You might also like
- Peptide and Protein DeliveryFrom EverandPeptide and Protein DeliveryChris Van Der WalleRating: 2 out of 5 stars2/5 (1)
- Enteral Versus Parenteral Nutrition in Critically Ill Patients - An Updated Systematic Review and Meta-Analysis of Randomized Controlled TrialsDocument14 pagesEnteral Versus Parenteral Nutrition in Critically Ill Patients - An Updated Systematic Review and Meta-Analysis of Randomized Controlled TrialsLea Bali Ulina SinurayaNo ratings yet
- Contro Pacientes DiabeticosDocument3 pagesContro Pacientes DiabeticosFrancisco Josue TinajeroNo ratings yet
- Eckert 2021Document10 pagesEckert 2021Igor EckertNo ratings yet
- ProteinasDocument9 pagesProteinaspauly 111No ratings yet
- 2015 Article 1002Document16 pages2015 Article 1002Nutricion 2018No ratings yet
- Disclosure of Interest: None DeclaredDocument1 pageDisclosure of Interest: None DeclaredLilíNo ratings yet
- Metanalisi ProbioticiDocument25 pagesMetanalisi ProbioticiLuigi LattucaNo ratings yet
- Glutamin Medi 94 E1319Document12 pagesGlutamin Medi 94 E1319Octavianus KevinNo ratings yet
- Asemi 2015Document7 pagesAsemi 2015ahmad azhar marzuqiNo ratings yet
- Fnut 08 716783Document15 pagesFnut 08 716783LorenzoNo ratings yet
- Ref 9 - García AlmeidaDocument2 pagesRef 9 - García AlmeidajavierNo ratings yet
- Glutamine: Role in Critical Illness and Ongoing Clinical TrialsDocument8 pagesGlutamine: Role in Critical Illness and Ongoing Clinical TrialsapyfNo ratings yet
- Omega 3 RCTDocument8 pagesOmega 3 RCTtoooqaaa21No ratings yet
- MIB 0b013e31828f5198Document9 pagesMIB 0b013e31828f5198canaltempolivreNo ratings yet
- Contoh Literature ReviewDocument12 pagesContoh Literature ReviewDenny EmiliusNo ratings yet
- Dietary Management and Major Clinical Events With LCHADDocument6 pagesDietary Management and Major Clinical Events With LCHADItzel Carrillo NietoNo ratings yet
- Mmunotec Edical UblicationsDocument23 pagesMmunotec Edical Ublicationsapi-26034055No ratings yet
- 384 2017 Article 2958Document11 pages384 2017 Article 2958FranciscoNo ratings yet
- Berger-Monitoreo Nutricional en UCI-2018Document10 pagesBerger-Monitoreo Nutricional en UCI-2018Brayan AuntaNo ratings yet
- Song 2014Document11 pagesSong 2014Ayssa WitjaksonoNo ratings yet
- Zhou2019 Article InsulinDegludecANovelUltra-LonDocument18 pagesZhou2019 Article InsulinDegludecANovelUltra-LonmehakNo ratings yet
- Effect of A Glutamine-Enriched Enteral Diet OnDocument6 pagesEffect of A Glutamine-Enriched Enteral Diet Ondiajeng gayatriNo ratings yet
- 5044-17662-1-PB Neomune PDFDocument11 pages5044-17662-1-PB Neomune PDFSIUSANTO HadiNo ratings yet
- Saglimbene2021 Article DietaryIntakeInAdultsOnHemodiaDocument9 pagesSaglimbene2021 Article DietaryIntakeInAdultsOnHemodiaKevin OwenNo ratings yet
- Fungal Beta-Glucans As Adjuvants For Treating Cancer Patients - Revisão Sistemática de ECRDocument10 pagesFungal Beta-Glucans As Adjuvants For Treating Cancer Patients - Revisão Sistemática de ECRMaria Vitória Cota de AbreuNo ratings yet
- A Randomized, Controlled Trial of Liraglutide For Adolescents With ObesityDocument12 pagesA Randomized, Controlled Trial of Liraglutide For Adolescents With ObesityWarun KumarNo ratings yet
- BIOS LIFE - Cleveland Clinic Trial by Dr. Dennis SprecherDocument5 pagesBIOS LIFE - Cleveland Clinic Trial by Dr. Dennis SprecherHisWellnessNo ratings yet
- Nej Mo A 2206038Document12 pagesNej Mo A 2206038dravlamfNo ratings yet
- Evidence-Based Treatmentsin Pemphigusvulgaris Andpemphigus FoliaceusDocument8 pagesEvidence-Based Treatmentsin Pemphigusvulgaris Andpemphigus FoliaceusCharly EscobarNo ratings yet
