You might also like
- How To Perform The Best Intrauterine Insemination A Review 2167 0250 1000140Document7 pagesHow To Perform The Best Intrauterine Insemination A Review 2167 0250 1000140Anand NNo ratings yet
- Heavy Menstrual BleedingDocument29 pagesHeavy Menstrual BleedingsanjupainNo ratings yet
- Erpm InfoDocument16 pagesErpm InfoPamudri Basnayake100% (1)
- AUBDocument45 pagesAUBJBNo ratings yet
- Infertility IDocument36 pagesInfertility Idr_asaleh100% (1)
- AUB StartedDocument13 pagesAUB StartedIbrahim AbdullahNo ratings yet
- InfertilityDocument14 pagesInfertilityDrChauhanNo ratings yet
- Uterine FibroidsDocument21 pagesUterine FibroidsPrasun BiswasNo ratings yet
- Dr. Sharda Jain: Director: Secretary GeneralDocument91 pagesDr. Sharda Jain: Director: Secretary GeneraljijaniNo ratings yet
- Secondary Amenorrhea: DR Hanaa AlaniDocument44 pagesSecondary Amenorrhea: DR Hanaa AlaniAakashNo ratings yet
- Benign and Malignant Tumors of Female Genital TractDocument14 pagesBenign and Malignant Tumors of Female Genital TractDimitrios PapadopoulosNo ratings yet
- Male InfertilityDocument57 pagesMale InfertilityUsha AnengaNo ratings yet
- Colposcopy Principles and Practice PDFDocument2 pagesColposcopy Principles and Practice PDFAnne0% (2)
- Pulmonary Disorders in PregnancyDocument49 pagesPulmonary Disorders in PregnancyMara Medina - BorleoNo ratings yet
- Hormonal ContraceptivesDocument25 pagesHormonal Contraceptivesmd easarur rahmanNo ratings yet
- Cervical Intraepithelial Neoplasia and Cervical CancerDocument28 pagesCervical Intraepithelial Neoplasia and Cervical CancerNatnael100% (1)
- Bacterial VaginosisDocument4 pagesBacterial VaginosisjoycesiosonNo ratings yet
- Diabetes RoadmapDocument8 pagesDiabetes Roadmapwuryan dewiNo ratings yet
- Mal Presentations Mal PositionsDocument4 pagesMal Presentations Mal PositionsMelissa Aina Mohd YusofNo ratings yet
- (Gyne) 2.06 Aub - Dr. Quillamor (Final)Document8 pages(Gyne) 2.06 Aub - Dr. Quillamor (Final)Rj PolvorosaNo ratings yet
- Recurrent Pregnancy LossDocument61 pagesRecurrent Pregnancy LossHerman FiraNo ratings yet
- Differential Diagnosis of The Adnexal Mass 2020Document38 pagesDifferential Diagnosis of The Adnexal Mass 2020Sonia MVNo ratings yet
- C SectionDocument50 pagesC SectionAlano S. LimgasNo ratings yet
- Preterm Prelabour Rupture of MembranesDocument12 pagesPreterm Prelabour Rupture of MembranesSeptiany Indahsari DjanNo ratings yet
- Annotated Bibliography of Advance Nursing PracticeDocument4 pagesAnnotated Bibliography of Advance Nursing PracticeKaku ManishaNo ratings yet
- Submitted By: Diana M. Resultay A301/Group-3B Submitted To: Ms. ReyesDocument9 pagesSubmitted By: Diana M. Resultay A301/Group-3B Submitted To: Ms. ReyesDiannetotz MoralesNo ratings yet
- Gynecological and Obstetrics InstrumentsDocument61 pagesGynecological and Obstetrics InstrumentsRaja33% (3)
- Hiv in PregnancyDocument98 pagesHiv in PregnancyAkrit DahalNo ratings yet
- Protocol Book For OBGYNDocument41 pagesProtocol Book For OBGYNShabir BadakhshNo ratings yet
- Abnormal Uterine BleedingDocument44 pagesAbnormal Uterine BleedingBezza Mae Roche CruzNo ratings yet
- Essentials for Practice of Medicine in the Frontline: From Tropical Africa; Pleasantly Different Volume 2From EverandEssentials for Practice of Medicine in the Frontline: From Tropical Africa; Pleasantly Different Volume 2No ratings yet
- Ob-Gyn (Clinic/Office) Nurse: OB/GYN Nurses Provide A Variety of Functions Related To The Female Reproductive SystemDocument13 pagesOb-Gyn (Clinic/Office) Nurse: OB/GYN Nurses Provide A Variety of Functions Related To The Female Reproductive SystemJaclyn SarmientoNo ratings yet
- AUBDocument26 pagesAUByayaslaras96No ratings yet
