You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- PEBC Evaluating Exam Mustpass - Misbah - 2016Document437 pagesPEBC Evaluating Exam Mustpass - Misbah - 2016Dan89% (36)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Lehnes Pharmacology For Nursing Care 10th Edition Burchum Test BankDocument35 pagesLehnes Pharmacology For Nursing Care 10th Edition Burchum Test Bankmanganicidealityfy9rc1100% (19)
- Pedia QuizesDocument19 pagesPedia QuizesPraneeth PaletiNo ratings yet
- Jadwal Jaga Kepaniteraan Anak Fakultas Kedokteran Universitas Yarsi Di Rs TK Ii Moh Ridwan Meuraksa Periode 13 Mei - 27 Juli 2019Document5 pagesJadwal Jaga Kepaniteraan Anak Fakultas Kedokteran Universitas Yarsi Di Rs TK Ii Moh Ridwan Meuraksa Periode 13 Mei - 27 Juli 2019Dea Melinda SabilaNo ratings yet
- A Multicenter, Randomized, Open-Label, Active-Comparator Trial To Determine The Efficacy, .Document16 pagesA Multicenter, Randomized, Open-Label, Active-Comparator Trial To Determine The Efficacy, .Dea Melinda SabilaNo ratings yet
- A Multicenter, Randomized, Open-Label, Active-Comparator Trial To Determine The Efficacy, .Document16 pagesA Multicenter, Randomized, Open-Label, Active-Comparator Trial To Determine The Efficacy, .Dea Melinda SabilaNo ratings yet
- NIH Public Access: Interventions For Acute Internal HordeolumDocument20 pagesNIH Public Access: Interventions For Acute Internal HordeolumhilmanNo ratings yet
- Jurnal ANAKDocument11 pagesJurnal ANAKAndrew NdewNo ratings yet
- Blanko Ujian Status Pasien Klinik Penyakit DalamDocument16 pagesBlanko Ujian Status Pasien Klinik Penyakit DalamDea Melinda SabilaNo ratings yet
- The Antipyretic Efficacy and Safety of Propacetamol Compared With Dexibuprofen PDFDocument7 pagesThe Antipyretic Efficacy and Safety of Propacetamol Compared With Dexibuprofen PDFDea Melinda SabilaNo ratings yet
- A Multicenter, Randomized, Open-Label, Active-Comparator Trial To Determine The Efficacy, .Document16 pagesA Multicenter, Randomized, Open-Label, Active-Comparator Trial To Determine The Efficacy, .Dea Melinda SabilaNo ratings yet
- Presentasi Kasus Ppok: Oleh: Annisa Robiyanti 1102011038 Dea Melinda Sabila 1102013072 Pembimbing: DR - Endah A. SP.PDocument3 pagesPresentasi Kasus Ppok: Oleh: Annisa Robiyanti 1102011038 Dea Melinda Sabila 1102013072 Pembimbing: DR - Endah A. SP.PDea Melinda SabilaNo ratings yet
- NIH Public Access: Interventions For Acute Internal HordeolumDocument20 pagesNIH Public Access: Interventions For Acute Internal HordeolumhilmanNo ratings yet
- Jurnal: Efikasi Kombinasi Artesunate-Amodiaquine Pada Pengobatan Malaria Falciparum Tanpa Komplikasi Di MadagaskarDocument26 pagesJurnal: Efikasi Kombinasi Artesunate-Amodiaquine Pada Pengobatan Malaria Falciparum Tanpa Komplikasi Di MadagaskarDea Melinda SabilaNo ratings yet
- Maquinas ElectricasDocument4 pagesMaquinas ElectricasDiego GabrielNo ratings yet
- Effects of Chalazia On Corneal AstigmatismDocument9 pagesEffects of Chalazia On Corneal AstigmatismDea Melinda SabilaNo ratings yet
- Blanko Ujian Status Pasien Klinik Penyakit DalamDocument16 pagesBlanko Ujian Status Pasien Klinik Penyakit DalamDea Melinda SabilaNo ratings yet
- Dyspepsia in ESRD PatientsDocument4 pagesDyspepsia in ESRD PatientsDea Melinda SabilaNo ratings yet
- Efficacy of Artesunate-Amodiaquine in The Treatment of Falciparum Uncomplicated Malaria in MadagascarDocument7 pagesEfficacy of Artesunate-Amodiaquine in The Treatment of Falciparum Uncomplicated Malaria in MadagascarDea Melinda SabilaNo ratings yet
- Efficacy of Artesunate-Amodiaquine in The Treatment of Falciparum Uncomplicated Malaria in MadagascarDocument7 pagesEfficacy of Artesunate-Amodiaquine in The Treatment of Falciparum Uncomplicated Malaria in MadagascarDea Melinda SabilaNo ratings yet