- 2 51 1624856559 Ijmpsdec20213Document10 pages2 51 1624856559 Ijmpsdec20213TJPRC PublicationsNo ratings yet
- Jurnal Perbandingan DM PDFDocument8 pagesJurnal Perbandingan DM PDFSigit DwiyantoNo ratings yet
- Probiotics Contribute To Glycemic Control in Patients With Type 2 Diabetes Mellitus, A Systematic Review and Meta-AnalysisDocument13 pagesProbiotics Contribute To Glycemic Control in Patients With Type 2 Diabetes Mellitus, A Systematic Review and Meta-Analysisภัคจิรา ทองนะNo ratings yet
- Freguency Diabetologia 2014Document10 pagesFreguency Diabetologia 2014ANGEL ALEXANDER BENITESNo ratings yet
- Efficacy of Lifestyle Interventions in Patients With Type 2 Diabetes - A Systematic Review and Meta-AnalysisDocument11 pagesEfficacy of Lifestyle Interventions in Patients With Type 2 Diabetes - A Systematic Review and Meta-AnalysisDara Agusti MaulidyaNo ratings yet
- Intoxicacion Por Betabloqueadores ToxicologyDocument42 pagesIntoxicacion Por Betabloqueadores ToxicologyIza ÁlvarezNo ratings yet
- 1 s2.0 S0272638619311151 MainDocument17 pages1 s2.0 S0272638619311151 Main吴善统No ratings yet
- Dgac 661Document10 pagesDgac 661bdcqmnb4tzNo ratings yet
- Nutrition Journal: Nutrition Support in Cancer Patients: A Brief Review and Suggestion For Standard Indications CriteriaDocument5 pagesNutrition Journal: Nutrition Support in Cancer Patients: A Brief Review and Suggestion For Standard Indications CriteriaSunardiasihNo ratings yet
- Dapagli Ozin Treatment For Type 2 Diabetes: A Systematic Review and Meta-Analysis of Randomized Controlled TrialsDocument18 pagesDapagli Ozin Treatment For Type 2 Diabetes: A Systematic Review and Meta-Analysis of Randomized Controlled TrialsVictoria Maya ChyntiaNo ratings yet
- Adipokines and Systemic Inflammation in Weight-Losing Lung Cancer PatientsDocument6 pagesAdipokines and Systemic Inflammation in Weight-Losing Lung Cancer PatientsAnna GozaliNo ratings yet
- Review Article: DPP-4 Inhibitors As Treatments For Type 1 Diabetes Mellitus: A Systematic Review and Meta-AnalysisDocument11 pagesReview Article: DPP-4 Inhibitors As Treatments For Type 1 Diabetes Mellitus: A Systematic Review and Meta-AnalysisGREESTYNo ratings yet
- E3 FullDocument2 pagesE3 FullafandianddonkeyNo ratings yet
- Glutamine, Fish Oil and Antioxidants in Critical Illness: Metaplus Trial Post Hoc Safety AnalysisDocument12 pagesGlutamine, Fish Oil and Antioxidants in Critical Illness: Metaplus Trial Post Hoc Safety AnalysisAni E GuamánNo ratings yet
- Fnut 09 961207Document12 pagesFnut 09 961207mamcn unhasNo ratings yet
- Sremanakova Et Al-2018-Journal of Human Nutrition and DieteticsDocument11 pagesSremanakova Et Al-2018-Journal of Human Nutrition and DieteticsLulu BadriyahNo ratings yet
- Fphar 13 1021584Document11 pagesFphar 13 1021584topanNo ratings yet
- Colistin Monotherapy Versus Combination Therapy For Carbapenem-Resistant Organisms NEJM EvidenceDocument27 pagesColistin Monotherapy Versus Combination Therapy For Carbapenem-Resistant Organisms NEJM Evidencerac.oncologyNo ratings yet
- Hepatology - April 1993 - Mendenhall - A Study of Oral Nutritional Support With Oxandrolone in Malnourished Patients WithDocument13 pagesHepatology - April 1993 - Mendenhall - A Study of Oral Nutritional Support With Oxandrolone in Malnourished Patients WithkentryzbustamanteNo ratings yet
- 2022 JastreboffDocument12 pages2022 JastreboffSinityNo ratings yet
- Effect of Restricted Protein Diet Supplemented WitDocument11 pagesEffect of Restricted Protein Diet Supplemented WitBogdan LeonardNo ratings yet
