You might also like
- The Power Behind Your Eyes: Improving Your Eyesight with Integrated Vision TherapyFrom EverandThe Power Behind Your Eyes: Improving Your Eyesight with Integrated Vision TherapyNo ratings yet
- Controlling Myopia Progression in Children and AdolescentsDocument12 pagesControlling Myopia Progression in Children and AdolescentsTakhta AlfinaNo ratings yet
- 1 s2.0 S1367048416000059 MainDocument3 pages1 s2.0 S1367048416000059 MainArturo GuilliemNo ratings yet
- Myopia Control: A Review: Jeffrey J. WallineDocument6 pagesMyopia Control: A Review: Jeffrey J. WallineChristine Yohana SianturiNo ratings yet
- How To Use Low Dose Atropin To Slow Myopic Progression in KidsDocument3 pagesHow To Use Low Dose Atropin To Slow Myopic Progression in Kidsrak3uNo ratings yet
- World Sight Day - 13 October 2022Document2 pagesWorld Sight Day - 13 October 2022Times MediaNo ratings yet
- Review On The Myopia PandemicDocument8 pagesReview On The Myopia PandemicIlona HiariejNo ratings yet
- Atropine Treatment 1Document7 pagesAtropine Treatment 1Chris ChowNo ratings yet
- Myopia ControlDocument3 pagesMyopia ControlEric Chow100% (1)
- Epidemiologia Miopia UsaDocument7 pagesEpidemiologia Miopia Usabrenda elielNo ratings yet
- Glaucoma 9Document13 pagesGlaucoma 9Sheila Kussler TalgattiNo ratings yet
- Atropine For The Prevention of Myopia Progression in ChildrenDocument10 pagesAtropine For The Prevention of Myopia Progression in ChildrenWenny AgustinNo ratings yet
- Myopia 1Document2 pagesMyopia 1wn_xngNo ratings yet
- Amblyopia NCBI Journal PDFDocument24 pagesAmblyopia NCBI Journal PDFDea PhillyaNo ratings yet
- HHS Public Access: Advances in Dry Eye Disease TreatmentDocument25 pagesHHS Public Access: Advances in Dry Eye Disease TreatmentjojdoNo ratings yet
- Myopia - Incidence, Pathogenesis, Management and New Possibilities of TreatmentDocument7 pagesMyopia - Incidence, Pathogenesis, Management and New Possibilities of TreatmenthanaddulNo ratings yet
- Prevalence and Progression of Myopia in Children at RaipurDocument9 pagesPrevalence and Progression of Myopia in Children at RaipurInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Clinical Review MyopiaDocument5 pagesClinical Review MyopiaWing Yan LamNo ratings yet
- Cause of Amblyopia in Adult Patients A Cross-Sectional StudyDocument5 pagesCause of Amblyopia in Adult Patients A Cross-Sectional StudyRagni MishraNo ratings yet
- 1 s2.0 S1091853116304438 MainDocument6 pages1 s2.0 S1091853116304438 MainMarcella PolittonNo ratings yet
- Atropine For The Prevention of Myopia Progression in ChildrenDocument10 pagesAtropine For The Prevention of Myopia Progression in ChildrenDwi ZirobeNo ratings yet
- Case 1 Anisometropia Phs Usa PDFDocument10 pagesCase 1 Anisometropia Phs Usa PDFZuhud Zinedine PangindraNo ratings yet
- Manage Adult ExotropiaDocument3 pagesManage Adult ExotropiaTlati AmineNo ratings yet
- Exotropiain AdultsDocument3 pagesExotropiain AdultsTlati AmineNo ratings yet
- Exotropiain AdultsDocument3 pagesExotropiain AdultsTlati AmineNo ratings yet
- Optimal Management of Pediatric Keratoconus: Challenges and SolutionsDocument9 pagesOptimal Management of Pediatric Keratoconus: Challenges and SolutionsJesus Rodriguez NoriegaNo ratings yet
- The Current Management Strategies For Myopia Control in Children: Mini ReviewDocument3 pagesThe Current Management Strategies For Myopia Control in Children: Mini Reviewlona diolandaNo ratings yet
- Congenital Cataract-Approach and Management ReviewDocument6 pagesCongenital Cataract-Approach and Management ReviewFirgietaPotterNo ratings yet
- IMI - Prevention of Myopia and Its ProgressionDocument10 pagesIMI - Prevention of Myopia and Its ProgressionJesse James Arteaga PeraltaNo ratings yet
- The Best and Worst Habbits For Eyesight-1Document2 pagesThe Best and Worst Habbits For Eyesight-1윤호진No ratings yet
- NEI Guide to Amblyopia Causes and TreatmentsDocument5 pagesNEI Guide to Amblyopia Causes and TreatmentsWinda TambunanNo ratings yet
