CM MED/U/39
L ABORATORIUM
BADAN LAYANAN UMUM DAERAH
PUSKESMAS KECAMATAN KEBON JERUK
Jl. Raya Kebon Jeruk No. 2, Jakarta Barat. Nomor Telp: 5309838, 5482367, Fax: 5482367
NO. URUT LAB : ............................................................ NO. REGISTER LAB : .............................................................
NAMA PASIEN : ................................................... L / P TANGGAL : .............................................................
UMUR : ................................................ Tahun DOKTER : .............................................................
ALAMAT : ............................................................ UNIT : .............................................................
DIAGNOSA : ............................................................
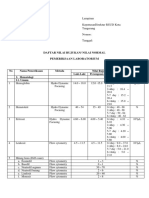
1. HEMATOLOGI 4. URINE
□ Darah Lengkap Nilai Normal □ Urine Lengkap Nilai Normal
Kimia Urine
□ Hb : ............... gr/dl 11 – 16,5 gr Warna : .................... Kuning
□ Leukosit : ............... / mm3 darah 4..000 – 10.000
Kejernihan
Urobilinogen
: ....................
: ....................
Jernih
(+)
□ Eritrosit : ............... Juta / mm3 3,8 – 5,8
□ Glukosa : .................... (–)
□ DifferensiaL : Keton : .................... (–)
Basofil : ............... % 0 – 1 Bilirubin : .................... (–)
Eosinofil : ............... % 1 – 3
N. Batang
N. Segmen
: ............... %
: ............... %
2
50
–
–
6
70
□ Protein : .................... (–)
Nitrit : .................... (–)
Limfosit : ............... % 20 – 40
Monosit : ............... % 2 – 8 PH : .................... ( 4.8 – 7.3 )
Occult Blood : .................... (–)
□ Trombosit : ............... x 109/L 100 – 300 Specific Gravity : .................... ( 1.003 – 1.030 )
□ Hematokrit : ............... % 30 – 50
Leukosit : .................... (–)
Mikroskopis Urine /Sedimen
□ MCV : ............... fl 80 – 99 Leukosit : .................... (0–3)
□ MCH : ............... pg 26,5 – 33,5
Eritrosit
Epithel
: ....................
: ....................
(0–1)
(+/– )
□ MCHC : ............... gr/dl 32 – 36 Asam urat : .................... (–)
□ LED : ............... mm / jam P : 0 – 10
Kristal ca. Oksalat : ....................
Triple fosfat : ....................
(–)
(–)
W : 0 – 20
Amorf : .................... (–)
□ Golongan Darah : ............... RH ............ Silinder : .................... (–)
□ Masa Pendarahan / BT : ..........’ ..........” 1’00” – 3’00”
Bakteri : .................... (–)
□ Masa Pembekuan / CT : ...........’ ..........” 3’00” – 6’00”
□ Test Kehamilan : .................... (+/–)
5. FEACES
2. KIMIA DARAH
□ GULA DARAH
□ Feaces Rutin
Warna : .................... Kuning / Coklat
□ Gula Darah Sewaktu : ........... mg/dl P/W : < 180 mg/dl
Bau : .................... Khas
□ Gula Darah Puasa* : ........... mg/dl P/W : < 110 mg/dl Konsistensi : .................... Lunak
□ Gula Darah 2 Jam PP** : ........... mg/dl P/W : < 140 mg/dl Lendir : .................... (–)
□ LEMAK
Eritrosit : .................... (–)
Telur Cacing : .................... (–)
□ Kolesterol Total* : ........... mg/dl P/W : < 200 mg/dl
□ Trigliserida* : ........... mg/dl P/W : < 150 mg/dl 6. BAKTERIOLOGI
□ HDL Kolesterol : ........... mg/dl P : 30-60 mg/dl □ SPUTUM BTA
W : 40-70 mg/dl
□ Pagi : .................... (–)
□ LDL Kolesterol : ........... mg/dl P/W : < 150 mg/dl
□ Sewaktu : .................... (–)
□ FAAL HATI
□ Gene-Xpert : .................... (–)
□ SGOT : ........... u/l P/W : < 40 u/l
□ Kerokan Kulit / MH : .................... (–)
□ SGPT : ........... u/l P/W : < 41 u/l
□ Bilirubin Total : ........... mg/dl P/W : < 1,1 mg/dl
Bayi : < 12 mg/dl INFORMED CONSENT
□ Bilirubin Direk : ........... mg/dl P/W : < 0,25 mg/dl Saya yang bertanda tangan dibawah ini menyatakan, bahwa
□ Bilirubin Indirek : .......... mg/dl P/W : 0,1-0,8mg/dl
saya SETUJU* / MENOLAK* dilakukan pengambilan sample
untuk pemeriksaan laboratorium.
□ FAAL GINJAL
SETUJU MENOLAK
□ Uric acid : .......... mg/dl P : 3,5 – 7,2 mg/dl
W : 2,6 – 6,0 mg/dl
□ Ureum : .......... mg/dl P/W : 10–50 mg/dl
□ Creatinin : .......... mg/dl P/W: 0,6–1,4mg/dl
NO. TELP PASIEN
3. IMUNOSEROLOGI
□ WIDAL □ HbsAg : ................ ( - )
Ag – O : ............... ( - )
AO : ............... ( - ) □ Anti HbsAg : ................ ( - )
BO : ............... ( - ) PETUGAS PEMERIKSA
CO : ............... ( - ) □ RAPID TEST
Ag – H : ............... ( - ) □ HIV : ................ ( - )
AH : ............... ( - ) □ Syphilis : .................. ( - )
BH : ............... ( - )
CH : ............... ( - )
Keterangan :
* Pemeriksaan dilakukan setelah “PUASA” selama 10 – 12 jam *Silahkan coret salah satu pada kata SETUJU / MENOLAK
**Pemeriksaan dilakukan setelah “PUASA” 2 jam, setelah makan
� L ABORATORIUM
BADAN LAYANAN UMUM DAERAH
PUSKESMAS KECAMATAN KEBON JERUK
Jl. Raya Kebon Jeruk No. 2, Jakarta Barat. Nomor Telp: 5309838, 5482367, Fax: 5482367