Professional Documents
Culture Documents
Focused Reviews: Pneumococcal Vaccination Strategies
Uploaded by
Rishi MangalOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Focused Reviews: Pneumococcal Vaccination Strategies
Uploaded by
Rishi MangalCopyright:
Available Formats
FOCUSED REVIEWS
Pneumococcal Vaccination Strategies
An Update and Perspective
Andrew C. Berical, Drew Harris, Charles S. Dela Cruz, and Jennifer D. Possick
Section of Pulmonary, Critical Care, and Sleep Medicine, Department of Internal Medicine, Yale School of Medicine, New Haven,
Connecticut
ORCID ID: 0000-0002-5258-1797 (C.S.D.C.).
Abstract stimulate effective antipneumococcal antibody and mucosal
immunity response and immunological memory. Vaccination of
Streptococcus pneumoniae is an important global pathogen that infants and young children with pneumococcal conjugate vaccine has
causes a wide range of clinical disease in children and adults. led to significant decrease in nasal carriage rates and pneumococcal
Pneumococcal pneumonia is by far the common presentation disease in all age groups. Recent pneumococcal vaccine indication
of noninvasive and invasive pneumococcal disease and and schedule recommendations on the basis of age and risk factors
affects the young, the elderly, and the immunocompromised are outlined in this Focused Review. As new pneumococcal vaccine
disproportionately. Patients with chronic pulmonary diseases are recommendations are being followed, continued efforts are needed to
also at higher risk for pneumococcal infections. Substantial address the vaccine efficacy in the waning immunity of the ever-aging
progress over the century has been made in the understanding population, the implementation of vaccines using two different
of pneumococcal immunobiology and the prevention of vaccines under very specific schedules and their real world clinical
invasive pneumococcal disease through vaccination. Currently, two and cost effectiveness, and the development of next generation
pneumococcal vaccines are available for individuals at risk of pneumococcal vaccines.
pneumococcal disease: the 23-valent pneumococcal polysaccharide
vaccine (PPV23) and the 13-valent pneumococcal protein-conjugate Keywords: Streptococcus pneumoniae; pneumonia; PCV-13
vaccine (PCV13). The goal of pneumococcal vaccination is to vaccine; pneumococcal vaccines
(Received in original form November 24, 2015; accepted in final form February 23, 2016 )
Supported by a Patterson Trust Clinical Research Award (C.S.D.C.), Yale Center of Clinical Investigation Clinical Translational Scholar Award (C.S.D.C.),
National Heart, Lung, and Blood Institute grants HL126094 and HL103770 (C.S.D.C.), and a Clinical and Translational Science Award grant UL1 TR000142
(C.S.D.C.) from the National Center for Advancing Translational Science, a component of the National Institutes of Health. The funding bodies had no part in
the writing of the manuscript or the submission.
Correspondence and requests for reprints should be addressed to Charles S. Dela Cruz, M.D., Ph.D., Assistant Professor of Medicine (Pulmonary, Critical Care,
and Sleep Medicine), Yale School of Medicine, 300 Cedar Street, TACS 441D, New Haven, CT 06510. E-mail: charles.delacruz@yale.edu; or Jennifer D. Possick,
M.D., Assistant Professor of Medicine (Pulmonary, Critical Care, and Sleep Medicine); Director, Winchester Chest Clinic, P.O. Box 208057300 Cedar Street, New
Haven, CT 06510-8057. E-mail: jennifer.possick@yale.edu
Ann Am Thorac Soc Vol 13, No 6, pp 933–944, Jun 2016
Copyright © 2016 by the American Thoracic Society
DOI: 10.1513/AnnalsATS.201511-778FR
Internet address: www.atsjournals.org
Streptococcus pneumoniae is an in 900,000 cases and 400,000 estimates an annual invasive pneumococcal
endemic global pathogen that causes hospitalizations annually in the disease incidence of 10.6/100,000 U.S.
a wide range of clinical disease in United States; mortality ranges from population, primarily occurring in adults.
children and adults. Noninvasive 5 to 7% (1). The majority of these cases start with
pneumococcal disease encompasses otitis, Invasive pneumococcal disease implies streptococcal pneumonia as a primary focus.
sinusitis, and community-acquired invasion of pneumococcus into a normally Pneumococcus is the most common cause of
pneumonia. As the name implies, sterile site, leading to complications such as community-acquired pneumonia in adults,
pneumococcal pneumonia is a bacteremia, empyema, meningitis, composing at least 25% of documented
common presentation of noninvasive endocarditis, and osteomyelitis. The Centers cases, with bacteremia present 20% of the
pneumococcal disease, resulting for Disease Control and Prevention time.
Focused Reviews 933
FOCUSED REVIEWS
Epidemiology and Risk Factors Although pneumococcal pneumonia is more complete understanding of the
a leading cause of community-acquired pneumococcal capsular structure
Although invasive pneumococcal disease pneumonia irrespective of comorbidity, had been established, the first tetravalent
is much less prevalent than noninvasive individuals with chronic lung diseases, polysaccharide pneumococcal vaccine was
disease, it confers significant mortality risk particularly those with COPD, are at developed and tested in a large population of
(up to 10% for meningitis and 15% for increased risk of pneumococcal community- Army recruits (20). Although this study did
bacteremia), and survivors can be left with acquired pneumonia and invasive show significant improvement in rates of
significant sequelae (2). Furthermore, given pneumococcal disease, are prone to higher infection with vaccination (Table 1),
the widespread use of empiric antibiotics rates of complications and mortality, and enthusiasm waned with the success of
and frequent lack of timely culture or suffer prolonged recovery after such penicillin. As reports emerged of
urinary antigen data, the true burden of illnesses (16). The reasons for this are resistant pneumococcal infections in
primary and invasive pneumococcal disease many, including reduced innate immunity immunosuppressed, pediatric, and adult
may be significantly underestimated (3). in diseased airways, systemic inflammation, populations, with up to one-quarter of
Certain groups are at particularly high ongoing smoking, acute exacerbations, and patients dying despite appropriate
risk for invasive pneumococcal disease: intermittent use of systemic corticosteroids. antibiotic treatment (21–23), there was
young children, the elderly, and those with In addition, there is ongoing concern renewed interest in effective prophylaxis.
high-risk comorbid diseases or substance about the increased risk for community- In 1977, a 14-valent purified
habits. The Centers for Disease Control acquired pneumonia in the setting of polysaccharide vaccine was approved for use
and Prevention’s Active Bacterial Core chronic use of inhaled corticosteroids, an in the United States, targeting the 14
Surveillance data from 2013 demonstrated important component of maintenance serotypes responsible for more than 75% of
increased rates of invasive pneumococcal therapy in COPD and asthma (17). Because infections at the time. This vaccine
death from pneumococcal pneumonia, even significantly reduced morbidity and
disease in children younger than age 5 years
in absence of invasive disease, is more mortality in healthy adults but notably did
(9.6/100,000 cases) and in adults 65 years
frequent in patients with underlying not reduce overall rates of pneumonia (24).
or older (31/100,000 cases) (4).
chronic pulmonary conditions, appropriate Over the next decade, it became
The elderly in particular have been
and timely vaccination against increasingly apparent that many clinically
consistently shown to have a marked
pneumococcus is an essential component of important pneumococcal infections were
increased risk for invasive pneumococcal
preventative care in this population. occurring despite vaccination, particularly
disease (5, 6). Functional or anatomic
in vulnerable populations, raising numerous
asplenia confers very high risk, particularly
concerns about further antimicrobial
in younger patients with sickle cell anemia;
Pneumococcal resistance, shifting serotype dominance, and
mortality from invasive pneumococcal
Vaccine Development: the efficacy of polysaccharide vaccine
disease in asplenic patients is more than A Historical Perspective preparations. In particular, elderly adults
50% (7, 8). Patients being treated for with higher rates of comorbid disease
underlying solid or hematologic S. pneumoniae was first discovered in the seemed to derive little benefit from the
malignancies have high rates of invasive late 19th century by U.S. Army physician 14-valent polysaccharide vaccine, with no
pneumococcal disease, although, George Sternberg and French scientist differences seen in rates of pneumococcal
interestingly, less than one-fifth of these Louis Pasteur, when it was recognized as pneumonia/bronchitis, all-cause
infections occur during periods of a major pathogenic cause of bacterial pneumonia, or overall mortality during a
neutropenia (9, 10). Antiretroviral therapy pneumonia (18). In 1902, German scientist follow-up period of almost 3 years (25). This
has significantly reduced the overall burden Friedrich Neufeld discovered that was attributed to the fact that more than
of invasive pneumococcal disease in antiserum containing different types of half of this susceptible patient population
individuals with HIV; however, the risk of S. pneumonia–specific antibodies caused did not mount or sustain adequate levels of
invasive pneumococcal disease remains a type-specific capsular swelling, or antibodies deemed to be protective against
35 times higher in HIV-infected individuals “Quellung reaction,” which allowed pneumococcal infection.
than in non–HIV-infected adults (11). identification of multiple pneumococcal
Independent of age, the presence of serotypes. Polysaccharides that were
other comorbid chronic conditions such as identified coursing along the exterior of the Immunologic Basis and
cardiovascular disease, chronic obstructive bacterium could be targeted for vaccine Host Response to
pulmonary disease (COPD), asthma, renal development. British physician Sir Almroth Pneumococcal Vaccines
insufficiency, and diabetes mellitus increases Wright conducted the first large clinical
the risk for invasive pneumococcal disease (9, trial of a whole-cell pneumococcal vaccine. S. pneumoniae is a complex bacterium
12). Patients with common pulmonary This trial was largely unsuccessful, bringing with 92 different polysaccharide capsular
conditions like COPD and asthma have vaccine development to a relative halt for serotypes identified to date (26). The
a two- to sixfold risk for invasive the next three decades (19). human airway uses numerous mechanisms
pneumococcal disease compared with the In 1945, Alexander Fleming, a former to protect from colonization and invasive
general population (9, 12). In addition, active aide of Wright, won a Nobel Prize for the pneumococcal infection. Innate immune
smoking confers increased risk, as do alcohol discovery of the antibacterial properties defenses, such as mucociliary escalator and
and intravenous drug use (9, 13–15). of penicillin. That same year, after a an array of pattern recognition receptors
934 AnnalsATS Volume 13 Number 6 | June 2016
FOCUSED REVIEWS
Table 1. Pneumococcal vaccine studies
Study Population Methods Primary Outcome Results Conclusions Other
MacLeod and 17,035 male army Tetravalent polysaccharide Vaccine-type PNA 84% RR reduction for Vaccine reduces Herd immunity
Hodges, recruits; aged vaccine (serotypes 1, 2, incidence vaccine-type PNA incidence of vaccine- conferred to the
1945 (20) 18–32 yr 5, 7) vs. placebo type pneumonia nonimmunized.
