You might also like
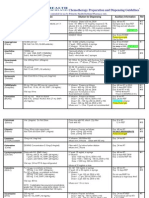
- Chemo Chart Final 121509Document7 pagesChemo Chart Final 121509José Mauricio Peñaloza100% (3)
- Health Seeking Behavior NCPDocument2 pagesHealth Seeking Behavior NCPTrisha Cayabyab0% (1)
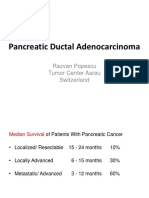
- Europe Balkan Course 2018 Systemic Management of Pancreatic Cancer PopescuDocument64 pagesEurope Balkan Course 2018 Systemic Management of Pancreatic Cancer PopescuCripto MonedeNo ratings yet
- Abstract #4033Document26 pagesAbstract #4033Yareni ReyesNo ratings yet
- CCO Melanoma Clin Impact Slideset2Document27 pagesCCO Melanoma Clin Impact Slideset2Paola Yepez LugoNo ratings yet
- CCO NSCLC IO Discussion Slideset1Document28 pagesCCO NSCLC IO Discussion Slideset1Yasar HammorNo ratings yet
- Nasopharyngeal Carcinoma: Site Specific Approaches, 2008Document21 pagesNasopharyngeal Carcinoma: Site Specific Approaches, 2008Kartika RezkyNo ratings yet
- Pembrolizumab Plus Pemetrexedplatinum For Metastatic Nonsquamous NSCLC KEYNOTE 189 Japan StudyDocument11 pagesPembrolizumab Plus Pemetrexedplatinum For Metastatic Nonsquamous NSCLC KEYNOTE 189 Japan StudyasdffdsaNo ratings yet
- Advances in The Management of Non Small Cell Lung CancerDocument53 pagesAdvances in The Management of Non Small Cell Lung CancerRashid AyubiNo ratings yet
- SOFIE FAP Webinar 2023Document42 pagesSOFIE FAP Webinar 2023Shibin JayakrishnanNo ratings yet
- Randomized Clinical Trials in Localised Anal Cancer (2017)Document14 pagesRandomized Clinical Trials in Localised Anal Cancer (2017)Michelle LEINo ratings yet
- ESMO Breast 2020 Presentation Dent Final Results of The Double Blind Placebo PBO Controlled Randomized Phase 2 LOTUS TrialDocument18 pagesESMO Breast 2020 Presentation Dent Final Results of The Double Blind Placebo PBO Controlled Randomized Phase 2 LOTUS TrialJoju SebastianNo ratings yet
- F DOPA y Otros RF Pet en TNEDocument24 pagesF DOPA y Otros RF Pet en TNEMon Ti TaNo ratings yet
- Bi Omar CadresDocument33 pagesBi Omar CadresNataly Butrón BustamanteNo ratings yet
- Emergence of Immunotherapy As A Cancer Treatment - Feb 26 2018Document50 pagesEmergence of Immunotherapy As A Cancer Treatment - Feb 26 2018KaramSoftNo ratings yet
- Intermittent Versus Continuous Systemic Therapy For Metastatic Colorectal CancerDocument34 pagesIntermittent Versus Continuous Systemic Therapy For Metastatic Colorectal CanceraritrisnawatiNo ratings yet
- Molecular Pathology of Breast CancerDocument42 pagesMolecular Pathology of Breast CancerleartaNo ratings yet
- Hamid 2018Document5 pagesHamid 2018AbulHasan Idrus IstarNo ratings yet
- Early Breast UpdatesDocument59 pagesEarly Breast UpdatesYogesh ShindeNo ratings yet
- Association of Folate Gene SNPs and Breast Cancer RiskDocument42 pagesAssociation of Folate Gene SNPs and Breast Cancer RiskFaisal AliNo ratings yet
- Right Vs Left CRC Final 1Document47 pagesRight Vs Left CRC Final 1Hemanth KumarNo ratings yet
- Gene Xpert Ultra JC Sayan FinalDocument40 pagesGene Xpert Ultra JC Sayan FinalmeghaNo ratings yet
- 2 TishleDocument38 pages2 TishleIRANo ratings yet
- 2017 Article 141 Part1Document5 pages2017 Article 141 Part1Karina MonasaNo ratings yet
- Use of FET-PET in Glioblastoma: Journal Club May 4 2011Document41 pagesUse of FET-PET in Glioblastoma: Journal Club May 4 2011tienloNo ratings yet
- Poster Session Topoisomerase I Inhibitors Friday 1 October 155Document1 pagePoster Session Topoisomerase I Inhibitors Friday 1 October 155JESUS DAVID BOLA‹O JIMENEZNo ratings yet