- Antidiabetic Potential of Phycocyanin: Effects On Kkay Mice: Pharmaceutical Biology February 2013Document8 pagesAntidiabetic Potential of Phycocyanin: Effects On Kkay Mice: Pharmaceutical Biology February 2013faizahNo ratings yet
- Complementary Therapies in Medicine: SciencedirectDocument11 pagesComplementary Therapies in Medicine: SciencedirectNejc KovačNo ratings yet
- Tight Glycemic Control in Critically Ill PediatricDocument11 pagesTight Glycemic Control in Critically Ill Pediatricbella friscaamaliaNo ratings yet
- Fphys 13 960580Document13 pagesFphys 13 960580غاز الشمالNo ratings yet
- Https:/zero Sci-Hub Se/5089//boulet2016Document10 pagesHttps:/zero Sci-Hub Se/5089//boulet2016Caroline QueirogaNo ratings yet
- Tight GlycemicDocument10 pagesTight GlycemicIsmail Mohammed AbdelgawadNo ratings yet
- Probiotics For The Management of Type 2 Diabetes MellitusDocument11 pagesProbiotics For The Management of Type 2 Diabetes MellitusKelly BarrosNo ratings yet
- SLIDE JURNAL DHR MTDocument29 pagesSLIDE JURNAL DHR MTTenyson AnalauwNo ratings yet
- J Clin Endocrinol Metab. 2012 97 16 38Document23 pagesJ Clin Endocrinol Metab. 2012 97 16 38rizwan234No ratings yet
- Maternal Child Nursing Care Perry Hockenberry Lowdermilk 5th Edition Test BankDocument13 pagesMaternal Child Nursing Care Perry Hockenberry Lowdermilk 5th Edition Test Bankthiamity35n0No ratings yet
- Prescription - Apollo 2471659105066202Document2 pagesPrescription - Apollo 2471659105066202JEENEET CHEMISTRYNo ratings yet
- E-Learning, Telemadicin, Tele Nursing AssignmentDocument22 pagesE-Learning, Telemadicin, Tele Nursing AssignmentBhawna Joshi100% (2)
- Social and Political Issues Debate TopicsDocument6 pagesSocial and Political Issues Debate TopicsbjdevhervehroheghghbhbhotbhhortbhNo ratings yet
- Classification of Nursing Theory Developed by Nursing ExpertsDocument49 pagesClassification of Nursing Theory Developed by Nursing ExpertsVhaNo ratings yet
- Bonded Composites Versus Ceramic Veneers PDFDocument7 pagesBonded Composites Versus Ceramic Veneers PDFAnnaAffandieNo ratings yet
- Prescribing BenzoDocument10 pagesPrescribing BenzoAndreea CraioveanuNo ratings yet
- Enteric BacteriaDocument16 pagesEnteric BacteriaBernie QuepNo ratings yet
- Resume Iggy Hernandez FinalDocument1 pageResume Iggy Hernandez Finalapi-379228020No ratings yet
- JMIR Med Edu - Response To Letter To Editor - USMLE Step 1 Pass Fail ChangeDocument3 pagesJMIR Med Edu - Response To Letter To Editor - USMLE Step 1 Pass Fail ChangeAhmad OzairNo ratings yet
- Patient Rights Audit ToolsDocument4 pagesPatient Rights Audit ToolsAbdur Rashid KhanNo ratings yet
- Rubrics NCP NCM 103 SL Funda VSDocument1 pageRubrics NCP NCM 103 SL Funda VSJohn TacordaJrNo ratings yet
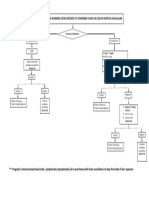
- Management of Healthcare Workers (HCW) Exposed To Confirmed Covid-19 Case in Hospital Shah AlamDocument1 pageManagement of Healthcare Workers (HCW) Exposed To Confirmed Covid-19 Case in Hospital Shah AlamNurhafizah IbrahimNo ratings yet
- Compre FundaDocument10 pagesCompre FundaAngie SaquingNo ratings yet
- LGD-4033 Cycle (Ligandrol Cycle Guide) - Steroid CyclesDocument22 pagesLGD-4033 Cycle (Ligandrol Cycle Guide) - Steroid Cyclesmaxime.rivasNo ratings yet
- Iligan City Hospital 1Document3 pagesIligan City Hospital 1danny17phNo ratings yet
- Blumel Et Al - Germany System HealthDocument308 pagesBlumel Et Al - Germany System HealthVictor Hugo Loaiza SeguraNo ratings yet
- Answer and Rationale LMRDocument23 pagesAnswer and Rationale LMRCharles Gerard B. BeluanNo ratings yet
- PharmacyDocument20 pagesPharmacyRajJoshiNo ratings yet
- Ethiopia: Community Health RoadmapDocument18 pagesEthiopia: Community Health Roadmapyonas yohannesNo ratings yet