Riley et al., 11,958 healthy adults 14-valent polysaccharide PNA incidence 16% RR reduction Vaccination reduced
1977 (24) from Papua New vaccine (serotypes 1, 2, for all PNA (P . 0.05) all-cause mortality and
Guinea 3, 4, 5, 6, 7, 8, 12, 14, Overall mortality 21% RR reduction mortality due to
18, 23, 25, 46) vs. for all-cause mortality pneumonia
placebo (P , 0.05)
PNA mortality 43% RR reduction for
PNA-related mortality
(P , 0.05)
Simberkoff et al., 2,295 high-risk adults; 14-valent polysaccharide Overall mortality 24% RR increase Vaccination of “high-risk” High risk includes 11
1986 (25) mean age, 61 yr; vaccine vs. placebo Proven S. pneumoniae 100% RR increase subjects with PPSV14 of the following:
followed up for infections is not protective against .55 yr old; chronic
2.93 yr Probable S. pneumoniae 27% RR increase pneumococcal infections renal, hepatic,
infections cardiac, or pulmonary
Total S. pneumoniae 54% RR increase disease; alcoholism;
infections diabetes mellitus.
Shapiro et al., Case-control study; Case = confirmed (VE against VE (all patients) = 56% Vaccination reduces Vaccine was
1991 (60) 2,108 subjects; pneumococcal infection vaccine-type IPD (P , 0.00001) vaccine-type IPD not protective
mean age, 68 yr and indication for VE (immunocompetent) = infection against non–vaccine-type
vaccination. Control 61% (P , 0.00001) pneumococcal
subjects were matched VE (immune compromised) = infections. VE waned
for age and vaccine 21% (P = 0.48) as time from
indication vaccination increased
and with increasing
age of subject.
Black et al., 37,868 healthy infants; PCV7 vs. meningococcus Vaccine-type IPD VE = 97.4% (P , 0.001) Vaccination reduces IPD Non–vaccine-type
2000 (46) randomized to conjugated vaccine (fully vaccinated) in healthy infants infections were also
vaccination (series VE = 85.7% (P , 0.05) prevented by vaccine
of 4 immunizations); (partially vaccinated) (VE = 89.1%, P , 0.001).
follow up 3.5 yr Trial enrollment was
stopped early due to
high efficacy at the
interim analysis.
Black et al., 37,868 healthy infants; PCV7 vs. meningococcus Clinical PNA Vaccine effectiveness = Vaccination may prevent Vaccine effectiveness
2002 (61) randomized to conjugated vaccine 6.0% (P = 0.13) pneumonia in healthy calculated by Cox
vaccination (series PNA and X-ray Vaccine effectiveness = infants regression with the time
of 4 immunizations); performed 8.9% (P = 0.03) to first event as the
follow up 3.5 yr PNA and positive X-ray Vaccine effectiveness = primary outcome.
17.7% (P = 0.01) Intention to treat data
PNA and perihilar Vaccine effectiveness = shown.
infiltrate 11.1% (P = 0.35)
Jackson et al., Retrospective cohort Prior vaccination with Hospitalization due HR, 1.14 (95% CI, PPSV23 does not Influenza vaccination status
2003 (51) study; assessed PPSV23 vs. no prior to CAP 1.02–1.28) prevent pneumonia (in immunocompetent
47,365 outpatients vaccination “Outpatient” CAP HR, 1.04 (95% CI, but does reduce rates subjects) was the only
from Washington 0.96–1.13) of pneumococcal variable to be associated
State; all .65 yr old; Pneumococcal HR, 0.56 (95% CI, bacteremia with a statistically
followed up for 3 yr bacteremia 0.33–0.93) significant reduction in
the rate of death from
any cause.
French et al., 496 subjects (88% HIV PCV7 3 2 (given 4 wk Recurrent IPD HR, 0.31 (95% CI, PCV7 is protective HRs were adjusted for age,
2010 (68) infected) with previous apart) vs. placebo 0.11–0.84) against recurrent IPD sex, viral load, CD41 cell
IPD; follow up 4.5 yr in HIV-infected count. There was no
subjects change in mortality in
non–vaccine-type IPD.
Jackson et al., 835 healthy adults PCV13 vs. PPSV23 Antipneumococcal OPA titers were higher PCV13 shows a higher OPA titers have not been
2013 (66) with no prior OPA titers at 1 mo for 8 of 12 common immune response at directly shown to protect
pneumococcal and 1 yr serotypes, 1 mo 1 mo compared with from pneumococcal
vaccination; age, postvaccination postvaccination. Titers PPSV23 infection.
60–64 yr decreased at 1 yr but
remained higher than
baseline.
Jackson et al., 936 adults; age . 70 yr; PCV13 3 2 (1 yr apart) OPA titers at 1 mo after OPA titers were higher in With prior PPSV23 OPA titers have not been
2013 (67) previously received versus PPSV23 each vaccination the PCV13 group for 10 vaccination, PCV13 is directly shown to protect
PPSV23 .5 yr earlier followed by PCV13 of 12 common serotypes more immunogenic from pneumococcal
1 year later at 1 mo post initial than PPSV23 infection.
vaccination. OPA titers
were higher in the PCV13
group for 11 of 12
common serotypes at
1 mo post second
vaccination.
Bonten et al., 84,496 healthy adults; PCV13 vs. placebo Prevention of VE = 37.7% (P = 0.006) PCV13 is effective in Secondary outcomes that
2015 (69) .65 yr old; no prior vaccine-type CAP preventing vaccine- were also statistically
pneumococcal type CAP in older, significant include: IPD,
vaccination; healthy patients bacteremic and
follow up 4 yr nonbacteremic CAP.
Importantly, there was
no difference in mortality
and no difference in CAP
from all causes.
Definition of abbreviations: CAP = community-acquired pneumonia; CI = confidence interval; HR = hazard ratio; IPD = invasive pneumonococcal disease; OPA =
opsonophagocytic activity; PNA = pneumonia; RR = relative risk; S. pneumoniae = Streptococcus pneumoniae; VE = vaccine efficacy.
Focused Reviews 935
FOCUSED REVIEWS
Polysaccharide
A Pneumococcal
Surface protein
B
IgG2, IgM
Differentiation • Antibody production
Cell wall C-
polysaccharide B cell Plasma cell
Carrier protein
Capsular Polysaccharide
polysaccharide
IgG1, IgG3
Differentiation • Antibody production
B cell
Neuraminidase
MHC
Co-stimulatory
TCR molecules Polysaccharide-specific
plasma cell
Pneumolysin IgA protease
Autolysin
IL-4, IL-5, IL-13 Polysaccharide-
Carrier-peptide specific memory
specific T helper cell B cell
• Memory Response
Humoral Immunity
Clearance of extracellular pathogen
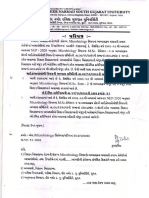
Figure 1. (A) Pneumococcus bacteria and virulence factors including capsular polysaccharide. (B) Immune response to polysaccharide and protein-
polysaccharide conjugate vaccines. MHC = major histocompatibility complex; TCR = T cell receptor. Adapted by permission from Reference 48.
that recognize bacterial proteins, help with on innate immune defenses that stimulate With vaccination, B-cell responses are
the initial protection against the bacteria the recruitment of polymorphonuclear cells. induced by vaccine antigen to produce
(27, 28). The antiphagocytic bacterial This response initially involves phagocytosis antibodies that can bind to the bacteria. It is
capsule is considered to be the most and intracellular killing by resident alveolar the acquired humoral immunity against
important determinant of pneumococcal macrophages, followed by infiltration of the bacterial capsule that is central to
virulence and is important for colonization neutrophil granulocytes into infected lungs. vaccination strategies against pneumococcal
of the nasopharynx (29–31) (Figure 1). Studies in innate immunity have shed pneumonia (34, 42). Immunologic
Pneumococcal cell wall fragments and light on the importance of complement, protection is mediated through
capsular polysaccharides are recognized surfactant proteins, antimicrobial peptides, opsonophagocytic antibodies directed
by antibodies that bind and activate the and several classes of pattern recognition against bacterial capsular polysaccharides
complement system (32). All pneumococci receptors that recognize pathogen- that define the pneumococcal serotypes and
serotypes can establish a carrier state and associated molecular patterns and bacterial serve as virulence factors (43). Cell-
colonize in the human nasopharynx during virulence factors on the pneumococci, mediated response (in the form of T-cell
the first few months of life. Children are which include the antiphagocytic help and cytokine production) is needed to
the main reservoir, with colonization rates polysaccharide capsule (27, 32, 34–39). augment the humoral B-cell response to
of up to 50%. Other important bacterial determinants generate optimal robust and longer-lasting
The ability of pneumococci to move include the pili, various adhesions, and antipneumococcal protective antibody
to another body site is limited to 20 of toxins, including pneumolysin and response. Once a humoral response has
the 92 serotypes (33). Moreover, the autolysin (40). The innate immune been generated, either in the setting of
development of symptoms of disease in the response helps trigger subsequent acquired vaccination or with previous infection, the
host involves the interactions between humoral and cellular responses. antipneumococcal antibodies contribute
multiple bacterial virulence determinants Humoral response is important to help to a more immediate and effective
and the host immune response. Typically, it eradicate the bacteria during primary neutralization of the bacteria.
is the very young and very old individuals infection, although these responses are not The development of pneumococcal
who are most susceptible to systemic as robust during primary infection. polysaccharide vaccines for adults and the
infection, as an effective immune response Anticapsular polysaccharide antibodies are efficacy of pneumococcal polysaccharide-
to S. pneumoniae relies on both innate and believed to represent the single most protein conjugate vaccines in infants and
adaptive cellular components of the important protective mechanism against children have confirmed that antibodies
immune system. invasive disease. In fact, antibodies to to polysaccharide antigens can provide
The host immune response to pneumococcal polysaccharides were excellent protection against invasive disease
pneumococcal lung disease is often the basis of serum therapy in which caused by pneumococci of the same serotype
characterized as intense and inflammatory passively transferred, serotype-specific as well as that caused by cross-reacting
in nature. In the unvaccinated population, antipneumococcal serum was shown to serotypes (44–46).
