You might also like
- Acad Dermatol Venereol - 2015 - Leccia - Topical Acne Treatments in Europe and The Issue of Antimicrobial ResistanceDocument8 pagesAcad Dermatol Venereol - 2015 - Leccia - Topical Acne Treatments in Europe and The Issue of Antimicrobial Resistancealihassan.ph40No ratings yet
- Sabiiti Et Al 2019 Heat Inactivation Renders Sputum Safe and Preserves Mycobacterium Tuberculosis Rna For DownstreamDocument8 pagesSabiiti Et Al 2019 Heat Inactivation Renders Sputum Safe and Preserves Mycobacterium Tuberculosis Rna For DownstreamsrambofheniNo ratings yet
- Hrabak 2014Document15 pagesHrabak 2014Ignacio Velasquez MiñoNo ratings yet
- Colson 2016Document4 pagesColson 2016rabbanibreNo ratings yet
- 5 E Coli in UTIDocument7 pages5 E Coli in UTIGhadah AlyousifNo ratings yet
- Ultimos AntimicrobianosDocument3 pagesUltimos Antimicrobianosmargarita rodriguezNo ratings yet
- Artigo 03 Filmarray PneumoniaDocument6 pagesArtigo 03 Filmarray Pneumoniapriscila pimentel martinelliNo ratings yet
- Lismond AntibiotikDocument14 pagesLismond AntibiotikSaadah 0210No ratings yet
- Antimicrobial Resistance Genetic Lineages and BiofDocument12 pagesAntimicrobial Resistance Genetic Lineages and BiofNäjlãå SlnNo ratings yet
- 2014 Article 47 PDFDocument7 pages2014 Article 47 PDFalif bagusNo ratings yet
- s12879 019 4536 8Document11 pagess12879 019 4536 8mariamaNo ratings yet
- Microorganisms 11 01474Document19 pagesMicroorganisms 11 01474hawamasfufahNo ratings yet
- Pharmaceutics 14 01678Document14 pagesPharmaceutics 14 01678Ana ApolinárioNo ratings yet
- Jurnal Eucast LainnyaDocument228 pagesJurnal Eucast Lainnyaonly taaNo ratings yet
- Jurnal Mikfar Utari 2-1Document10 pagesJurnal Mikfar Utari 2-1Azri Aprisonia SaritaNo ratings yet
- Intensive Care Unit-Acquired Infections in A Moroccan Teaching Hospital: Epidemiology, Risk Factors and OutcomeDocument13 pagesIntensive Care Unit-Acquired Infections in A Moroccan Teaching Hospital: Epidemiology, Risk Factors and OutcomePrimasari DiahNo ratings yet
- Nosocomial Infection in Burn Unit of Cipto Mangunkusumo Hospital, JakartaDocument5 pagesNosocomial Infection in Burn Unit of Cipto Mangunkusumo Hospital, JakartaDennyKurniawanNo ratings yet
- Genomic Epidemiology Reveals Multiple Mechanisms of Linezolid Resistance in Clinical Enterococci in ChinaDocument11 pagesGenomic Epidemiology Reveals Multiple Mechanisms of Linezolid Resistance in Clinical Enterococci in Chinad4rkgr455No ratings yet
- Genomic Epidemiology Reveals Multiple Mechanisms of Linezolid Resistance in Clinical Enterococci in ChinaDocument11 pagesGenomic Epidemiology Reveals Multiple Mechanisms of Linezolid Resistance in Clinical Enterococci in Chinad4rkgr455No ratings yet
- Clin Microbiology Infect - 2013 - Tacconelli - ESCMID Guidelines For The Management of The Infection Control Measures ToDocument55 pagesClin Microbiology Infect - 2013 - Tacconelli - ESCMID Guidelines For The Management of The Infection Control Measures ToJhon PincayNo ratings yet
- 1 s2.0 S1876034120300046 MainDocument9 pages1 s2.0 S1876034120300046 MainYHCT K45 Bùi Ngọc Bảo TrânNo ratings yet
- UntitledDocument10 pagesUntitledLalainasoa Odile RivoarilalaNo ratings yet
- Daptomycin For The Treatment of Bacteraemia Du - 2014 - International Journal ofDocument9 pagesDaptomycin For The Treatment of Bacteraemia Du - 2014 - International Journal ofPatricio Suazo SotoNo ratings yet
- Comparison of Gene-Xpert and Line Probe Assay For Detection of Mycobacterium Tuberculosis and Rifampicin-Mono ResistanceDocument8 pagesComparison of Gene-Xpert and Line Probe Assay For Detection of Mycobacterium Tuberculosis and Rifampicin-Mono ResistanceFaradilla FirdausaNo ratings yet