- NICUDocument190 pagesNICUSoat Alfajer100% (2)
- 8 Things To Consider About BiocompatibilityDocument2 pages8 Things To Consider About BiocompatibilityYousif Jamal MahboubaNo ratings yet
- CPT Modifier NewDocument10 pagesCPT Modifier NewSeenuvasanLeeManiNo ratings yet
- Medical School Application Guide 1Document17 pagesMedical School Application Guide 1Marilyn CitadelNo ratings yet
- Burning Mouth Syndrome and Treatment With ParoxetinDocument2 pagesBurning Mouth Syndrome and Treatment With ParoxetinFitri AngginiNo ratings yet
- Kaloji Narayana Rao University of Health Sciences: Telangana WARANGAL 506 002 PG Degree Md/Ms Dissertation Topics For The Academic Year 2021-22Document104 pagesKaloji Narayana Rao University of Health Sciences: Telangana WARANGAL 506 002 PG Degree Md/Ms Dissertation Topics For The Academic Year 2021-22sateesh reddiNo ratings yet
- Bill 15Document296 pagesBill 15Ctv Montreal100% (1)
- Reggie Bert R. Sintos B.S. Architecture 4-A Eastern Visayas State UniversityDocument1 pageReggie Bert R. Sintos B.S. Architecture 4-A Eastern Visayas State UniversityRoberto R. SintosNo ratings yet
- Medical MalpracticeDocument10 pagesMedical MalpracticeSakshi Suri100% (2)
- Adolescent Informed Consent - KannadaDocument5 pagesAdolescent Informed Consent - KannadaKrishna BhatNo ratings yet
- Instant Loss On a Budget: Super-Affordable Recipes for the Health-Conscious CookFrom EverandInstant Loss On a Budget: Super-Affordable Recipes for the Health-Conscious CookRating: 3.5 out of 5 stars3.5/5 (2)
- Body Love Every Day: Choose Your Life-Changing 21-Day Path to Food FreedomFrom EverandBody Love Every Day: Choose Your Life-Changing 21-Day Path to Food FreedomRating: 4 out of 5 stars4/5 (1)
- The Body Book: The Law of Hunger, the Science of Strength, and Other Ways to Love Your Amazing BodyFrom EverandThe Body Book: The Law of Hunger, the Science of Strength, and Other Ways to Love Your Amazing BodyNo ratings yet
- Summary: Fast Like a Girl: A Woman’s Guide to Using the Healing Power of Fasting to Burn Fat, Boost Energy, and Balance Hormones: Key Takeaways, Summary and AnalysisFrom EverandSummary: Fast Like a Girl: A Woman’s Guide to Using the Healing Power of Fasting to Burn Fat, Boost Energy, and Balance Hormones: Key Takeaways, Summary and AnalysisRating: 3 out of 5 stars3/5 (2)
- Summary of Mary Claire Haver's The Galveston DietFrom EverandSummary of Mary Claire Haver's The Galveston DietRating: 5 out of 5 stars5/5 (1)
- Forever Strong: A New, Science-Based Strategy for Aging WellFrom EverandForever Strong: A New, Science-Based Strategy for Aging WellNo ratings yet
- Gut: The Inside Story of Our Body's Most Underrated Organ (Revised Edition)From EverandGut: The Inside Story of Our Body's Most Underrated Organ (Revised Edition)Rating: 4 out of 5 stars4/5 (378)
- The Food Lover's Cleanse: 140 Delicious, Nourishing Recipes That Will Tempt You Back into Healthful EatingFrom EverandThe Food Lover's Cleanse: 140 Delicious, Nourishing Recipes That Will Tempt You Back into Healthful EatingRating: 4 out of 5 stars4/5 (3)
- Metabolism Revolution: Lose 14 Pounds in 14 Days and Keep It Off for LifeFrom EverandMetabolism Revolution: Lose 14 Pounds in 14 Days and Keep It Off for LifeNo ratings yet
- Intermittent Fasting Basics for Women: The Complete Guide to Safe and Effective Weight Loss with Intermittent FastingFrom EverandIntermittent Fasting Basics for Women: The Complete Guide to Safe and Effective Weight Loss with Intermittent FastingRating: 5 out of 5 stars5/5 (12)