and in the absence of preexisting serotype- reduce mortality from pneumococcal Capsular polysaccharide antigens elicit
specific antibodies, the infected host relies pneumonia by half (41). antibodies that are isotype restricted to IgM
936 AnnalsATS Volume 13 Number 6 | June 2016
FOCUSED REVIEWS
and IgG2 and, to a lesser extent, IgG1. These costimulatory signals, the triggering is an immediate and essential precursor for
IgM responses are typically short lived, and of carrier-peptide–specific T cells results in pneumococcal disease and the source of
the IgG2 responses from polysaccharides are T-cell help, with the production of both transmission between individuals (54). The
weak compared with what is induced by plasma cells and memory B cells. This pneumococcal nasopharyngeal carriage rate
conjugate-based vaccines that are typically allows for enhanced immunogenicity with a is age dependent, starting early in the first
dominated by IgG1 subclasses that bind to more rapid and robust production of year of life and peaking at 55% around
complement better and are of higher affinity antibodies and the establishment of T-cell– 3 years of age, with a steady decline into
(47). Early pneumococcal vaccines were dependent immunological memory (48). adulthood.
based on the use of capsular This process stimulates good antibody The protective herd effect of the vaccine
polysaccharides that induced type-specific response, mucosal immunity, and is hypothesized to be a direct consequence of
antibodies that activated and fixed immunologic memory and systemic the reduction in nasopharyngeal carriage of
complement, promoting bacterial anamnestic IgG response in all children and vaccine-type strains in immunized children,
opsonization and phagocytosis. Antibodies adults. with subsequent interruption of
to pneumococcus are also believed to Polysaccharide-based vaccines have transmission to their nonimmunized
represent the primary mechanism of been shown to result in decreased memory contacts (55). The presumed mechanism of
naturally acquired resistance to B-cell frequency, whereas conjugate protein- herd immunity has been attributed to
colonization. Appropriately triggered B based vaccines increase serotype-specific mucosal IgA antibodies or serum
cells also release IgA, which is deposited memory B-cell responses, highlighting that antibodies that leak into the mucosa to alter
on mucosal surfaces to protect against these vaccines induce important T-cell– and decrease the bacterial population in the
pneumococcal colonization. dependent memory responses (49). nasopharynx (56).
Vaccines composed of purified Given the importance of cellular T- and As a result, the elderly have indirectly
capsular polysaccharides, which have been B-cell function in eliciting an effective and benefited considerably from the
available for more than 50 years, are not protective anticapsular antibody response, introduction of conjugate vaccines in
immunogenic in young children and the patients with impaired immune systems, pediatric population. Deaths and
elderly. Moreover, capsular polysaccharides such as those with HIV infection, splenic hospitalizations related to pneumonia have
do not yield an anamnestic response, despite dysfunction, cancer, solid-organ all decreased substantially with reduction in
multiple exposures, so that antibody titers transplantation, or iatrogenic invasive pneumococcal disease and
do not boost beyond their original level after immunosuppressive medications, are highly nonbacteremic pneumococcal pneumonia
primary immunization. This is due to the at risk for invasive pneumococcal infections. among adults 65 years of age or older,
inability of polysaccharides to recruit The polysaccharide vaccine has been widely comparing prevaccination and
cognate CD41 T-cell help through T-cell evaluated in these populations, but due to its postvaccination eras (57). Even though herd
receptor recognition of peptide–major low immunogenicity, its efficacy has been immunity limits the transmission of the
histocompatibility complex class II on the suboptimal or even absent (50–52). Age- bacteria, populations at risk, including
surface of antigen-presenting cells. related immunosenescence mechanisms in the elderly and the immunosuppressed,
However, the regularly spaced elderly people have been described to do not intrinsically mount excellent
repeating epitopes expressed by explain the increased susceptibility of the antipneumococcal responses. There is still a
polysaccharides induce multivalent aging population to pneumococcus (37). In need to achieve a more effective direct
membrane immunoglobulin cross-linking these populations, the conjugate vaccine vaccination in the adult population.
on the B-cell surface. This immunological should provide improved immunogenicity;
crosslinking on the B-cell surface by however, there is a paucity of evidence
polysaccharide repeating epitopes mediates surrounding the clinical efficacy of Pneumococcal Vaccination in
improved B-cell proliferative responses; conjugate pneumococcal vaccines in adults the Modern Age
however, on its own, and without proper with varying immunocompromising
T-cell help and cytokine signaling, this conditions (50). PPSV23
immunological crosslinking does not induce In 1983, the 23-valent polysaccharide
good memory response, which leads to vaccine (PPSV23) was approved for use in
decreased and suboptimal subsequent Herd Effect the United States (Figure 2) for adults and
immune responses. children older than 2 years of age. This new
The lack of anamnestic response by Individuals who are otherwise personally formulation was developed after worldwide
capsular polysaccharide can be overcome by vulnerable to pneumococcal infection derive surveillance showed a high frequency of
the use of conjugate vaccines that elicit more protection from the presence of herd pneumococcal bacteremia and meningitis
of an IgG1 (and IgG3) response to immunity in the immunocompetent by serotypes not covered in the previous
polysaccharide and produce a stronger population. The maintenance of indirect (or 14-valent vaccine (58). Use of PPSV23 has
immune response because polysaccharides herd) immunity depends on the sustained repeatedly been shown to provide a
coexpressed with carrier proteins interact ability of the immune response to significant reduction in the rates of invasive
better with major histocompatibility prevent acquisition of the bacteria by pneumococcal disease, however, sadly,
complex and mediate cognate CD41 T-cell individuals in the population who are without impact on overall mortality or
help for polysaccharide-specific B-cell transmitters (53). There is strong evidence in overall rates of pneumonia (59).
activation. In the context of appropriate that pneumococcal nasopharyngeal carriage Historically, rates of pneumococcal
Focused Reviews 937
FOCUSED REVIEWS
although rates of vaccine-type invasive
PCV7 PCV13 pneumococcal disease, pneumonia, and
otitis media were decreasing, rates of
disease from nonvaccine serotypes were
6A becoming more common. A large
retrospective cohort study identified more
than 30,000 cases of invasive pneumococcal
4, 6B, 9V, disease over a 9-year time period (64).
14, 18C, There was a reduction in overall and PCV7-
19F, 23F type invasive pneumococcal disease of
1, 3, 5, 45 and 94%, respectively.
7F, 19A
A study of a pediatric population
showed that only 15% of identified invasive
pneumococcal disease infections were caused
2, 8, 9N, 10A, 11A, 12F, by PCV7 serotypes. The study also showed,
15B, 17F, 20, 22F, 33F however, a stable overall rate of invasive
pneumococcal disease in this population when
compared with pre-PCV7 data, suggesting no
PPSV23 change in overall disease burden (65).
In June 2012, the U.S. Food and Drug
Figure 2. Pneumococcal serotypes in vaccines.
Administration approved PCV13 for all
adults older than 50 years, for the
prevention of pneumonia and invasive
meningitis have been too low for The biggest differences were seen in the pneumococcal disease. Much of this
determination of vaccination efficacy and very young (,2 yr old, decrease by 64%) recommendation was supported by
do not factor largely into published data, and the elderly (.65 yr old, decrease by evidence from immunogenicity trials in
even in metaanalysis; thus, the majority of 54%) (62). which more than 800 vaccine-naive
the measured benefit is seen in cases of The effect of herd immunity was seen in subjects aged 60 to 64 years old were
bacteremic pneumococcal pneumonia. years to follow, with rates of pneumococcal randomized to receive one dose of either
As previously discussed, disease decreasing in older patients who PCV13 or PPSV23 (66). The primary
immunocompromised individuals are had never received conjugated vaccine, often outcome was 1-month postvaccination
significantly less likely to benefit from by significant magnitude (45). In a 10-year opsonophagocytic activity (OPA) titers
vaccination when compared with study after routine PCV7 vaccination of that are believed, but not proven, to be
immunocompetent individuals, borne out infants, reduction in the rates of invasive associated with in vivo protection from
by studies of clinical infection rates (60). pneumococcal disease and pneumococcal pneumococcal infection. At 1 month,
Moreover, even in patients without frank pneumonia were shown in all age subjects given PCV13 had increased OPA
immunocompromise, vaccine efficacy groups (57), with drastic reductions in titers compared with the subjects given
degrades with age. For example, the vaccine nonbacteremic pneumococcal pneumonia in PPSV23, specifically for the shared
efficacy of an immune-competent 80-year- infants (47%) and adults 65 years and older serotypes between the two vaccines.
old man is 67% within 3 years of being (54%). Prevention of at least 750,000 Titers were shown to decrease at 1 year
vaccinated; more than 5 years after hospitalizations over a 6-year period was postvaccination, although they still remained
vaccination, the same man has a vaccine attributed to the PCV7 vaccine, primarily higher than prevaccination levels.
efficacy of only 32%. from herd protection in adult populations. A A similar study was performed looking
study in South Africa similarly showed a at the effect of PCV13 (vs. PPSV23) on
PCV7 decrease in invasive pneumococcal disease subjects older than 70 years who were
Conjugated vaccinations had been rates in children and adults after pediatric previously vaccinated with PPSV23 more
developed previously for prevention of vaccination with PCV7 (63). than 5 years earlier (67). OPA titers were
Haemophilus and Meningococcus higher in the PCV13 “boosted” group for
infections with good efficacy, which led to PCV13 10 of 12 serotypes common to the two
the development and approval of a seven- Figure 2 shows the serotypes that were vaccines, implying that a patient’s
valent conjugated vaccine in 2000 for included in the development of PCV13 immunity against pneumococcal infection
pediatric use. In large prospective trials, (seven serotypes from PCV7, five that were could be enhanced with a combined
the conjugated vaccine was shown not in PPSV23, and one previously uncovered strategy of polysaccharide vaccination
only to reduce pneumococcal bacteremia serotype). In February 2010, the U.S. Food followed by conjugate vaccine, particularly
(46) but also to decrease the risk of otitis and Drug Administration approved PCV13 in the face of waning immunity.
