage What Is It?Document4 pagesMiscarriage What Is It?Suseno AjiNo ratings yet
- Comprehensive Sex Ed May Reduce Teen PregnancyDocument2 pagesComprehensive Sex Ed May Reduce Teen PregnancyHanz FetiloNo ratings yet
- Breastfeeding: Proper Positioning and Latch-On SkillsDocument4 pagesBreastfeeding: Proper Positioning and Latch-On SkillsEdmr SlzarNo ratings yet
- DLP CeliaCabacangDocument7 pagesDLP CeliaCabacangAthena Althea100% (1)
- Polycystic Ovary Syndrome (PCOS) : February 2020Document5 pagesPolycystic Ovary Syndrome (PCOS) : February 2020Lia MeivianeNo ratings yet
- Management of Obstetric Emergencies Y5Document80 pagesManagement of Obstetric Emergencies Y5Charles Wilson83% (6)
- IDEA Endometrioza ISUOGDocument16 pagesIDEA Endometrioza ISUOGAlexandra CristoforNo ratings yet
- The 5 Types of Female OrgasmsDocument16 pagesThe 5 Types of Female OrgasmsKriketNo ratings yet
- Screening and Diagnosis of High-Risk PregnancyDocument44 pagesScreening and Diagnosis of High-Risk PregnancyKavipriyaNo ratings yet
- Antenatal Corticosteroid Therapy For Fetal Maturation - ACOGDocument21 pagesAntenatal Corticosteroid Therapy For Fetal Maturation - ACOGherryNo ratings yet
- Management of LabourDocument38 pagesManagement of LabourAnjali Rahul AjmeriNo ratings yet
- Squirt! The Female Ejaculation Black BookDocument35 pagesSquirt! The Female Ejaculation Black BookAARON AYIKU50% (2)
- The Sex Industry in Western AustraliaDocument55 pagesThe Sex Industry in Western Australiaantonia_bordoniNo ratings yet
- 2019 IVF Fee Schedule and ContactsDocument9 pages2019 IVF Fee Schedule and ContactsamirNo ratings yet
- Velma Cosplay Camshow, Free XNNX Porn Video 5f Xhamster Xhamster 2 PDFDocument1 pageVelma Cosplay Camshow, Free XNNX Porn Video 5f Xhamster Xhamster 2 PDFTemitope GruhnNo ratings yet
- Assessment of Fetal Growth and DevelopmentDocument12 pagesAssessment of Fetal Growth and Developmentaracelisurat100% (1)
- Family Planning Flip ChartDocument44 pagesFamily Planning Flip ChartWarrenNo ratings yet
- NCP Shoulder DystociaDocument4 pagesNCP Shoulder DystociaTrishia CaroNo ratings yet
- Genogram Symbols & GuideDocument1 pageGenogram Symbols & Guidesigmanu22No ratings yet
- 50 Shades Bared Scrutinizing Contemporary Erotic Literature Through The Eyes of Moral Philosophy and ReligionDocument23 pages50 Shades Bared Scrutinizing Contemporary Erotic Literature Through The Eyes of Moral Philosophy and ReligionLenie Rose Clarete VeronillaNo ratings yet
- Pelatihan Massage Akupressur untuk BidanDocument9 pagesPelatihan Massage Akupressur untuk BidanViviNo ratings yet
- Premature Birth GuideDocument11 pagesPremature Birth GuidetasaNo ratings yet
- DynaMed Plus - Premature Rupture of Membranes at Term (Term PROM)Document16 pagesDynaMed Plus - Premature Rupture of Membranes at Term (Term PROM)LudwinNo ratings yet
- Child Rearing TypesDocument11 pagesChild Rearing TypesAnjali SainiNo ratings yet
- Manfaat Rendaman Air Hangat Dan Garam Dalam Menurunkan Derajat Edema Kaki Ibu Hamil Trimester IiiDocument6 pagesManfaat Rendaman Air Hangat Dan Garam Dalam Menurunkan Derajat Edema Kaki Ibu Hamil Trimester IiiShinta BalikpapanNo ratings yet
- Rhesus FactorDocument2 pagesRhesus Factorinspirohm777No ratings yet
- Reference Manual For Male Sterilization-NSV-Oct 2013Document132 pagesReference Manual For Male Sterilization-NSV-Oct 2013Anagha M NairNo ratings yet
- Mapeh Worksheet - Wk5-Q2 Health 8: Unit 2: Family Life Pregnancy-Related Concerns and Pre-Natal CareDocument7 pagesMapeh Worksheet - Wk5-Q2 Health 8: Unit 2: Family Life Pregnancy-Related Concerns and Pre-Natal CareNathan MasilunganNo ratings yet