- Deep Vein Thrombosis and Pulmonary Embolism in Pregnancy - Prevention - UpToDateDocument11 pagesDeep Vein Thrombosis and Pulmonary Embolism in Pregnancy - Prevention - UpToDateGabyta007No ratings yet
- Impey Obs and Gynae Revision Notes PDFDocument9 pagesImpey Obs and Gynae Revision Notes PDFRoiseNo ratings yet
- OB Hematologic DiseasesDocument2 pagesOB Hematologic DiseasespreciousjemNo ratings yet
- Biomarkers in Abnormal Uterine Bleeding: Precision Medicine in Assisted Reproductive Technologies Special IssueDocument12 pagesBiomarkers in Abnormal Uterine Bleeding: Precision Medicine in Assisted Reproductive Technologies Special IssueWahyuning PutriNo ratings yet
- O&G Counselling - TSPDocument6 pagesO&G Counselling - TSPTarran PhagooNo ratings yet
- Uterus NeoDocument11 pagesUterus NeoHester Marie SimpiaNo ratings yet
- PulseDocument43 pagesPulseAngelo LacisteNo ratings yet
- Gynecological History Taking and ExaminationDocument17 pagesGynecological History Taking and Examinationnmsiswaridewi100% (1)
- Obs History Taking FormatDocument24 pagesObs History Taking FormatBibek PandeyNo ratings yet
- Hepatitis B in PregnancyDocument17 pagesHepatitis B in PregnancysnazzyNo ratings yet
- Green Top Guidelines 13Document29 pagesGreen Top Guidelines 13garfield1No ratings yet
- MenorrhagiaDocument4 pagesMenorrhagiaFlloyd_Martin__1259No ratings yet
- Obstetric Gynaecology Jan 11Document32 pagesObstetric Gynaecology Jan 11selvie87No ratings yet
- Uterine FibroidsDocument47 pagesUterine FibroidsMoh Aldhy HusaintNo ratings yet
- Approach To Patient With Ovarian Cysts: Done By: Yahyia Al-Abri 90440Document53 pagesApproach To Patient With Ovarian Cysts: Done By: Yahyia Al-Abri 90440NinaNo ratings yet
- Nausea and Vomiting of Pregnancy and Hyperemesis GravidarumDocument27 pagesNausea and Vomiting of Pregnancy and Hyperemesis GravidarumxxdrivexxNo ratings yet
- Guidelines For Management of Endometrial CarcinomaDocument41 pagesGuidelines For Management of Endometrial CarcinomaVeenaNo ratings yet
- Gestational Trophoblastic Disease Pt2Document75 pagesGestational Trophoblastic Disease Pt2yurie_ameliaNo ratings yet
- Obstetric Summm 1Document46 pagesObstetric Summm 1ملك عيسىNo ratings yet
- Repair of Obstetric Perineal LacerationsDocument7 pagesRepair of Obstetric Perineal LacerationsadriantiariNo ratings yet
- FIGO Guidelines - Prevention and Treatment of PPH Etc1Document12 pagesFIGO Guidelines - Prevention and Treatment of PPH Etc1karinasurakusumaNo ratings yet
- Syndromic Management of Sexually Transmitted InfectionsDocument76 pagesSyndromic Management of Sexually Transmitted Infectionsnamita100% (2)
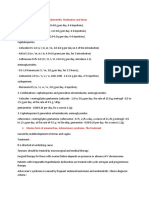
- Treatment of Acute Endometritis. Medication and DosesDocument3 pagesTreatment of Acute Endometritis. Medication and DosesTitoun LettounNo ratings yet
- Acute GlomerulonephritisDocument28 pagesAcute GlomerulonephritisPaul SinsNo ratings yet
- 8surgical Management of Dysfunctional Uterine Bleeding - KabilanDocument14 pages8surgical Management of Dysfunctional Uterine Bleeding - KabilanNavani TharanNo ratings yet
- Genital FistulaeDocument15 pagesGenital Fistulaesangeetha francisNo ratings yet
- Obstetrics History Taking in and Examination PowerpointDocument15 pagesObstetrics History Taking in and Examination Powerpointياسر كوثر هانيNo ratings yet
- Revision Long Case Obs GynaeDocument10 pagesRevision Long Case Obs GynaeHo Yong WaiNo ratings yet
- HysterectomyDocument70 pagesHysterectomyYudhistira AdiNo ratings yet
- Acog Committee Opinion: Medically Indicated Late-Preterm and Early-Term DeliveriesDocument5 pagesAcog Committee Opinion: Medically Indicated Late-Preterm and Early-Term DeliveriesBianca CaterinalisendraNo ratings yet