media and pneumonia (61). A population- for use in children 6 weeks to 71 months In June 2012, PCV13 was recommended
based survey between 1998 and 2005 was old, for the prevention of invasive by the Advisory Committee on Immunization
able to demonstrate a 30% decrease in the pneumococcal disease and otitis media. Practices (ACIP) for adults older than
incidence of pneumococcal meningitis. Data from the post-PCV7 era showed that 18 years with immune-compromising
938 AnnalsATS Volume 13 Number 6 | June 2016
FOCUSED REVIEWS
conditions. This recommendation was Table 2. Pneumococcal disease risk assessment
based largely on a 2010 randomized
controlled trial that studied the secondary Immunocompetent individuals Chronic heart disease (with exception of isolated
prevention of invasive pneumococcal with high-risk comorbidities hypertension)
disease in nearly 500 subjects, most of Chronic lung disease
whom had HIV (68). In this population, Diabetes mellitus
Chronic liver disease or cirrhosis
two doses of PCV7 resulted in a Smoking
significant decrease in the rate of Alcoholism
recurrent invasive pneumococcal disease Cerebrospinal fluid leak
over 5 years. Cochlear implants
As of August 2014, the ACIP has Functional or anatomical asplenia Sickle cell disease and other hemoglobinopathies
Congenital or acquired asplenia/splenic
recommended the routine use of PCV13, in dysfunction
series with PPSV23, for all patients 65 years Immunosuppressed individuals HIV
and older. The Community Acquired Chronic renal failure and nephrotic syndrome
Pneumonia Immunization Trial in Adults Immunosuppressant diseases and/or associated
immunosuppressant drugs or radiation therapy
(CAPiTA) study, conducted between 2008 (malignant neoplasms, leukemias, lymphomas,
and 2010, randomized 85,000 Dutch solid organ transplants)
subjects 65 years and older to receive one Congenital immunodeficiencies (B- or T-cell
dose of PCV13 or placebo (69). The subjects deficiencies, complement deficiencies,
had never been vaccinated and were phagocytic disorders)
otherwise immune competent. It is
important to note that in the CAPiTA
PCV7-based regimens over to the current pneumococcal infection in adults and
cohort, 12% of subjects were current
PCV13-based regimens (70). impact vaccination recommendations
smokers, and 10% reported a known
between ages 19 and 65 years (Table 2).
diagnosis of chronic lung disease. They
Special Pediatric Scenarios Those with otherwise intact immunity but
used a serotype-specific urinary antigen
with high-risk comorbid conditions should
assay to differentiate vaccine-type and
1. For children aged 6 to 18 years who receive a dose of PPSV23 at the earliest
non–vaccine-type infections. After a mean
previously completed an appropriate relevant opportunity. Notably, this includes
follow up of 4 years, the vaccinated group
vaccination regimen with either PCV7 active smokers, irrespective of presence of
developed 49 episodes of vaccine-type
or PPSV23, and who are at higher risk lung disease. Their subsequent vaccine
confirmed community-acquired
of pneumococcal infection, a one-time schedule would otherwise follow that for
pneumonia compared with 90 episodes
dose of PCV13 can be administered. the adult population.
in the placebo group, representing 45%
2. For children aged 2 to 18 years who Those with immunocompromising
vaccine efficacy. There were also significant
previously completed an appropriate conditions, such as acquired or functional
decreases in the rates of invasive
vaccination regimen with PCV13, and asplenia, congenital or acquired
pneumococcal disease and confirmed
who are at higher risk of pneumococcal immunosuppression, chronic renal failure,
noninvasive community-acquired pneumonia
infection, a dose of PPSV23 can be given nephrotic syndrome, or underlying
(P = 0.007). For invasive pneumococcal
at age 2 years, at least 8 weeks after last malignancy, should also first receive PCV13,
disease, vaccine efficacy was 75%.
dose of PCV13. followed by PPSV23 8 weeks later, but
3. For those children with specific high- should also receive a second PPSV23 5 years
risk conditions (functional or anatomic after the initial PPSV23 dose. Once again, if
Current Recommendations for asplenia, sickle cell disease, HIV, other PPSV23 has been given first, PCV13 may
Pneumococcal Vaccination immunocompromised conditions; see still be given 1 year after the initial PSV23,
Table 2), an additional PPSV23 one- with the second PPSV23 still occurring
For the clinician, there are multiple branch time booster can be given 5 years later 5 years after the initial vaccination. All
points to consider when approaching than the initial PPSV23 vaccine. individuals should receive an additional
pneumococcal vaccination of an individual dose of PPSV23 at age 65 years, provided
patient. Here, we will first consider age it has been 5 years since the last dose.
Adult Population
groups, followed by vaccination status, then Immunocompetent individuals with either
Many individuals will have received
clinical risk factors (Table 2). cochlear implants or cerebrospinal fluid leak
pneumococcal vaccination at some point
prior as an adult (age 19 years or older), follow a similar schedule.
Pediatric Population requiring a more complex algorithm to be Otherwise, vaccine-naive individuals
The ACIP currently recommends routine discussed below, but in the case of truly should receive one dose of the PCV13
vaccination for children aged 2 to 59 months vaccine-naive individuals, the vaccine vaccine at age 65 years (or older, if none
with PCV13 as a four-dose series (at age 2, 4, 6, schedule is again predicated on age and prior) followed by one dose of the PPSV23
and 12–15 mo) (Figure 3). There are comorbid conditions (Figure 4) (71). As vaccine 6 to 12 months later. The minimum
resources available to assist with phasing with the pediatric population, there are interval between the two vaccines should be
non–vaccine-naive patients from primarily comorbid conditions that increase risk for 8 weeks, and the PPSV23 vaccine can be
Focused Reviews 939
FOCUSED REVIEWS
Give PPSV23
at 2y
(8 wks after last
Give PCV13 Yes dose of PCV13)
at 2, 4, 6, and High risk?*
12–15 months
No
No action Give one time
No
booster
Prior complete of PPSV23
pneumococcal 5y after last
vaccine series PPSV23
Yes
with PCV7 or Very
Give PCV13
PPSV23? high
Yes between
age 6–18y risk?†
Yes
No
High risk?*
No action
No
No action
Figure 3. Advisory Committee on Immunization Practices recommendations for pediatric pneumococcal vaccination. *See Table 2 for relevant high-risk
comorbidities and immunocompromised conditions. †Functional or anatomic asplenia and immunocompromised conditions. Adapted from CDC
guidelines for appropriate overlap schedules for individuals who received partial series of PCV7 and/or PPSV23 (70).
given more than 12 months beyond the 6- to It is important to note that current secondary response to a polysaccharide
12-month interval if this window is missed. ACIP guidelines recommend very specific vaccine. However, a randomized trial that
However, many individuals will already intervals between both types of vaccines. administered polysaccharide vaccine in the
have received one, if not more, doses of Because conjugate vaccines stimulate first 6 months before the PCV7 conjugate
PPSV23 in adulthood. In this case, timing memory B cells, it was believed that vaccine resulted in attenuated antibody
and sequence of PCV13 and any subsequent administration of conjugate vaccine should concentration compared with PCV7
PPSV23 must be more deliberate (Figure 5). prime the immune system for an improved alone (72).
Give
PPSV23
Give Yes booster Give
Give PPSV23 5yrs later PPSV23
Cochlear implant
PCV13 8wks at age 65y,
or CSF leak?
later 5yrs after
Yes No last PPSV23
Age High
19–64y risk?*
No
Give PPSV23
Medium Give Give PSV13
1y after PCV13 and
risk?† PPSV23 at age 65y
5y after last PPSV23
Age
Give PCV 13 Give PPSV231y later
65y
Figure 4. Advisory Committee on Immunization Practices recommendations for adult pneumococcal vaccination: vaccine-naive individuals. *Includes
patients with functional/anatomic asplenia, immunocompromising conditions, cerebrospinal fluid (CSF) leak, or cochlear implants (see Table 2). †Includes
patients with normal immunity but certain comorbid conditions.
940 AnnalsATS Volume 13 Number 6 | June 2016
FOCUSED REVIEWS
Give
PPSV23
Yes booster
Give PCV13 5yrs later Give PPSV23
1 year after Cochlear implant at age 65y,
PPSV23 or CSF leak? 5yrs after
No last PPSV23
Yes
Age
High risk?*
19–64y
No
Give PPSV23
Give PCV13 at age
1y after PCV13,
65y, 1y after
5yrs after last PPSV23
PPSV23
Give PPSV23
Give PCV 13
Age 65y 1y after PCV13 and
1y after PPSV23
5y after PPSV23
Figure 5. Advisory Committee on Immunization Practices recommendations for adult pneumococcal vaccination: individuals with prior PPSV23
vaccination. *Includes patients with functional/anatomic asplenia, immunocompromising conditions, cerebrospinal fluid (CSF) leak, or cochlear implants
(see Table 2).
Although several smaller earlier 1 year before receiving PCV13. More the elderly population was the robust
studies did not show that priming with investigations are needed to determine immunogenicity data in this population.
pneumococcal conjugate vaccine followed the clinical implications of frequent This fact, in conjunction with clinical
by polysaccharide vaccine enhanced vaccinations. trial results in immunocompromised
immunogenicity, more recent larger studies populations, was the foundation for the
showed improved response (72–74). These present substantial shift in adult
larger studies using PCV13 conjugate Discussion and immunization practice. Although this
vaccine followed a year later by the Future Directions strategy appears to be well supported by the
polysaccharide-based PPSV23 resulted in compelling results observed in CAPiTA,
higher antibody activities after a month of Over the past 100 years, substantial progress with 45% efficacy in prevention of
PPSV23 administration, but at 6 months has been made in the prevention of community-acquired pneumonia and 75%
the antibody levels in booster recipients fall invasive pneumococcal disease. Current efficacy in prevention of invasive
to baseline (66, 75). recommendations reflect a series of changes pneumococcal disease, there are some
Although polysaccharide made over a relatively short span of time, on caveats to consider.