- Journal Reading Nasopharyngeal Carcinoma: Current Treatment Options and Future DirectionsDocument28 pagesJournal Reading Nasopharyngeal Carcinoma: Current Treatment Options and Future DirectionsyuliNo ratings yet
- tmpB2A TMPDocument9 pagestmpB2A TMPFrontiersNo ratings yet
- MedComm - 2024 - Yuan - Perioperative Immunotherapy the Main Clinical Treatment for Resectable Non‐Small Cell Lung CancerDocument4 pagesMedComm - 2024 - Yuan - Perioperative Immunotherapy the Main Clinical Treatment for Resectable Non‐Small Cell Lung CancerMihary RamanandraitsioryNo ratings yet
- Summary Table of Available Protocols in This Document: Institute Gene TargetsDocument80 pagesSummary Table of Available Protocols in This Document: Institute Gene TargetsGraha NusaNo ratings yet
- Difficulties With The Implemented Xpert MTBRIF For Determining DiagnosisDocument5 pagesDifficulties With The Implemented Xpert MTBRIF For Determining DiagnosisParluhutan DolliNo ratings yet
- Results of Proton ReirradiationDocument9 pagesResults of Proton ReirradiationJesse Helmut Hansen-BartelNo ratings yet
- 35 Newnew Esmo Breast Virtual 2021 Oliveira Upload v.2Document21 pages35 Newnew Esmo Breast Virtual 2021 Oliveira Upload v.2gaby andreaNo ratings yet
- Esmo 2020 Hendriks 021020Document27 pagesEsmo 2020 Hendriks 021020TaloipaNo ratings yet
- Summary Gynecology - 1Document29 pagesSummary Gynecology - 1Mohamad MostafaNo ratings yet
- Oppligerleibundgut 2012Document5 pagesOppligerleibundgut 2012HEARTJUGGLERNo ratings yet
- Armand Et Al. - 2013 - Detection of Circulating Tumour DNA in Patients With Aggressive B-Cell Non-Hodgkin Lymphoma PDFDocument4 pagesArmand Et Al. - 2013 - Detection of Circulating Tumour DNA in Patients With Aggressive B-Cell Non-Hodgkin Lymphoma PDFflashjetNo ratings yet
- Study Design: Condition or Disease Intervention/treatmentDocument36 pagesStudy Design: Condition or Disease Intervention/treatmentMihu DragostinNo ratings yet
- Therapeutic Journal Appraisal January 2020: Tadalafil more effective for BPH symptomsDocument4 pagesTherapeutic Journal Appraisal January 2020: Tadalafil more effective for BPH symptomsDaniel GarratonNo ratings yet
- Treatmentoftheprimary Tumorinanalcanal Cancers: Rob Glynne-Jones,, Sheela RaoDocument18 pagesTreatmentoftheprimary Tumorinanalcanal Cancers: Rob Glynne-Jones,, Sheela RaodanteyuriNo ratings yet
- Construction of A Reference Material Panel For Detecting Kras/Nras/Egfr/Braf/Met Mutations in Plasma CtdnaDocument7 pagesConstruction of A Reference Material Panel For Detecting Kras/Nras/Egfr/Braf/Met Mutations in Plasma Ctdnasylvi293No ratings yet
- F-18 NaFDocument47 pagesF-18 NaFLadipo Temitope AyodejiNo ratings yet
- Tuberculosis With Discordant Drug Resistance Patterns - A Diagnostic DilemmaDocument4 pagesTuberculosis With Discordant Drug Resistance Patterns - A Diagnostic DilemmaKevinNo ratings yet
- Prima Linea Di Trattamento: Roberto SabbatiniDocument40 pagesPrima Linea Di Trattamento: Roberto SabbatiniCHARMI JAINNo ratings yet
- 85 Jiang 2022 LucyDocument6 pages85 Jiang 2022 LucyJassa MaviNo ratings yet
- Molecular Minimal Residual Disease Detection in Acute Myeloid LeukemiaDocument42 pagesMolecular Minimal Residual Disease Detection in Acute Myeloid LeukemiaANo ratings yet
- Managing Colorectal Liver MetastasesDocument66 pagesManaging Colorectal Liver MetastasesFlaviusNo ratings yet
- Permenkes Tentang Penetapan Nilai KritisDocument34 pagesPermenkes Tentang Penetapan Nilai KritisMeutia sariNo ratings yet