- Puerpera L Mental DisordersDocument13 pagesPuerpera L Mental DisordersclarheenaNo ratings yet
- Manajemen Pelayanan Primer: (Primary Health Care)Document34 pagesManajemen Pelayanan Primer: (Primary Health Care)wuryan dewiNo ratings yet
- Psikiatri BiologikDocument39 pagesPsikiatri Biologikwuryan dewiNo ratings yet
- 10a Dermatitis AtopikDocument27 pages10a Dermatitis Atopikwuryan dewiNo ratings yet
- Kuliah Pengantar Blok KulitDocument27 pagesKuliah Pengantar Blok Kulitwuryan dewiNo ratings yet
- A New Understanding of The Coagulation ProcessDocument6 pagesA New Understanding of The Coagulation Processwuryan dewiNo ratings yet
- Kuliah Blok Hemaologi-ERITROSITDocument30 pagesKuliah Blok Hemaologi-ERITROSITwuryan dewiNo ratings yet
- 002 Kuliah Nutrisi Untuk HematopoiesisDocument120 pages002 Kuliah Nutrisi Untuk Hematopoiesiswuryan dewiNo ratings yet
- Jaypee Ebook Titles Upto 2016 PDFDocument38 pagesJaypee Ebook Titles Upto 2016 PDFShraadha JaiswaniNo ratings yet
- Colposcopy - UpToDateDocument25 pagesColposcopy - UpToDatemew2xxNo ratings yet
- Uts 4Document16 pagesUts 4raine zapantaNo ratings yet
- Art Bio ProjectDocument13 pagesArt Bio ProjectKriti Sharma75% (8)
- Asherman Jurnal 1Document8 pagesAsherman Jurnal 1Rahma MahrozaNo ratings yet
- Proliferative EndometriumDocument4 pagesProliferative EndometriumKristine Dela CruzNo ratings yet
- CUC Breast Cancer History and Examination DR Corinne Jones Mar10Document1 pageCUC Breast Cancer History and Examination DR Corinne Jones Mar10starblue265No ratings yet
- Pelvic Inflammatory DiseaseDocument15 pagesPelvic Inflammatory DiseaseJay PaulNo ratings yet
- Esgd 3Document279 pagesEsgd 3JOSHUA MEDRANONo ratings yet
- DR Suman Lal Best Gynecologist Obstetrician Doctor in GurgaonDocument3 pagesDR Suman Lal Best Gynecologist Obstetrician Doctor in GurgaondrsumanlalNo ratings yet
- AMC OBS & GYNAC 2005 To 2009Document22 pagesAMC OBS & GYNAC 2005 To 2009Vidarshi Supushpa KithminiNo ratings yet
- Yellow Vaginal Discharge During PregnancyDocument3 pagesYellow Vaginal Discharge During PregnancyDavid Eka PrasetyaNo ratings yet
- Sex EduDocument3 pagesSex EduVarEedt Kodox'sNo ratings yet
- Case WriteupDocument5 pagesCase WriteupBatool AldaherNo ratings yet
- Test Bank For Davis Advantage For Maternal-Child Nursing CareDocument16 pagesTest Bank For Davis Advantage For Maternal-Child Nursing CarekapedispursNo ratings yet
- Dr. Sourav Chowdhury Senior ResidentDocument79 pagesDr. Sourav Chowdhury Senior ResidentBhawna JoshiNo ratings yet
- KULIAH 4 - Siklus MenstruasiDocument15 pagesKULIAH 4 - Siklus MenstruasigahanNo ratings yet
- Ramakrishna College VisitDocument18 pagesRamakrishna College Visitrmconvidhya sri2015No ratings yet
- Name: - Date: - Grade/Section: - Score: - Subject: ENGLISH 5 Quarter 2 - Worksheet No.1Document13 pagesName: - Date: - Grade/Section: - Score: - Subject: ENGLISH 5 Quarter 2 - Worksheet No.1Roc ValdezNo ratings yet
- 2011 - Unsafe Abortion and Postabortion Care - An OverviewDocument9 pages2011 - Unsafe Abortion and Postabortion Care - An OverviewJeremiah WestNo ratings yet
- Abstinence and Birth Control Analysis Chart: Sample: Sterilization SurgeryDocument3 pagesAbstinence and Birth Control Analysis Chart: Sample: Sterilization SurgeryGabriel GalvezNo ratings yet
- SARMS Powders Prices - David FromDocument1 pageSARMS Powders Prices - David FromOld World OrderNo ratings yet
- Synthetic Preparation of HormonesDocument23 pagesSynthetic Preparation of HormonesSadia YousafNo ratings yet
- Endometrial CancerDocument23 pagesEndometrial CancerAlmina RehmanNo ratings yet
- Actinomyces Israelii in The Review: Female GenitalDocument6 pagesActinomyces Israelii in The Review: Female GenitalfranciscaNo ratings yet