vaccines do not necessarily trigger the basis of growing data and experience First, this study does not represent a
anamnestic responses, revaccination with both polysaccharide and conjugate true test of the current ACIP guidelines or
with polysaccharide vaccines at the vaccines in multiple different populations. comparison to prior recommended practice
proper interval can result in sustained With so many nearly simultaneous changes with PPSV23, as subjects were vaccine naive,
antipneumococcal antibody titers, especially in vaccine strategy, it remains a challenge to and subjects received either PCV13 or
in middle-aged and older adults (76, 77). appropriately attribute the source of greatest placebo. Moreover, results may in part
There are studies to suggest that there is an effect. It is clear that prior PCV7 vaccination reflect herd-immunity impact of pediatric
inverse relationship between circulating strategies in children over the past 2 decades vaccination practices in the Netherlands,
antibodies before revaccination and the yielded substantial indirect impacts on first with PCV7, then with PCV10. Finally,
subsequent increase in antibody titers (78). the prevalence of adult vaccine-type the population studied was predominantly
However, there is also a suggestion that pneumococcal disease, and therefore the white, and most patients were 65 to 75 years
revaccination too soon after initial switchover to preferential use of PCV13 in of age. As the average life expectancy
vaccination could be detrimental. Because the pediatric population may be expected to continues to increase, we will need to confer
of these findings, ACIP recommend yield more of the same, although that vaccine efficacy to an ever-aging population
PCV13 first, followed by a minimum of remains to be proven. for whom vaccine efficacy is known to wane
8 weeks before the PPSV23. For those who At this point, we are still inferring over time (51, 60). A study in a more
already have received PPSV23, current future benefits from data presently available. heterogeneous elderly population with
recommendations advocate waiting The original impetus for use of PCV13 in more long-term follow up of vaccine titers
Focused Reviews 941
FOCUSED REVIEWS
would be instructive, as concern remains colonization, or should the goal be and lower cost, the use of common
about waning immunity in the elderly as preventing bacterial invasion, leaving pneumococcal proteins for broader
they move decades (or more) beyond last colonization unaffected to avoid selective coverage, and the use of immune
vaccination. colonization with more virulent organisms? adjuvants to improve mucosal and
Although expanded serologic coverage These facts underline the key role for systemic immunity. Monitoring changes
makes intuitive sense, particularly for an pneumococcal colonization in pathogenesis in the distribution of serotypes causing
aging and immunologically vulnerable and prevention of pneumococcal infections, pneumococcal disease among children and
population, it is unclear whether any further which justifies extensive consideration in adults should inform formulations of
changes to vaccination protocol could decision making about mass vaccination future higher-valent conjugate vaccines.
outstrip the benefits of comprehensive and future vaccine strategies. Certainly, Approaches that rely on targeting common
measures to improve immunization without complete eradication of proteins independent of serotypes,
adherence in both the pediatric and adult pneumococcal carriage, the immunological inactivated and live attenuated whole-cell
populations. With the use of two different pressure will ultimately select for vaccines, DNA vaccines and genetic
vaccines administered under very specific noncovered bacterial serotypes, but engineering of glycoproteins to develop
schedules, implementation may prove to be will these serotypes cause invasive glycoconjugates hold the promise to
a difficult task in the real world. It will be pneumococcal disease (79)? confer broader serotype-independent
important to monitor immunization There is also a role for controlling drug- protection against pneumococcal
adherence as this combination strategy resistant bacteria with judicious use of disease. (80).
moves into general practice and to antibiotics. The rapid increase in antibiotic Close scrutiny of the changing
determine if these vaccines are indeed being resistance, high cost, and limited serotype epidemiology of invasive pneumococcal
administered as intended to most patients. coverage of the currently available disease and pneumonia will be required
More study is needed to see how effectively pneumococcal vaccines will likely require to evaluate the effectiveness and the
(and cost-effectively) these new the need for novel vaccine candidates that continued utility of the current vaccination
pneumococcal vaccination strategies can be are more affordable and elicit protection strategy and the future directions for
applied in populations that differ in age, sex, against a broader range of pneumococcal pneumococcal disease prevention among
socioeconomic status, race, comorbidities, strains. Moreover, efforts are needed for older adults. n
access to care, and immunologic status. next-generation vaccine development that
Finally, is eradication of invasive has longer-lasting immunity effects with Author disclosures are available with the text
pneumococcal disease an attainable goal? broader serotype coverage that work well in of this article at www.atsjournals.org.
For this to take place, there are several the aging population.
questions that need to be addressed. Should Efforts in this area include Acknowledgment: The authors thank Susan
the aim of pneumococcal disease prevention optimization of cultivation conditions for Ardito and Dr. Geoffrey Connors for their editorial
be eradication of nasopharyngeal bacteria capsule production for better yield assistance and review of the manuscript.
References before and after the introduction of the pneumococcal conjugate
vaccine. Clin Infect Dis 2007;44:1428–1433.
1 Atkinson W, Wolfe C, Hamborsky J, editors. Epidemiology and 9 Kyaw MH, Rose CE Jr, Fry AM, Singleton JA, Moore Z, Zell ER, Whitney
prevention of vaccine-preventable diseases, 12th ed. Washington CG; Active Bacterial Core Surveillance Program of the Emerging
DC: Public Health Foundation; 2012. Infections Program Network. The influence of chronic illnesses on
2 Huang SS, Johnson KM, Ray GT, Wroe P, Lieu TA, Moore MR, Zell ER, the incidence of invasive pneumococcal disease in adults. J Infect
Linder JA, Grijalva CG, Metlay JP, et al. Healthcare utilization and Dis 2005;192:377–386.
cost of pneumococcal disease in the United States. Vaccine 2011; 10 Kumashi P, Girgawy E, Tarrand JJ, Rolston KV, Raad II, Safdar A.
29:3398–3412. Streptococcus pneumoniae bacteremia in patients with cancer:
3 Austrian R. The pneumococcus at the millennium: not down, not out. disease characteristics and outcomes in the era of escalating drug
J Infect Dis 1999;179:S338–S341. resistance (1998-2002). Medicine (Baltimore) 2005;84:303–312.
4 Centers for Disease Control and Prevention. Active Bacterial Core 11 Heffernan RT, Barrett NL, Gallagher KM, Hadler JL, Harrison LH,
Surveillance (ABCs) report Emerging Infections Program Network Reingold AL, Khoshnood K, Holford TR, Schuchat A. Declining
Streptococcus pneumoniae; 2013 [accessed 2013 Dec 6]. Available incidence of invasive Streptococcus pneumoniae infections among
from: http://www.cdc.gov/abcs/reports-findings/survreports/ persons with AIDS in an era of highly active antiretroviral therapy,
1995-2000. J Infect Dis 2005;191:2038–2045.
spneu12.pdf
12 Talbot TR, Hartert TV, Mitchel E, Halasa NB, Arbogast PG, Poehling
5 van der Hoek W, Wielders CC, Schimmer B, Wegdam-Blans MC,
KA, Schaffner W, Craig AS, Griffin MR. Asthma as a risk factor
Meekelenkamp J, Zaaijer HL, Schneeberger PM. Detection of phase I
for invasive pneumococcal disease. N Engl J Med 2005;352:
IgG antibodies to Coxiella burnetii with EIA as a screening test for 2082–2090.
blood donations. Eur J Clin Microbiol Infect Dis 2012;31:3207–3209. 13 Cruickshank HC, Jefferies JM, Clarke SC. Lifestyle risk factors for
6 Hjuler T, Poulsen G, Wohlfahrt J, Kaltoft M, Biggar RJ, Melbye M. invasive pneumococcal disease: a systematic review. BMJ Open
Genetic susceptibility to severe infection in families with invasive 2014;4:e005224.
pneumococcal disease. Am J Epidemiol 2008;167:814–819. 14 Taylor SN, Sanders CV. Unusual manifestations of invasive
7 Bisharat N, Omari H, Lavi I, Raz R. Risk of infection and death among pneumococcal infection. Am J Med 1999;107:12S–27S.
post-splenectomy patients. J Infect 2001;43:182–186. 15 Harboe ZB, Larsen MV, Ladelund S, Kronborg G, Konradsen HB,
8 Halasa NB, Shankar SM, Talbot TR, Arbogast PG, Mitchel EF, Wang Gerstoft J, Larsen CS, Pedersen C, Pedersen G, Obel N, et al.
WC, Schaffner W, Craig AS, Griffin MR. Incidence of invasive Incidence and risk factors for invasive pneumococcal disease in HIV-
pneumococcal disease among individuals with sickle cell disease infected and non-HIV-infected individuals before and after the
942 AnnalsATS Volume 13 Number 6 | June 2016
FOCUSED REVIEWS
introduction of combination antiretroviral therapy: persistent high risk Streptococcus pneumoniae. Infect Immun 2011;79:4210–4217.
among HIV-infected injecting drug users. Clin Infect Dis 2014;59: 37 Krone CL, van de Groep K, Trzciński K, Sanders EA, Bogaert D.
1168–1176. Immunosenescence and pneumococcal disease: an imbalance in
16 Torres A, Blasi F, Dartois N, Akova M. Which individuals are at host-pathogen interactions. Lancet Respir Med 2014;2:141–153.
increased risk of pneumococcal disease and why? Impact of COPD, 38 Paterson GK, Orihuela CJ. Pneumococci: immunology of the innate
asthma, smoking, diabetes, and/or chronic heart disease on host response. Respirology 2010;15:1057–1063.
community-acquired pneumonia and invasive pneumococcal 39 Koppe U, Suttorp N, Opitz B. Recognition of Streptococcus
disease. Thorax 2015;70:984–989. pneumoniae by the innate immune system. Cell Microbiol 2012;14:
17 Kew KM, Seniukovich A. Inhaled steroids and risk of pneumonia for 460–466.
chronic obstructive pulmonary disease. Cochrane Database Syst Rev 40 Steel HC, Cockeran R, Anderson R, Feldman C. Overview of
2014;3:CD010115. community-acquired pneumonia and the role of inflammatory
18 Welch W. The Micrococcus lanceolatus, with especial reference to the mechanisms in the immunopathogenesis of severe pneumococcal
etiology of acute lobar pneumonia. Johns Hopkins Hospital Bulletin disease. Mediators Inflamm 2013;2013:490346.
1892;iii:125–139. 41 Lord F, Hefron R. Pneumonia and serum therapy. New York:
19 Wright A, Morgan W, Colebrook L, Dodgson R. Observation on Commonwealth Fund; 1938.
prophylactic inoculation against pneumococcus infections, and 42 Snapper CM. Mechanisms underlying in vivo polysaccharide-specific
on the results that have been achieved by it. Lancet 1914;10: immunoglobulin responses to intact extracellular bacteria. Ann N Y
87–95. Acad Sci 2012;1253:92–101.
20 MacLeod CM, Hodges RG. Prevention of pneumococcal pneumonia by 43 Kim JO, Romero-Steiner S, Sørensen UB, Blom J, Carvalho M,
immunization with specific capsular polysaccharides. J Exp Med Barnard S, Carlone G, Weiser JN. Relationship between cell
1945;82:445–465. surface carbohydrates and intrastrain variation on
21 Hansman D, Bullen M. A resistant pneumococcus. Lancet 1967;2: opsonophagocytosis of Streptococcus pneumoniae. Infect Immun
264–265. 1999;67:2327–2333.