- Biomarkers HER2+ MBCDocument30 pagesBiomarkers HER2+ MBChiroshima123No ratings yet
- Ukall Xii V4.1Document62 pagesUkall Xii V4.1Doc Javaria ChaudryNo ratings yet
- Contemporary Approach To The Diagnosis of Malignant Pleural EffusionDocument8 pagesContemporary Approach To The Diagnosis of Malignant Pleural EffusionranityaindraNo ratings yet
- High Risk Prostate Cancer: Comparison of Radical Prostatectomy Versus Radiation Therapy: Experience of Military Hospital RabatDocument6 pagesHigh Risk Prostate Cancer: Comparison of Radical Prostatectomy Versus Radiation Therapy: Experience of Military Hospital RabatIJAR JOURNALNo ratings yet
- WCLC2013 Alimta Final JB-1Document1 pageWCLC2013 Alimta Final JB-1Shru2611No ratings yet
- Systemic Therapies of CRC: Johan KurniandaDocument56 pagesSystemic Therapies of CRC: Johan KurniandaANISA RACHMITA ARIANTI 2020No ratings yet
- 2018 ESMO Preceptorship Breast Principles Breast Radiation Therapy Philip PoortmansDocument111 pages2018 ESMO Preceptorship Breast Principles Breast Radiation Therapy Philip PoortmansAna Sofia PintoNo ratings yet
- Cas 112 388Document9 pagesCas 112 388herdianNo ratings yet
- Jco 19 03136Document15 pagesJco 19 03136asdffdsaNo ratings yet
- Imaging Molecolare: Carcinoma Della Prostata: Nuove Evidenze Dallo Screening Alla TerapiaDocument20 pagesImaging Molecolare: Carcinoma Della Prostata: Nuove Evidenze Dallo Screening Alla TerapiaaxedemoNo ratings yet
- Clomiphene Citrate Improves Hormonal and Semen Parameters in Obese MenDocument1 pageClomiphene Citrate Improves Hormonal and Semen Parameters in Obese MenCătălin NechitaNo ratings yet
- Impower 132Document12 pagesImpower 132linxiaNo ratings yet
- Pi Is 0923753420431692Document14 pagesPi Is 0923753420431692adri20121989No ratings yet
- Fast Facts: Comprehensive Genomic Profiling: Making precision medicine possibleFrom EverandFast Facts: Comprehensive Genomic Profiling: Making precision medicine possibleNo ratings yet
- Blood 2020006028 PDFDocument13 pagesBlood 2020006028 PDFJosé Mauricio PeñalozaNo ratings yet
- Preguntas RealizadasDocument1 pagePreguntas RealizadasJosé Mauricio PeñalozaNo ratings yet
- The Top 5 Things You May Have Missed at SABCSDocument9 pagesThe Top 5 Things You May Have Missed at SABCSJosé Mauricio PeñalozaNo ratings yet
- Preguntas RealizadasDocument1 pagePreguntas RealizadasJosé Mauricio PeñalozaNo ratings yet
- Neoadjuvant breast cancer trials at SABCS 2013Document2 pagesNeoadjuvant breast cancer trials at SABCS 2013José Mauricio PeñalozaNo ratings yet
- Rules Update Guide 2015Document3 pagesRules Update Guide 2015José Mauricio PeñalozaNo ratings yet
- Comprehensive Hands On Course of Transnasal Skull Base Surgery Dec 2017Document4 pagesComprehensive Hands On Course of Transnasal Skull Base Surgery Dec 2017José Mauricio PeñalozaNo ratings yet
- Intracranial Neuroendoscopy 2017Document8 pagesIntracranial Neuroendoscopy 2017José Mauricio PeñalozaNo ratings yet
- 0504 NewsPath Breast Carcinoma MarkersDocument2 pages0504 NewsPath Breast Carcinoma MarkersJosé Mauricio PeñalozaNo ratings yet
- 217Document17 pages217José Mauricio PeñalozaNo ratings yet
- Colon Cancer:: Pfizer Headquarter Office. Wednesday 18/02/2015Document92 pagesColon Cancer:: Pfizer Headquarter Office. Wednesday 18/02/2015José Mauricio PeñalozaNo ratings yet
- Comprehensive Hands On Course of Transnasal Skull Base Surgery Dec 2017Document4 pagesComprehensive Hands On Course of Transnasal Skull Base Surgery Dec 2017José Mauricio PeñalozaNo ratings yet