- Time-Kill Curve Analysis and Pharmacodynamic Modelling For in Vitro Evaluation of Antimicrobials Against Neisseria GonorrhoeaeDocument11 pagesTime-Kill Curve Analysis and Pharmacodynamic Modelling For in Vitro Evaluation of Antimicrobials Against Neisseria GonorrhoeaeRonaldo MachadoNo ratings yet
- The Revolution of Lateral Flow Assay in The Field of AMRDetectionDocument26 pagesThe Revolution of Lateral Flow Assay in The Field of AMRDetectionalbertNo ratings yet
- Antibacterial Activity of Blue Light Against Nosocomial Wound Pathogens Growing Planktonically and As Mature BiofilmsDocument11 pagesAntibacterial Activity of Blue Light Against Nosocomial Wound Pathogens Growing Planktonically and As Mature Biofilmscecy loNo ratings yet
- Evolution of The Antimicrobial Resistance Rates in Clinical Isolates of Pseudomonas Aeruginosa Causing Invasive Infections in The South of SpainDocument5 pagesEvolution of The Antimicrobial Resistance Rates in Clinical Isolates of Pseudomonas Aeruginosa Causing Invasive Infections in The South of SpainDostin JasserNo ratings yet
- In Vitro Susceptibility of Four Antimicrobials AgaDocument8 pagesIn Vitro Susceptibility of Four Antimicrobials Agathanh ba matNo ratings yet
- A Review and Perspectives For Covid-19 TreatmentDocument19 pagesA Review and Perspectives For Covid-19 Treatmentkristine.claacctngNo ratings yet
- s13756 017 0195 yDocument7 pagess13756 017 0195 yTonny YuliantoNo ratings yet
- JM 002169Document4 pagesJM 002169edisonballaNo ratings yet
- Lep120 123 PDFDocument4 pagesLep120 123 PDFaghorbanzadehNo ratings yet
- Patterned SurfacesDocument10 pagesPatterned SurfacesAndri WigunaNo ratings yet
- Study On Emergence of MDR Pathogen and Its Microbiological StudyDocument9 pagesStudy On Emergence of MDR Pathogen and Its Microbiological StudyIJAR JOURNALNo ratings yet
- Assessment of Susceptibility To Five Common Antibiotics and Their Resistance Pattern in Clinical Enterococcus IsolatesDocument10 pagesAssessment of Susceptibility To Five Common Antibiotics and Their Resistance Pattern in Clinical Enterococcus IsolatesIsidora NikolicNo ratings yet
- Genotypic Characterization of Mycobacterium Tuberculosis Strains Resistant To Rifampicin Isoniazid and Second Line Antibiotics in ChadDocument14 pagesGenotypic Characterization of Mycobacterium Tuberculosis Strains Resistant To Rifampicin Isoniazid and Second Line Antibiotics in ChadAthenaeum Scientific PublishersNo ratings yet
- A Retrospective Observational Study On The Sputum Samples Received by The Department of Microbiology, Teaching Hospital, Karapitiya in The Year 2007Document5 pagesA Retrospective Observational Study On The Sputum Samples Received by The Department of Microbiology, Teaching Hospital, Karapitiya in The Year 2007Rahmi AmiNo ratings yet
- Potential Properties of Lactobacillus Plantarum F-10 As A Bio-Control Strategy For Wound InfectionsDocument14 pagesPotential Properties of Lactobacillus Plantarum F-10 As A Bio-Control Strategy For Wound InfectionsIgor BaltaNo ratings yet
- 10 1093@jac@dky192Document8 pages10 1093@jac@dky192Rahmad SyamsulNo ratings yet
- Puyen 2022 MICDocument11 pagesPuyen 2022 MICRoger CNo ratings yet
- Ofy 064Document3 pagesOfy 064Robert StryjakNo ratings yet
- Mycoplasma Pneumoniae: Prevalance in Navi Mumbai, India Biomedical. Indian Journal of Applied ResearchDocument4 pagesMycoplasma Pneumoniae: Prevalance in Navi Mumbai, India Biomedical. Indian Journal of Applied ResearchSpinalis 2017No ratings yet
- Correlation Between A Baumanii Resistance and Hospital Use of Meropenem 2021Document12 pagesCorrelation Between A Baumanii Resistance and Hospital Use of Meropenem 2021czikkely23No ratings yet