22 Jacobs MR, Koornhof HJ, Robins-Browne RM, Stevenson CM, 44 Cornu C, Yzèbe D, Léophonte P, Gaillat J, Boissel JP, Cucherat M.
Vermaak ZA, Freiman I, Miller GB, Witcomb MA, Isaäcson M, Ward Efficacy of pneumococcal polysaccharide vaccine in
JI, et al. Emergence of multiply resistant pneumococci. N Engl J Med immunocompetent adults: a meta-analysis of randomized trials.
1978;299:735–740. Vaccine 2001;19:4780–4790.
23 Austrian R, Gold J. Pneumococcal bacteremia with especial reference 45 Whitney CG, Farley MM, Hadler J, Harrison LH, Bennett NM, Lynfield R,
to bacteremic pneumococcal pneumonia. Ann Intern Med 1964;60: Reingold A, Cieslak PR, Pilishvili T, Jackson D, et al.; Active Bacterial
759–776. Core Surveillance of the Emerging Infections Program Network.
24 Riley ID, Tarr PI, Andrews M, Pfeiffer M, Howard R, Challands P, Decline in invasive pneumococcal disease after the introduction of
Jennison G. Immunisation with a polyvalent pneumococcal vaccine: protein-polysaccharide conjugate vaccine. N Engl J Med 2003;348:
reduction of adult respiratory mortality in a New Guinea Highlands 1737–1746.
community. Lancet 1977;1:1338–1341. 46 Black S, Shinefield H, Fireman B, Lewis E, Ray P, Hansen JR, Elvin L,
25 Simberkoff MS, Cross AP, Al-Ibrahim M, Baltch AL, Geiseler PJ, Nadler Ensor KM, Hackell J, Siber G, et al.; Northern California Kaiser
J, Richmond AS, Smith RP, Schiffman G, Shepard DS, et al. Efficacy Permanente Vaccine Study Center Group. Efficacy, safety and
of pneumococcal vaccine in high-risk patients: results of a Veterans immunogenicity of heptavalent pneumococcal conjugate vaccine in
Administration Cooperative Study. N Engl J Med 1986;315: children. Pediatr Infect Dis J 2000;19:187–195.
1318–1327. 47 van der Poll T, Opal SM. Pathogenesis, treatment, and prevention of
26 Dockrell DH, Whyte MK, Mitchell TJ. Pneumococcal pneumonia: pneumococcal pneumonia. Lancet 2009;374:1543–1556.
mechanisms of infection and resolution. Chest 2012;142:482–491. 48 Pollard AJ, Perrett KP, Beverley PC. Maintaining protection against
27 Calbo E, Garau J. Factors affecting the development of systemic invasive bacteria with protein-polysaccharide conjugate vaccines.
inflammatory response syndrome in pneumococcal infections. Curr Nat Rev Immunol 2009;9:213–220.
Opin Infect Dis 2011;24:241–247. 49 Clutterbuck EA, Lazarus R, Yu LM, Bowman J, Bateman EA, Diggle L,
28 Calbo E, Garau J. Of mice and men: innate immunity in pneumococcal Angus B, Peto TE, Beverley PC, Mant D, et al. Pneumococcal
pneumonia. Int J Antimicrob Agents 2010;35:107–113. conjugate and plain polysaccharide vaccines have divergent
29 Magee AD, Yother J. Requirement for capsule in colonization by effects on antigen-specific B cells. J Infect Dis 2012;205:
Streptococcus pneumoniae. Infect Immun 2001;69:3755–3761. 1408–1416.
30 Weinberger DM, Trzciński K, Lu YJ, Bogaert D, Brandes A, Galagan J, 50 Cordonnier C, Averbuch D, Maury S, Engelhard D. Pneumococcal
Anderson PW, Malley R, Lipsitch M. Pneumococcal capsular immunization in immunocompromised hosts: where do we stand?
polysaccharide structure predicts serotype prevalence. Plos Pathog Expert Rev Vaccines 2014;13:59–74.
2009;5:e1000476. 51 Jackson LA, Neuzil KM, Yu O, Benson P, Barlow WE, Adams AL,
31 Jonsson S, Musher DM, Chapman A, Goree A, Lawrence EC. Hanson CA, Mahoney LD, Shay DK, Thompson WW; Vaccine Safety
Phagocytosis and killing of common bacterial pathogens of the lung Datalink. Effectiveness of pneumococcal polysaccharide vaccine in
by human alveolar macrophages. J Infect Dis 1985;152:4–13. older adults. N Engl J Med 2003;348:1747–1755.
32 Mitchell AM, Mitchell TJ. Streptococcus pneumoniae: virulence factors 52 Jackson ML, Neuzil KM, Thompson WW, Shay DK, Yu O, Hanson CA,
and variation. Clin Microbiol Infect 2010;16:411–418. Jackson LA. The burden of community-acquired pneumonia in
33 Robinson KA, Baughman W, Rothrock G, Barrett NL, Pass M, Lexau C, seniors: results of a population-based study. Clin Infect Dis 2004;39:
Damaske B, Stefonek K, Barnes B, Patterson J, et al.; Active 1642–1650.
Bacterial Core Surveillance (ABCs)/Emerging Infections Program 53 Rashid H, Khandaker G, Booy R. Vaccination and herd immunity: what
Network. Epidemiology of invasive Streptococcus pneumoniae more do we know? Curr Opin Infect Dis 2012;25:243–249.
infections in the United States, 1995-1998: opportunities for 54 Weinberger DM, Dagan R, Givon-Lavi N, Regev-Yochay G, Malley R,
prevention in the conjugate vaccine era. JAMA 2001;285: Lipsitch M. Epidemiologic evidence for serotype-specific acquired
1729–1735. immunity to pneumococcal carriage. J Infect Dis 2008;197:
34 Casal J, Tarragó D. Immunity to Streptococcus pneumoniae: factors 1511–1518.
affecting production and efficacy. Curr Opin Infect Dis 2003;16: 55 O’Brien KL, Dagan R. The potential indirect effect of conjugate
219–224. pneumococcal vaccines. Vaccine 2003;21:1815–1825.
35 Vernatter J, Pirofski LA. Current concepts in host-microbe interaction 56 Fujihashi K, Sato S, Kiyono H. Mucosal adjuvants for vaccines to
leading to pneumococcal pneumonia. Curr Opin Infect Dis 2013;26: control upper respiratory infections in the elderly. Exp Gerontol 2014;
277–283. 54:21–26.
36 Olliver M, Hiew J, Mellroth P, Henriques-Normark B, Bergman P. 57 Simonsen L, Taylor RJ, Young-Xu Y, Haber M, May L, Klugman KP.
Human monocytes promote Th1 and Th17 responses to Impact of pneumococcal conjugate vaccination of infants on
Focused Reviews 943
FOCUSED REVIEWS
pneumonia and influenza hospitalization and mortality in all age 70 Nuorti JP, Whitney CG; Centers for Disease Control and Prevention
groups in the United States. MBio 2011;2:e00309–e00310. (CDC). Prevention of pneumococcal disease among infants and
58 Robbins JB, Austrian R, Lee CJ, Rastogi SC, Schiffman G, Henrichsen children - use of 13-valent pneumococcal conjugate vaccine and
J, Mäkelä PH, Broome CV, Facklam RR, Tiesjema RH, et al. 23-valent pneumococcal polysaccharide vaccine: recommendations
Considerations for formulating the second-generation of the Advisory Committee on Immunization Practices (ACIP).
pneumococcal capsular polysaccharide vaccine with emphasis on MMWR Recomm Rep 2010;59:1–18.
the cross-reactive types within groups. J Infect Dis 1983;148: 71 Tomczyk S, Bennett NM, Stoecker C, Gierke R, Moore MR, Whitney
1136–1159. CG, Hadler S, Pilishvili T; Centers for Disease Control and Prevention
59 Fine MJ, Smith MA, Carson CA, Meffe F, Sankey SS, Weissfeld LA, (CDC). Use of 13-valent pneumococcal conjugate vaccine and
Detsky AS, Kapoor WN. Efficacy of pneumococcal vaccination in 23-valent pneumococcal polysaccharide vaccine among adults aged
adults: a meta-analysis of randomized controlled trials. Arch Intern >65 years: recommendations of the Advisory Committee on
Med 1994;154:2666–2677. Immunization Practices (ACIP). MMWR Morb Mortal Wkly Rep 2014;
60 Shapiro ED, Berg AT, Austrian R, Schroeder D, Parcells V, Margolis A, 63:822–825.
Adair RK, Clemens JD. The protective efficacy of polyvalent 72 Lazarus R, Clutterbuck E, Yu LM, Bowman J, Bateman EA, Diggle L,
pneumococcal polysaccharide vaccine. N Engl J Med 1991;325: Angus B, Peto TE, Beverley PC, Mant D, et al. A randomized
1453–1460. study comparing combined pneumococcal conjugate and
61 Black SB, Shinefield HR, Ling S, Hansen J, Fireman B, Spring D, Noyes polysaccharide vaccination schedules in adults. Clin Infect Dis
J, Lewis E, Ray P, Lee J, et al. Effectiveness of heptavalent 2011;52:736–742.
pneumococcal conjugate vaccine in children younger than five years 73 Goldblatt D, Southern J, Andrews N, Ashton L, Burbidge P, Woodgate
of age for prevention of pneumonia. Pediatr Infect Dis J 2002;21: S, Pebody R, Miller E. The immunogenicity of 7-valent
810–815. pneumococcal conjugate vaccine versus 23-valent polysaccharide
62 Hsu HE, Shutt KA, Moore MR, Beall BW, Bennett NM, Craig AS, Farley vaccine in adults aged 50-80 years. Clin Infect Dis 2009;49:
MM, Jorgensen JH, Lexau CA, Petit S, et al. Effect of pneumococcal 1318–1325.
conjugate vaccine on pneumococcal meningitis. N Engl J Med 2009; 74 Miernyk KM, Butler JC, Bulkow LR, Singleton RJ, Hennessy TW,
360:244–256. Dentinger CM, Peters HV, Knutsen B, Hickel J, Parkinson AJ.