- Management of Kaposi'S Sarcoma Associated With Human Immunodeficiency Virus InfectionDocument21 pagesManagement of Kaposi'S Sarcoma Associated With Human Immunodeficiency Virus InfectionJosé Mauricio PeñalozaNo ratings yet
- The Journal of Torah and Medicine of The Albert Einstein College of Medicine Synagogue and RIETSDocument160 pagesThe Journal of Torah and Medicine of The Albert Einstein College of Medicine Synagogue and RIETSoutdash2No ratings yet
- Insurance SalaoDocument16 pagesInsurance SalaoJohn Robert BautistaNo ratings yet
- SLE234 Lab Report 1Document3 pagesSLE234 Lab Report 1Wafaa AdamNo ratings yet
- 101 Rice FactsDocument13 pages101 Rice FactsrbmalasaNo ratings yet
- Trascendental Experience - RD LaingDocument5 pagesTrascendental Experience - RD LaingJosé LoschiNo ratings yet
- October 23, 2015 Strathmore TimesDocument28 pagesOctober 23, 2015 Strathmore TimesStrathmore TimesNo ratings yet
- Nursing Care Plan for Diverticulitis PatientDocument3 pagesNursing Care Plan for Diverticulitis PatientLeny GallardoNo ratings yet
- Herbal MedicinesDocument2 pagesHerbal MedicinesPrincess Gwyneth MartinezNo ratings yet
- ADL-12 (Business Law)Document6 pagesADL-12 (Business Law)samee380No ratings yet
- Exercise 14 - Isolation of Pure Culture.Document5 pagesExercise 14 - Isolation of Pure Culture.Chen JoshetteNo ratings yet
- NIH Low Iodine Diet For Nuclear MedDocument8 pagesNIH Low Iodine Diet For Nuclear MedderekcftamNo ratings yet
- Electroplating IndustryDocument5 pagesElectroplating IndustryRangasamyNo ratings yet
- Case Study (Uti)Document7 pagesCase Study (Uti)Ferreze AnnNo ratings yet
- Form 1 LGU Profile PDFDocument6 pagesForm 1 LGU Profile PDFArt Henrhey Bulic50% (2)
- Holistic Healing  " Sujok Therapy (PDFDocument24 pagesHolistic Healing  " Sujok Therapy (PDFDraghici Valentin80% (5)
- Houghton Hocut 795 - BDocument5 pagesHoughton Hocut 795 - BErwinNo ratings yet
- Education PreparationDocument17 pagesEducation Preparationpraveen praveen100% (2)
- Public Health Nutrition Career OptionsDocument2 pagesPublic Health Nutrition Career OptionsZaka RehmanNo ratings yet
- Best Practices in Health and NutritionDocument5 pagesBest Practices in Health and NutritionMary Rose Fernando AngelesNo ratings yet
- Research Time ManagementDocument39 pagesResearch Time ManagementArnel Belza Torrejas79% (14)
- Transparency Concerns Led To Energy Minister Change: Remembering An Uprising, 25 Years OnDocument88 pagesTransparency Concerns Led To Energy Minister Change: Remembering An Uprising, 25 Years OnThe Myanmar TimesNo ratings yet
- History of Oral SurgeryDocument17 pagesHistory of Oral SurgeryAnupama NagrajNo ratings yet
- Key Skills For Hospital DoctorsDocument3 pagesKey Skills For Hospital DoctorsMustafaNo ratings yet
- Surgical Infection PDFDocument20 pagesSurgical Infection PDFosaNo ratings yet
- Medicinal Plants For The Treatment of Nervios Anxiety and Depression in Mexican Traditional Medicine - 2014 - Revista Brasileira de Farmacognosia PDFDocument18 pagesMedicinal Plants For The Treatment of Nervios Anxiety and Depression in Mexican Traditional Medicine - 2014 - Revista Brasileira de Farmacognosia PDFGabriela OliveiraNo ratings yet
- Lembar Usg Iota Onkologi KebidananDocument1 pageLembar Usg Iota Onkologi KebidananAhmad NazharNo ratings yet
- Volume 48, Issue 49, December 5, 2014Document43 pagesVolume 48, Issue 49, December 5, 2014BladeNo ratings yet
- December IssueDocument104 pagesDecember Issuemiltonwcraft100% (1)
- Febuxostat EMEADocument51 pagesFebuxostat EMEAIndra PaqotzNo ratings yet