- Polymicrobial Ventilator-Associated Pneumonia: Fighting in Vitro Candida albicans-Antifungal-Antibacterial Combination TherapyDocument19 pagesPolymicrobial Ventilator-Associated Pneumonia: Fighting in Vitro Candida albicans-Antifungal-Antibacterial Combination TherapyFarhanNo ratings yet
- A Rat Model of Central Venous Catheter To Study Establishment of Long-Term Bacterial Biofilm and Related Acute and Chronic InfectionsDocument12 pagesA Rat Model of Central Venous Catheter To Study Establishment of Long-Term Bacterial Biofilm and Related Acute and Chronic InfectionsDodoNo ratings yet
- Icmr-National Institute For Research in Tuberculosis-ChennaiDocument27 pagesIcmr-National Institute For Research in Tuberculosis-Chennaidhanya sriNo ratings yet
- New and Repurposed Drugs To Treat Multidrug-And Extensively Drug-Resistant TuberculosisDocument8 pagesNew and Repurposed Drugs To Treat Multidrug-And Extensively Drug-Resistant TuberculosisJUAN SARMIENTONo ratings yet
- José Domínguez Clinical Implications of MolecularDocument16 pagesJosé Domínguez Clinical Implications of MolecularcarolNo ratings yet
- Antimicrobial Susceptibility Against MetronidazoleDocument7 pagesAntimicrobial Susceptibility Against MetronidazolekityamuwesiNo ratings yet
- Journal Pre-Proof: Trends in Plant ScienceDocument17 pagesJournal Pre-Proof: Trends in Plant ScienceMUGDHA MITTALNo ratings yet
- Silver Nanoparticles As Potential Antiviral AgentsDocument25 pagesSilver Nanoparticles As Potential Antiviral AgentscreatrNo ratings yet
- Bepridil Is Potent Against SARS-CoV-2 in VitroDocument28 pagesBepridil Is Potent Against SARS-CoV-2 in VitrosovalaxNo ratings yet
- Accepted Manuscript: International Journal of Antimicrobial AgentsDocument16 pagesAccepted Manuscript: International Journal of Antimicrobial AgentsAdrian Quiroga RodriguezNo ratings yet
- Polymeric Nanoparticles and Nanomicelles of Hydroxychloroquine Co Loaded With Azithromycin Potentiate Anti Sars Cov 2 EffectDocument19 pagesPolymeric Nanoparticles and Nanomicelles of Hydroxychloroquine Co Loaded With Azithromycin Potentiate Anti Sars Cov 2 EffectGabriella Rdg'zNo ratings yet
- 32 Vol. 7 Issue 9 September 2016 IJPSR RA 6515Document5 pages32 Vol. 7 Issue 9 September 2016 IJPSR RA 6515Monyet...No ratings yet
- (M299) RL3Document11 pages(M299) RL3Jessa Louise TurredaNo ratings yet
- Clinical Spectrum and Antibiogram of Acinetobacter Infections in Children Study From A Tertiary Care Centre, IndiaDocument12 pagesClinical Spectrum and Antibiogram of Acinetobacter Infections in Children Study From A Tertiary Care Centre, IndiaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Delgado-Valverde, Clinical Management of Infections Caused by Multidrug-Resistant Enterobacteriaceae (Ótimo)Document22 pagesDelgado-Valverde, Clinical Management of Infections Caused by Multidrug-Resistant Enterobacteriaceae (Ótimo)fjr.celioNo ratings yet
- Surgical CricothyroidotomyDocument1 pageSurgical Cricothyroidotomyintan rosliNo ratings yet
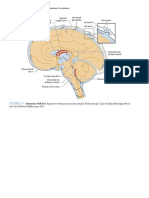
- Figure 3-7: PART I Neuroanatomy and Neuroanatomic LocalizationDocument1 pageFigure 3-7: PART I Neuroanatomy and Neuroanatomic Localizationintan rosliNo ratings yet
- Orthopaedic AnatomyDocument1 pageOrthopaedic Anatomyintan rosliNo ratings yet
- Translocation NeuromaDocument1 pageTranslocation Neuromaintan rosliNo ratings yet
- Translocation NeuromaDocument1 pageTranslocation Neuromaintan rosliNo ratings yet
- 7.2 Non-Absorbable Suture MaterialsDocument1 page7.2 Non-Absorbable Suture Materialsintan rosliNo ratings yet
- Corticosteroid Injection For de Quervain's Tenosynovitis (Review)Document19 pagesCorticosteroid Injection For de Quervain's Tenosynovitis (Review)intan rosliNo ratings yet