- NEI Guide to Amblyopia Causes and TreatmentsDocument5 pagesNEI Guide to Amblyopia Causes and Treatmentsmifta galuhNo ratings yet
- Strabismus: Kammi B. Gunton,, Barry N. Wasserman,, Caroline DebenedictisDocument15 pagesStrabismus: Kammi B. Gunton,, Barry N. Wasserman,, Caroline DebenedictisWendy Garduño SandovalNo ratings yet
- Energetic Eyehealing - The New Paradigm of Eye Medicine CategoriesDocument6 pagesEnergetic Eyehealing - The New Paradigm of Eye Medicine CategoriesMadon MariaNo ratings yet
- Myopia New AiocDocument44 pagesMyopia New Aiocneha midhaNo ratings yet
- Study of Vision Screening in School Children Between 5 and 15 YearsDocument16 pagesStudy of Vision Screening in School Children Between 5 and 15 YearsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Association of Asthenopia and Convergence Insufficiency in Children With Refractive Error-A Hospital Based StudyDocument6 pagesAssociation of Asthenopia and Convergence Insufficiency in Children With Refractive Error-A Hospital Based StudySilvia RNo ratings yet
- AtropinDocument36 pagesAtropintegarbondanNo ratings yet
- Evaluation and Management of Drug Resistant Epilepsy in ChildrenDocument10 pagesEvaluation and Management of Drug Resistant Epilepsy in ChildrenAzizah HalidNo ratings yet
- FDA Petition to Require Eye Professionals Advise on Myopia PreventionDocument58 pagesFDA Petition to Require Eye Professionals Advise on Myopia PreventionNguyen Thi van AnhNo ratings yet
- Juvenile Myopia Progression, Risk Factors and Interventions: Pediatric Ophthalmology UpdateDocument5 pagesJuvenile Myopia Progression, Risk Factors and Interventions: Pediatric Ophthalmology UpdateZhakiAlAsrorNo ratings yet
- Myopia - EyeWikiDocument1 pageMyopia - EyeWikiRima MaulinaNo ratings yet
- Guidelines For Automated Preschool Vision Screening: A 10-Year, Evidence-Based UpdateDocument5 pagesGuidelines For Automated Preschool Vision Screening: A 10-Year, Evidence-Based UpdateSyarifah Thalita NabillaNo ratings yet
- Tsai WS Et Al, 2020Document8 pagesTsai WS Et Al, 2020Muhammad Sidqi FahmiNo ratings yet
- Managing Myopia Clinical Guide Dec 2020Document12 pagesManaging Myopia Clinical Guide Dec 2020Jorge Ivan Carcache LopezNo ratings yet
- BCLA YOUR CHILD & MYOPIA Factsheet FVDocument2 pagesBCLA YOUR CHILD & MYOPIA Factsheet FVJorge CarcacheNo ratings yet
- 94 - CH 10 - Symptoms in Heterophoria and Heterotropia and The Psychological Effects of Strabismus P. 153-157Document5 pages94 - CH 10 - Symptoms in Heterophoria and Heterotropia and The Psychological Effects of Strabismus P. 153-157Catleya ProtacioNo ratings yet
- Eye Infections PDFDocument10 pagesEye Infections PDFDara Agusti MaulidyaNo ratings yet
- Evaluation of The Efficacy and Safety of A New Device For Eye Drops Instillation in Patients With GlaucomaDocument6 pagesEvaluation of The Efficacy and Safety of A New Device For Eye Drops Instillation in Patients With GlaucomajustintanmdNo ratings yet
- Antiepileptic Drug Treatment of Epilepsy in ChildrenDocument27 pagesAntiepileptic Drug Treatment of Epilepsy in ChildrenYunierNo ratings yet
- Morgan 2016Document3 pagesMorgan 2016angela_karenina_1No ratings yet
- Glaucoma Guide: Signs, Symptoms, Types & TreatmentDocument15 pagesGlaucoma Guide: Signs, Symptoms, Types & Treatmentyangi dokaNo ratings yet
- Nursing Care Plan for Hyperopia-Induced Visual ImpairmentDocument6 pagesNursing Care Plan for Hyperopia-Induced Visual ImpairmentgeeneevzzNo ratings yet
- Age of Onset of Hyperopia - 2010Document5 pagesAge of Onset of Hyperopia - 2010Rafael IribarrenNo ratings yet
- Pediatric Ophthalmology and Strabismus - PDF RoomDocument208 pagesPediatric Ophthalmology and Strabismus - PDF RoomjohannaNo ratings yet
- Current Management of Childhood Amblyopia: Shin Hae ParkDocument12 pagesCurrent Management of Childhood Amblyopia: Shin Hae ParkSyarifah Thalita NabillaNo ratings yet
- Literature Review On Refractive ErrorsDocument5 pagesLiterature Review On Refractive Errorsafmzfvlopbchbe100% (1)