- Sugar Crush: How to Reduce Inflammation, Reverse Nerve Damage, and Reclaim Good HealthFrom EverandSugar Crush: How to Reduce Inflammation, Reverse Nerve Damage, and Reclaim Good HealthRating: 4 out of 5 stars4/5 (6)
- The Beck Diet Solution Weight Loss Workbook: The 6-Week Plan to Train Your Brain to Think Like a Thin PersonFrom EverandThe Beck Diet Solution Weight Loss Workbook: The 6-Week Plan to Train Your Brain to Think Like a Thin PersonRating: 3.5 out of 5 stars3.5/5 (33)
- The Diabetes Code: Prevent and Reverse Type 2 Diabetes NaturallyFrom EverandThe Diabetes Code: Prevent and Reverse Type 2 Diabetes NaturallyRating: 4.5 out of 5 stars4.5/5 (2)
- Eat to Lose, Eat to Win: Your Grab-n-Go Action Plan for a Slimmer, Healthier YouFrom EverandEat to Lose, Eat to Win: Your Grab-n-Go Action Plan for a Slimmer, Healthier YouNo ratings yet
- The Diet Trap Solution: Train Your Brain to Lose Weight and Keep It Off for GoodFrom EverandThe Diet Trap Solution: Train Your Brain to Lose Weight and Keep It Off for GoodNo ratings yet
- The Candida Cure: The 90-Day Program to Balance Your Gut, Beat Candida, and Restore Vibrant HealthFrom EverandThe Candida Cure: The 90-Day Program to Balance Your Gut, Beat Candida, and Restore Vibrant HealthNo ratings yet
- Secrets From the Eating Lab: The Science of Weight Loss, the Myth of Willpower, and Why You Should Never Diet AgainFrom EverandSecrets From the Eating Lab: The Science of Weight Loss, the Myth of Willpower, and Why You Should Never Diet AgainRating: 3.5 out of 5 stars3.5/5 (38)
- The Arm: Inside the Billion-Dollar Mystery of the Most Valuable Commodity in SportsFrom EverandThe Arm: Inside the Billion-Dollar Mystery of the Most Valuable Commodity in SportsRating: 4 out of 5 stars4/5 (49)
- Find Your Path: Honor Your Body, Fuel Your Soul, and Get Strong with the Fit52 LifeFrom EverandFind Your Path: Honor Your Body, Fuel Your Soul, and Get Strong with the Fit52 LifeRating: 4 out of 5 stars4/5 (3)
- Keto Friendly Recipes: Easy Keto For Busy PeopleFrom EverandKeto Friendly Recipes: Easy Keto For Busy PeopleRating: 3.5 out of 5 stars3.5/5 (2)
- How Not to Die by Michael Greger MD, Gene Stone - Book Summary: Discover the Foods Scientifically Proven to Prevent and Reverse DiseaseFrom EverandHow Not to Die by Michael Greger MD, Gene Stone - Book Summary: Discover the Foods Scientifically Proven to Prevent and Reverse DiseaseRating: 4.5 out of 5 stars4.5/5 (83)
- The End of Craving: Recovering the Lost Wisdom of Eating WellFrom EverandThe End of Craving: Recovering the Lost Wisdom of Eating WellRating: 4.5 out of 5 stars4.5/5 (80)
- Rapid Weight Loss Hypnosis: Deep Sleep Your Way to Rapid Weight Loss, Healing Your Body and Self Esteem with Guided Meditations and Positive AffirmationsFrom EverandRapid Weight Loss Hypnosis: Deep Sleep Your Way to Rapid Weight Loss, Healing Your Body and Self Esteem with Guided Meditations and Positive AffirmationsRating: 5 out of 5 stars5/5 (7)
- How to Be Well: The 6 Keys to a Happy and Healthy LifeFrom EverandHow to Be Well: The 6 Keys to a Happy and Healthy LifeRating: 5 out of 5 stars5/5 (1)
- Happy Gut: The Cleansing Program to Help You Lose Weight, Gain Energy, and Eliminate PainFrom EverandHappy Gut: The Cleansing Program to Help You Lose Weight, Gain Energy, and Eliminate PainRating: 3.5 out of 5 stars3.5/5 (6)
- Proteinaholic: How Our Obsession with Meat Is Killing Us and What We Can Do About ItFrom EverandProteinaholic: How Our Obsession with Meat Is Killing Us and What We Can Do About ItRating: 4.5 out of 5 stars4.5/5 (19)
- Foods That Cause You to Lose Weight: The Negative Calorie EffectFrom EverandFoods That Cause You to Lose Weight: The Negative Calorie EffectRating: 3 out of 5 stars3/5 (5)