- Developing and Evaluating An Eighth Grade Curriculum Unit That Links Foundational Chemistry To Biological GrowthDocument29 pagesDeveloping and Evaluating An Eighth Grade Curriculum Unit That Links Foundational Chemistry To Biological GrowthHashir QaisarNo ratings yet
- Redox Biology: Bernard Schmitt, Morgane Vicenzi, Catherine Garrel, Frédéric M. DenisDocument8 pagesRedox Biology: Bernard Schmitt, Morgane Vicenzi, Catherine Garrel, Frédéric M. Denisrocio fernandez san juanNo ratings yet
- BMLT Workbook 1st SemDocument26 pagesBMLT Workbook 1st SemAnamika ThakurNo ratings yet
- Blood - تقرير عن الدم PDFDocument11 pagesBlood - تقرير عن الدم PDFSadon B AsyNo ratings yet
- The King of Freshwater: Keeping Discus, We Show You How!Document39 pagesThe King of Freshwater: Keeping Discus, We Show You How!manuelNo ratings yet
- Activity 26 Testing Leaves For StarchDocument3 pagesActivity 26 Testing Leaves For StarchDinesCidNo ratings yet
- AQA Biology Topic 8.3 Structures of Ribonucleic AcidDocument4 pagesAQA Biology Topic 8.3 Structures of Ribonucleic AcidfNo ratings yet
- Ch9 GaygeneDocument10 pagesCh9 GaygeneMbiami HermanNo ratings yet
- White MagicDocument182 pagesWhite Magicgodfrey73100% (7)
- Rizal University: TechnologicalDocument2 pagesRizal University: TechnologicalMark L. TumaliuanNo ratings yet
- Full Body Reflexology Chart Template Free PDF Format PDFDocument37 pagesFull Body Reflexology Chart Template Free PDF Format PDFShadrina Al Shafama100% (3)
- Reproduction and Hereditary UnitDocument7 pagesReproduction and Hereditary UnitBiologyhelper PersonNo ratings yet
- All You Ever Wanted To Know About Earth MagicDocument3 pagesAll You Ever Wanted To Know About Earth MagicSatish BoraNo ratings yet
- Environics Paper On Geopathic StresDocument5 pagesEnvironics Paper On Geopathic StresramachariNo ratings yet
- Jethno S 20 01027Document39 pagesJethno S 20 01027Krum V BardarovNo ratings yet
- Outer West HMCA AreaDocument88 pagesOuter West HMCA AreaJohn BaronNo ratings yet
- Pedia Case File PDFDocument25 pagesPedia Case File PDFSanskriti SinghNo ratings yet
- Lesson-27 Quality Control in CytologyDocument5 pagesLesson-27 Quality Control in CytologySasa AbassNo ratings yet
- Tratamento Dirofilariose AHS Canine GuidelinesDocument30 pagesTratamento Dirofilariose AHS Canine GuidelinesRaca DistribuidoraNo ratings yet
- 11th Bio Zoology EM Official Answer Keys For Public Exam Mhay 2022 PDF DownloadDocument3 pages11th Bio Zoology EM Official Answer Keys For Public Exam Mhay 2022 PDF DownloadS. TAMIZHANNo ratings yet
- Microbial Degradation and Valorization of Plastic WastesDocument20 pagesMicrobial Degradation and Valorization of Plastic WastesSpingus CharlestonNo ratings yet
- Komposisi Jenis Dan Struktur Hutan Kerangas BekasDocument5 pagesKomposisi Jenis Dan Struktur Hutan Kerangas BekasErna Karlinna D. YanthyNo ratings yet
- 1 A 2 AfcDocument6 pages1 A 2 AfcMahina WongNo ratings yet
- 1 - UK Lamuno Plus BrochureDocument2 pages1 - UK Lamuno Plus BrochurePhyo WaiNo ratings yet
- Hertz FrequenciesDocument1 pageHertz FrequenciesCharma Lee100% (2)
- Chapter 1 - Introduction and History of Microbiology-1-1Document26 pagesChapter 1 - Introduction and History of Microbiology-1-1Amanawit Gezahegn50% (2)
- Skripsi: Andini Dwi Putri 05071181520031Document19 pagesSkripsi: Andini Dwi Putri 05071181520031RinaERpienaNo ratings yet
- Neurons and Nerve Impulses: Nandika Arora and Risa Gaikwad (11 G2)Document17 pagesNeurons and Nerve Impulses: Nandika Arora and Risa Gaikwad (11 G2)RisaNo ratings yet
- More Words - List Words Ending With AllyDocument72 pagesMore Words - List Words Ending With AllyPietroNo ratings yet
- Literature Review of Dna FingerprintingDocument4 pagesLiterature Review of Dna Fingerprintingc5r0xg9z100% (1)