- Laparoscopic Versus Open Transhiatal Esophagectomy For Distal and Junction CancerDocument6 pagesLaparoscopic Versus Open Transhiatal Esophagectomy For Distal and Junction CancerDea Melinda SabilaNo ratings yet
- Jurnal Reading TrikiasisDocument7 pagesJurnal Reading TrikiasisDea Melinda SabilaNo ratings yet
- Dyspepsia in ESRD PatientsDocument4 pagesDyspepsia in ESRD PatientsDea Melinda SabilaNo ratings yet
- Surat Sponsor Orang TuaDocument1 pageSurat Sponsor Orang TuaDea Melinda SabilaNo ratings yet
- Prostatitis: Symptoms, Causes and TreatmentsDocument16 pagesProstatitis: Symptoms, Causes and TreatmentsjoserodrrNo ratings yet
- Ref Paczosa TatedaDocument33 pagesRef Paczosa TatedaJuan Martín VargasNo ratings yet
- Incontinence Case StudyDocument26 pagesIncontinence Case StudyRose AnnNo ratings yet
- Escherichia Coli: Jan T Poolman, Bacterial Vaccine Discovery & Early Development, Janssen, Leiden, The NetherlandsDocument9 pagesEscherichia Coli: Jan T Poolman, Bacterial Vaccine Discovery & Early Development, Janssen, Leiden, The NetherlandsSelma DerbalNo ratings yet
- NMJ VOL5 NO2 Final 44 49Document6 pagesNMJ VOL5 NO2 Final 44 49Ravi GuptaNo ratings yet
- Drought Needs Assessment Somaliland PDFDocument39 pagesDrought Needs Assessment Somaliland PDFOmar AwaleNo ratings yet
- Understanding the Common Findings in our Annual Physical ExaminationDocument18 pagesUnderstanding the Common Findings in our Annual Physical ExaminationCherrie AngcaoNo ratings yet
- 2013 EAUN Guideline Milan 2013-Lr DEF PDFDocument98 pages2013 EAUN Guideline Milan 2013-Lr DEF PDFdr5y3dNo ratings yet
- Parsley - A Traditional UTI Remedy and A Recipe For Parsley TeaDocument1 pageParsley - A Traditional UTI Remedy and A Recipe For Parsley TeaSu H HarthyNo ratings yet
- CL7 Urinary Tract Infection 20192020-20191212060056Document50 pagesCL7 Urinary Tract Infection 20192020-20191212060056Nur Ain IzzatiNo ratings yet
- Health: Quarter 2-Module 4Document27 pagesHealth: Quarter 2-Module 4Hannah BautistaNo ratings yet
- Types of urine tests revealedDocument2 pagesTypes of urine tests revealedRamon AzurNo ratings yet
- Urinary Germicides PharmaDocument11 pagesUrinary Germicides PharmaMaria Pina Barbado PonceNo ratings yet
- Case Study P.TDocument5 pagesCase Study P.TSharon WilliamsNo ratings yet
- ResearchDocument38 pagesResearchHelen McClintockNo ratings yet
- Case Simulation 117Document3 pagesCase Simulation 117Dudong SasakiNo ratings yet
- Amenorrhea Ovarian TumorsDocument18 pagesAmenorrhea Ovarian TumorsJeremy ShimlerNo ratings yet
- Childhood IllnessDocument32 pagesChildhood IllnessJesseNo ratings yet
- Practical MedicineDocument630 pagesPractical MedicineYong Lim80% (5)
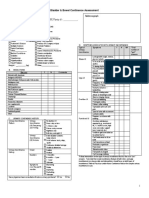
- Bladder & Bowel Continence Assessment: Chart (C), RN, RPN, PSW, OtherDocument4 pagesBladder & Bowel Continence Assessment: Chart (C), RN, RPN, PSW, OtherMeenakshiputraeashwarprasad MacherlaNo ratings yet
- Guias Europeas de UroanalisisDocument96 pagesGuias Europeas de UroanalisisMichael Hood100% (3)
- Anatomy and PhysiologyDocument4 pagesAnatomy and PhysiologyCris Joe Rollorata DumagalNo ratings yet
- ICPC 2 EnglishDocument2 pagesICPC 2 EnglishErlangga Pati KawaNo ratings yet
- Identifying Healthcare-Associated Infections (HAI) For NHSN SurveillanceDocument27 pagesIdentifying Healthcare-Associated Infections (HAI) For NHSN SurveillanceInter 4DMNo ratings yet
- ArbutinDocument38 pagesArbutinWajah IndahNo ratings yet
- ESTAVILLO, Karen G. (FEVER UTI, CONSTI)Document4 pagesESTAVILLO, Karen G. (FEVER UTI, CONSTI)Karen EstavilloNo ratings yet