63 von Gottberg A, de Gouveia L, Tempia S, Quan V, Meiring S, von Immunogenicity and reactogenicity of pneumococcal
Mollendorf C, Madhi SA, Zell ER, Verani JR, O’Brien KL, et al.; polysaccharide and conjugate vaccines in Alaska native adults 55-70
GERMS-SA Investigators. Effects of vaccination on invasive years of age. Clin Infect Dis 2009;49:241–248.
pneumococcal disease in South Africa. N Engl J Med 2014;371: 75 Jackson LA, Gurtman A, van Cleeff M, Frenck RW, Treanor J, Jansen
1889–1899. KU, Scott DA, Emini EA, Gruber WC, Schmoele-Thoma B. Influence
64 Pilishvili T, Lexau C, Farley MM, Hadler J, Harrison LH, Bennett NM, of initial vaccination with 13-valent pneumococcal conjugate vaccine
Reingold A, Thomas A, Schaffner W, Craig AS, et al.; Active Bacterial or 23-valent pneumococcal polysaccharide vaccine on anti-
Core Surveillance/Emerging Infections Program Network. Sustained pneumococcal responses following subsequent pneumococcal
reductions in invasive pneumococcal disease in the era of conjugate vaccination in adults 50 years and older. Vaccine 2013;31:
vaccine. J Infect Dis 2010;201:32–41. 3594–3602.
65 Hsu KK, Shea KM, Stevenson AE, Pelton SI; Massachusetts 76 Manoff SB, Liss C, Caulfield MJ, Marchese RD, Silber J, Boslego J,
Department of Public Health. Changing serotypes causing childhood Romero-Steiner S, Rajam G, Glass NE, Whitney CG, et al.
invasive pneumococcal disease: Massachusetts, 2001-2007. Pediatr Revaccination with a 23-valent pneumococcal polysaccharide
Infect Dis J 2010;29:289–293. vaccine induces elevated and persistent functional antibody
66 Jackson LA, Gurtman A, van Cleeff M, Jansen KU, Jayawardene D, responses in adults aged 65 . or = years. J Infect Dis 2010;201:
Devlin C, Scott DA, Emini EA, Gruber WC, Schmoele-Thoma B. 525–533.
Immunogenicity and safety of a 13-valent pneumococcal conjugate 77 Musher DM, Manof SB, Liss C, McFetridge RD, Marchese RD, Bushnell
vaccine compared to a 23-valent pneumococcal polysaccharide B, Alvarez F, Painter C, Blum MD, Silber JL. Safety and antibody
vaccine in pneumococcal vaccine-naive adults. Vaccine 2013;31: response, including antibody persistence for 5 years, after primary
3577–3584. vaccination or revaccination with pneumococcal polysaccharide
67 Jackson LA, Gurtman A, Rice K, Pauksens K, Greenberg RN, Jones TR, vaccine in middle-aged and older adults. J Infect Dis 2010;201:
Scott DA, Emini EA, Gruber WC, Schmoele-Thoma B. 516–524.
Immunogenicity and safety of a 13-valent pneumococcal conjugate 78 Grabenstein JD, Manoff SB. Pneumococcal polysaccharide 23-valent
vaccine in adults 70 years of age and older previously vaccinated vaccine: long-term persistence of circulating antibody and
with 23-valent pneumococcal polysaccharide vaccine. Vaccine immunogenicity and safety after revaccination in adults. Vaccine
2013;31:3585–3593. 2012;30:4435–4444.
68 French N, Gordon SB, Mwalukomo T, White SA, Mwafulirwa G, Longwe 79 Bogaert D, van Belkum A, Sluijter M, Luijendijk A, de Groot R, Rümke
H, Mwaiponya M, Zijlstra EE, Molyneux ME, Gilks CF. A trial of a HC, Verbrugh HA, Hermans PW. Colonisation by Streptococcus
7-valent pneumococcal conjugate vaccine in HIV-infected adults. pneumoniae and Staphylococcus aureus in healthy children. Lancet
N Engl J Med 2010;362:812–822. 2004;363:1871–1872.
69 Bonten MJ, Huijts SM, Bolkenbaas M, Webber C, Patterson S, Gault S, 80 Terra VS, Mills DC, Yates LE, Abouelhadid S, Cuccui J, Wren BW.
van Werkhoven CH, van Deursen AM, Sanders EA, Verheij TJ, et al. Recent developments in bacterial protein glycan coupling
Polysaccharide conjugate vaccine against pneumococcal technology and glycoconjugate vaccine design. J Med Microbiol
pneumonia in adults. N Engl J Med 2015;372:1114–1125. 2012;61:919–926.
944 AnnalsATS Volume 13 Number 6 | June 2016
You might also like
- Focused Reviews: Pneumococcal Vaccination StrategiesDocument12 pagesFocused Reviews: Pneumococcal Vaccination StrategiesrafaelreanoNo ratings yet
- Pneumonia ComunitariaDocument10 pagesPneumonia ComunitariaMaulida HalimahNo ratings yet
- Woolfrey2012 PDFDocument22 pagesWoolfrey2012 PDFJorge BarriosNo ratings yet
- Neumococo en NacDocument15 pagesNeumococo en NacMNo ratings yet
- Community-Acquired Pneumonia: An Overview: Clinical Feature ReviewDocument9 pagesCommunity-Acquired Pneumonia: An Overview: Clinical Feature ReviewAncuta CalimentNo ratings yet
- Pneumococcal Pneumonia in Children - UpToDateDocument30 pagesPneumococcal Pneumonia in Children - UpToDatejess.khoo.1204No ratings yet
- Microorganisms 11 01376Document16 pagesMicroorganisms 11 01376Ioana MariaNo ratings yet
- Clinical Presentation and Diagnosis of Pneumocystis Pulmonary Infection in HIV-infected PatientsDocument23 pagesClinical Presentation and Diagnosis of Pneumocystis Pulmonary Infection in HIV-infected PatientsAndréia GomesNo ratings yet
- Epidemiological Profile of Acute Typical Bacterial Pneumonia at The National Reference University Hospital Center of NDjamena Risk Factors and Antibiotic ResistanceDocument13 pagesEpidemiological Profile of Acute Typical Bacterial Pneumonia at The National Reference University Hospital Center of NDjamena Risk Factors and Antibiotic ResistanceAthenaeum Scientific PublishersNo ratings yet
- Pneumonia - PMCDocument21 pagesPneumonia - PMCDhany karubuyNo ratings yet
- Case Study PcapDocument3 pagesCase Study PcapClaire PalaciosNo ratings yet
- Bruyere Case13 001-012 DSDocument11 pagesBruyere Case13 001-012 DSjrnataNo ratings yet
- Pneumocistosis en VIHDocument14 pagesPneumocistosis en VIHSergio GarciaNo ratings yet
- Pneumonia Pada AnakDocument36 pagesPneumonia Pada AnakSilvestri PurbaNo ratings yet
- Prevencion de La Neumonia en Los Pacientes AncianosDocument10 pagesPrevencion de La Neumonia en Los Pacientes AncianosAlexandra RojasNo ratings yet
- Necrotizing Pneumonia (Aetiology, Clinical Features and Management)Document8 pagesNecrotizing Pneumonia (Aetiology, Clinical Features and Management)pachomdNo ratings yet
- Clinical Presentation and Diagnosis of Pneumocystis Pulmonary Infection in HIVDocument42 pagesClinical Presentation and Diagnosis of Pneumocystis Pulmonary Infection in HIVmariano villavicencioNo ratings yet
- Lower Respiratory Tract Infections: Prevention Using VaccinesDocument19 pagesLower Respiratory Tract Infections: Prevention Using VaccinesYampold Estheben ChusiNo ratings yet
- Acute Bacterial and Viral MeningitisDocument16 pagesAcute Bacterial and Viral MeningitisMaharani MahaNo ratings yet
- Meningite Aguda Bacteriana Rev Lancet 2016Document12 pagesMeningite Aguda Bacteriana Rev Lancet 2016elsonverdadeNo ratings yet
- Infectious Complications in Patients With Lung Cancer: K.S. Akinosoglou, K. Karkoulias, M. MarangosDocument11 pagesInfectious Complications in Patients With Lung Cancer: K.S. Akinosoglou, K. Karkoulias, M. Marangosabbhyasa5206No ratings yet
- 6.2. NeumoníaDocument5 pages6.2. NeumoníaErmilo José Echeverría OrtegónNo ratings yet
- JCM 12 02256Document14 pagesJCM 12 02256drtatitaNo ratings yet
- 18 UpToDate NeumoníaDocument113 pages18 UpToDate NeumoníaAl DavisNo ratings yet
- Influenzaandviral Pneumonia: Rodrigo Cavallazzi,, Julio A. RamirezDocument19 pagesInfluenzaandviral Pneumonia: Rodrigo Cavallazzi,, Julio A. Ramirezlevani memarneNo ratings yet
- Neumonia Complicada PDFDocument9 pagesNeumonia Complicada PDFadriana gallardoNo ratings yet
- Pyogenic Bacterial Pneumonia and Lung Abscess: Staphylococcus Aureus, Pseudomonas AeruginosaDocument5 pagesPyogenic Bacterial Pneumonia and Lung Abscess: Staphylococcus Aureus, Pseudomonas AeruginosaVladimir Tigrero ZernaNo ratings yet
- Seminar: Olli Ruuskanen, Elina Lahti, Lance C Jennings, David R MurdochDocument12 pagesSeminar: Olli Ruuskanen, Elina Lahti, Lance C Jennings, David R MurdochChika AmeliaNo ratings yet
- Antibioticoterapia Na Pneumonia Pediátrica 2006Document7 pagesAntibioticoterapia Na Pneumonia Pediátrica 2006Tainah__100% (1)
- 2021 - TorresDocument28 pages2021 - TorresCarlosNo ratings yet
- Pneumonia and Invasive Pneumococcal Diseases - The Role of Pneumococcal Conjugate Vaccine in The Era of Multi-Drug Resistance - PMCDocument33 pagesPneumonia and Invasive Pneumococcal Diseases - The Role of Pneumococcal Conjugate Vaccine in The Era of Multi-Drug Resistance - PMC90Agva Dwi FatikaNo ratings yet
- New Insights Into The Treatment of Acute Otitis MediaDocument13 pagesNew Insights Into The Treatment of Acute Otitis MediaAGUS DE COLSANo ratings yet
- NeumoniaDocument28 pagesNeumoniaresidentes isssteNo ratings yet