- 4 5837051926121809399 PDFDocument119 pages4 5837051926121809399 PDFSrinivas PingaliNo ratings yet
- World Sight Day - 8 October 2020Document7 pagesWorld Sight Day - 8 October 2020Times MediaNo ratings yet
- Conversion Cycle (Process Cost) : Rizal Technological UniversityDocument25 pagesConversion Cycle (Process Cost) : Rizal Technological UniversityHatdogNo ratings yet
- Review of Dr. Mark Cheng's "Prehab-Rehab 101" SeriesDocument6 pagesReview of Dr. Mark Cheng's "Prehab-Rehab 101" SeriesWilliam TortorielloNo ratings yet
- Flat Slab NoteDocument4 pagesFlat Slab NotesasiNo ratings yet
- Kuruk Etra:: Dharma-K Etra Śalya-ParvaDocument1 pageKuruk Etra:: Dharma-K Etra Śalya-ParvaRavinder Khullar100% (1)
- Sidhil - ICT Design EngineerDocument3 pagesSidhil - ICT Design Engineeratif_aman123No ratings yet
- Instruction Manual: Shimadzu Analytical BalanceDocument169 pagesInstruction Manual: Shimadzu Analytical BalanceChanthar SoeNo ratings yet
- Vedic Healing Through Gems4Document3 pagesVedic Healing Through Gems4gesNo ratings yet
- 255 Introduction Vocational Service enDocument12 pages255 Introduction Vocational Service enDmitri PopaNo ratings yet
- YLE - Top Tips and Common MistakesDocument15 pagesYLE - Top Tips and Common Mistakeskuvan alievNo ratings yet
- Clinical Practice Guidelines On Postmenopausal Osteoporosis: An Executive Summary and Recommendations - Update 2019-2020Document17 pagesClinical Practice Guidelines On Postmenopausal Osteoporosis: An Executive Summary and Recommendations - Update 2019-2020Marwa YassinNo ratings yet
- K Park 24 TH Edition ChangesDocument8 pagesK Park 24 TH Edition ChangesAnkit ChoudharyNo ratings yet
- Deutz td2011 l04w Service Manual PDFDocument7 pagesDeutz td2011 l04w Service Manual PDFLuis Carlos RamosNo ratings yet
- TECHNICALPAPER2Document8 pagesTECHNICALPAPER2spiderwebNo ratings yet
- Analyzing Historical DocumentDocument4 pagesAnalyzing Historical DocumentChristine Joy VillasisNo ratings yet
- RSA Industries, India - Products - Care - Polymeric Non Ionic Fabric Softener - Fabric Softener (RSF-H-SOFT)Document3 pagesRSA Industries, India - Products - Care - Polymeric Non Ionic Fabric Softener - Fabric Softener (RSF-H-SOFT)crplzNo ratings yet
- Oakham Surgery New Patient FormDocument7 pagesOakham Surgery New Patient FormTrần Thanh ThảoNo ratings yet
- Module 5 HomeworkDocument4 pagesModule 5 HomeworkCj LinceNo ratings yet
- Growatt Warranty Procedure - 07-09-2020Document9 pagesGrowatt Warranty Procedure - 07-09-2020Design TeamNo ratings yet
- Senior Power Apps Engineer JobDocument3 pagesSenior Power Apps Engineer JobMichałNo ratings yet
- Imeko WC 2012 TC21 O10Document5 pagesImeko WC 2012 TC21 O10mcastillogzNo ratings yet
- Studi Kasus Pada PT Damar Bandha Jaya Corp. BogorDocument10 pagesStudi Kasus Pada PT Damar Bandha Jaya Corp. BogorMayHan13No ratings yet
- Template PharmaconDocument4 pagesTemplate PharmaconDanang RaharjoNo ratings yet
- Cell Structure & FunctionDocument38 pagesCell Structure & Functiongundogan21100% (1)
- Participation RubricDocument2 pagesParticipation RubricCarmen Ibañez AlvarezNo ratings yet
- Revised Bsy Elementary Siatonwest 2 and Pio-Macahig - 2014-15 As of June 6 2014Document31 pagesRevised Bsy Elementary Siatonwest 2 and Pio-Macahig - 2014-15 As of June 6 2014api-273918959No ratings yet
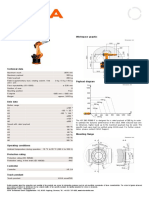
- KR 280 R3080 F technical specificationsDocument1 pageKR 280 R3080 F technical specificationsDorobantu CatalinNo ratings yet
- CaracterizacióndeSalpicadurasSMAW Molleda 2007Document5 pagesCaracterizacióndeSalpicadurasSMAW Molleda 2007Tamara Maria Ortiz MendezNo ratings yet
- Kwame Ture InterviewDocument8 pagesKwame Ture InterviewSumayya K AliNo ratings yet
- SIHI - Control Narrative Proc Compressor UnitDocument5 pagesSIHI - Control Narrative Proc Compressor Unitman_y2k100% (1)
- CIC-presentation of RP-577 PresentationDocument181 pagesCIC-presentation of RP-577 PresentationIbrahim Eldesoky75% (4)