- 1209.full Sadikot PDFDocument15 pages1209.full Sadikot PDFmufqifitra160491No ratings yet
- Pulmonary Infiltrates in The Non-HIV-Infected Immunocompromised PatientDocument12 pagesPulmonary Infiltrates in The Non-HIV-Infected Immunocompromised PatientAri KuncoroNo ratings yet
- Duke 2019Document3 pagesDuke 2019Diego AndradeNo ratings yet
- Meningitis Bacteriana Clinicas 2018Document12 pagesMeningitis Bacteriana Clinicas 2018carlos ballestasNo ratings yet
- Piis0140673610614596 PDFDocument12 pagesPiis0140673610614596 PDFMagdalenoNo ratings yet
- Addis Ababa University: Collage of Health Science Pediatrics and Neonatology On PneumoniaDocument21 pagesAddis Ababa University: Collage of Health Science Pediatrics and Neonatology On PneumoniaCheru DugaseNo ratings yet
- Mycoplasma Infect The Upper Respiratory Tract and Can Cause Pneumonia. Pneumonia Is AnDocument11 pagesMycoplasma Infect The Upper Respiratory Tract and Can Cause Pneumonia. Pneumonia Is AnJenny TaylorNo ratings yet
- Why Is The Rate of PneumococcalDocument7 pagesWhy Is The Rate of PneumococcalEduarda QuartinNo ratings yet
- Research ArticleDocument17 pagesResearch ArticleNatanael KindangenNo ratings yet
- Meningitis Bacteriana Aguda en El AdultoDocument12 pagesMeningitis Bacteriana Aguda en El AdultoJulian AlbarracínNo ratings yet
- MICROBIAL DISEASE Pneumococcal PneumoniaDocument7 pagesMICROBIAL DISEASE Pneumococcal PneumoniaShalini DoraisingamNo ratings yet
- Nosocomial: Infections in The Neonatal Intensive Care UnitDocument9 pagesNosocomial: Infections in The Neonatal Intensive Care UnitCleoanne Gallegos100% (1)
- Epidemiology, Pathogenesis, and Microbiology of Community-Acquired Pneumonia in AdultsDocument19 pagesEpidemiology, Pathogenesis, and Microbiology of Community-Acquired Pneumonia in AdultsRubén RodríguezNo ratings yet
- Pneumonia: Meningococcal Pneumonia: A ReviewDocument13 pagesPneumonia: Meningococcal Pneumonia: A ReviewRizki Handayani SiregarNo ratings yet
- 5 - Pneumococcal Disease Infections Caused by Stre - 2012 - Netter S InfectiousDocument5 pages5 - Pneumococcal Disease Infections Caused by Stre - 2012 - Netter S InfectiousstasiulinoNo ratings yet
- Pneumonia em Pac Com Cancer PDFDocument15 pagesPneumonia em Pac Com Cancer PDFleca_medica20144849No ratings yet
- Congenital and Neonatal Pneumonia PAEDIATRIC RESPIRATORY REVIEWS (2007) 8, 195-203 Michael D. NissenDocument9 pagesCongenital and Neonatal Pneumonia PAEDIATRIC RESPIRATORY REVIEWS (2007) 8, 195-203 Michael D. Nissenroggers72No ratings yet
- Special Considerations of Antibiotic Prescription in The Geriatric PopulationDocument7 pagesSpecial Considerations of Antibiotic Prescription in The Geriatric PopulationLydiaphNo ratings yet
- Pneumonia in Children - Epidemiology, Pathogenesis, and Etiology - UpToDateDocument29 pagesPneumonia in Children - Epidemiology, Pathogenesis, and Etiology - UpToDatejess.khoo.1204No ratings yet
- Coccidioidomycosis PDFDocument7 pagesCoccidioidomycosis PDFAustine OsaweNo ratings yet
- Vaccination in Asplenic PatientsDocument10 pagesVaccination in Asplenic PatientsNihal S KiranNo ratings yet
- Pneumonia in Children - Epidemiology, Pathogenesis, and Etiology - UpToDateDocument30 pagesPneumonia in Children - Epidemiology, Pathogenesis, and Etiology - UpToDateDavid QuinteroNo ratings yet
- Viral Meningitis: David R. ChadwickDocument14 pagesViral Meningitis: David R. ChadwickVina HardiantiNo ratings yet
- Essential Update: Pediatric Pneumonia May Be Effectively Treated With Twice-Daily AmoxicillinDocument54 pagesEssential Update: Pediatric Pneumonia May Be Effectively Treated With Twice-Daily AmoxicillinYostesara Maurena SantosaNo ratings yet
- SMITH Et Al 2012 RespirologyDocument14 pagesSMITH Et Al 2012 RespirologyJosue AvalosNo ratings yet
- Influenza vaccination: What does the scientific proof say?: Could it be more harmful than useful to vaccinate indiscriminately elderly people, pregnant women, children and health workers?From EverandInfluenza vaccination: What does the scientific proof say?: Could it be more harmful than useful to vaccinate indiscriminately elderly people, pregnant women, children and health workers?No ratings yet
- SR JR Corrigendum 010819Document1 pageSR JR Corrigendum 010819Rishi MangalNo ratings yet
- Estimation of PO2 and FiO2 PDFDocument1 pageEstimation of PO2 and FiO2 PDFRishi MangalNo ratings yet
- Thoracic Surgery Secrets Book PDFDocument4 pagesThoracic Surgery Secrets Book PDFRishi MangalNo ratings yet
- Motor Insurance - Two Wheeler Comprehensive PolicyDocument3 pagesMotor Insurance - Two Wheeler Comprehensive PolicyRishi MangalNo ratings yet
- 1549702645026sUKFJlx63rXI9ecx PDFDocument6 pages1549702645026sUKFJlx63rXI9ecx PDFRishi MangalNo ratings yet
- Thoracic Surgery Secrets Book PDFDocument4 pagesThoracic Surgery Secrets Book PDFRishi MangalNo ratings yet
- Phase9 210519 AmmendmentDocument1 pagePhase9 210519 AmmendmentRishi MangalNo ratings yet
- Covid-19 mRNA VaccinesDocument16 pagesCovid-19 mRNA VaccinesSargent Goodchild100% (2)
- RBSC2013 Abstract BookDocument138 pagesRBSC2013 Abstract BookPETIENo ratings yet
- Hypersensitivity Reactions: Type III and Type IV HypersensitivityDocument36 pagesHypersensitivity Reactions: Type III and Type IV HypersensitivityDil NavabNo ratings yet
- Acscentsci 1c00120Document22 pagesAcscentsci 1c00120Beverly EstoqueNo ratings yet
- White Blood CellDocument21 pagesWhite Blood CellAnonymous 0C4OZmRNo ratings yet
- Novavax Initiates COVID-19 Vaccine Clinical Trial CrossoverDocument2 pagesNovavax Initiates COVID-19 Vaccine Clinical Trial CrossoverDavid SantosNo ratings yet
- Cancer ImmunologyDocument31 pagesCancer ImmunologyAbdul FarooqNo ratings yet
- Antigens: Martha Margarita G. Arevalo Ana Mikaela D.O. de AsisDocument44 pagesAntigens: Martha Margarita G. Arevalo Ana Mikaela D.O. de AsisCherry Reyes-PrincipeNo ratings yet
- 9700 w09 Ms 21Document7 pages9700 w09 Ms 21Karen OngNo ratings yet
- 5 2 3 Genomes and Gene Technology All Past Paper QuestionsDocument32 pages5 2 3 Genomes and Gene Technology All Past Paper QuestionsblessingaliuNo ratings yet
- Exosome-Based Immunotherapy: A Promising Approach For Cancer TreatmentDocument16 pagesExosome-Based Immunotherapy: A Promising Approach For Cancer Treatment1810 15Marvin LionelNo ratings yet
- Drug Induced Liver Injury: An UpdateDocument27 pagesDrug Induced Liver Injury: An UpdateMari QcNo ratings yet
- Odisha PG Zoology SyllabusDocument35 pagesOdisha PG Zoology SyllabusThe IdyllicxNo ratings yet
- UntitledDocument23 pagesUntitledPravinNo ratings yet
- KUBYDocument5 pagesKUBYCristina CisnerosNo ratings yet
- Clonal Selection AlgorithmsDocument13 pagesClonal Selection AlgorithmsKumar NoriNo ratings yet
- HKDSE Biology Part 3 Health & DiseasesDocument17 pagesHKDSE Biology Part 3 Health & DiseasesTSZ YAN CHEUNGNo ratings yet
- Chapter 10Document24 pagesChapter 10Kandarpa SaikiaNo ratings yet
- HarrisDocument35 pagesHarrisMariel AbatayoNo ratings yet
- C5. Viral VaccineDocument16 pagesC5. Viral VaccineBen BuddyNo ratings yet
- Allen 2002 Recent Advances in Biology and Immunobiology of Eimeria Species and in Diagnosis and Control of InfectionDocument8 pagesAllen 2002 Recent Advances in Biology and Immunobiology of Eimeria Species and in Diagnosis and Control of InfectionRicardo Alberto Mejia OspinaNo ratings yet
- Property of Medtech Review Notes Do Not Distribute: Innate ImmunityDocument16 pagesProperty of Medtech Review Notes Do Not Distribute: Innate ImmunityCallie JaasielNo ratings yet
- Hla TypingDocument23 pagesHla Typingandri perdanaNo ratings yet
- Full Download Test Bank For Immunology and Serology in Laboratory Medicine 6th Edition by Turgeon PDF Full ChapterDocument36 pagesFull Download Test Bank For Immunology and Serology in Laboratory Medicine 6th Edition by Turgeon PDF Full Chapterstoredannage1uf100% (15)
- This Is A Bio-Attack AlertDocument10 pagesThis Is A Bio-Attack AlertJohn Burns100% (2)
- Disease and ImmunityDocument22 pagesDisease and ImmunityGuna VallabhNo ratings yet
- Wiki Therepeutic Vax (No BS)Document4 pagesWiki Therepeutic Vax (No BS)Jack NestelroadNo ratings yet
- Unit 2: Disease Prevention: Pkids' Infectious Disease WorkshopDocument21 pagesUnit 2: Disease Prevention: Pkids' Infectious Disease WorkshopCharlene Fadrigon-OtazuNo ratings yet
- @MedicalBooksStore 2014 ContraceptionDocument315 pages@MedicalBooksStore 2014 ContraceptionBernardo Fernandez SalazarNo ratings yet
- Worksheet 1 - Human GeneticsDocument4 pagesWorksheet 1 - Human GeneticsLei Zaira BiendimaNo ratings yet