You might also like
- Disease Detectives Cheat Sheet PDFDocument2 pagesDisease Detectives Cheat Sheet PDFDevesh KhilnaniNo ratings yet
- USMLE Step 3 Lecture Notes 2021-2022: Internal Medicine, Psychiatry, EthicsFrom EverandUSMLE Step 3 Lecture Notes 2021-2022: Internal Medicine, Psychiatry, EthicsRating: 5 out of 5 stars5/5 (9)
- Types of ImmunizationsDocument21 pagesTypes of Immunizationsmacmactongos100% (6)
- HPV Efficacy Against Bacteria, Viruses and FungiDocument12 pagesHPV Efficacy Against Bacteria, Viruses and FungiAdamNo ratings yet
- Crop ProtectionDocument14 pagesCrop ProtectionWala LangNo ratings yet
- Second Thoughts About Viruses Vaccines and The HIV Part 2 Robert.O.YoungDocument5 pagesSecond Thoughts About Viruses Vaccines and The HIV Part 2 Robert.O.YoungDavidNo ratings yet
- STS Module-Gene TherapyDocument6 pagesSTS Module-Gene TherapyWinter SummerNo ratings yet
- Hiv - Aids MCQDocument7 pagesHiv - Aids MCQSp Ppv100% (2)
- Industrial Microbiology and BiotechnologyDocument36 pagesIndustrial Microbiology and BiotechnologyMyra Wardati SNo ratings yet
- Guidelines for Vaccination in Normal Adults in India - PMCDocument14 pagesGuidelines for Vaccination in Normal Adults in India - PMCSKMH INSURANCENo ratings yet
- Greenbook Chapter 7 Immunsing ImmunosupressedDocument8 pagesGreenbook Chapter 7 Immunsing Immunosupressedحسام الدين إسماعيلNo ratings yet
- Vaccine Timing CDCDocument40 pagesVaccine Timing CDCanindita.prasidha.parameswariNo ratings yet
- 1 CombineDocument726 pages1 CombineSong Hành Vạn KiếpNo ratings yet
- General Recommendation On ImmunizationDocument19 pagesGeneral Recommendation On ImmunizationRickyNoviantoNo ratings yet
- Summary of Recommendations For Adult Immunization: (Age 19 Years & Older)Document4 pagesSummary of Recommendations For Adult Immunization: (Age 19 Years & Older)gyna_2002No ratings yet
- Cohen 2008Document5 pagesCohen 2008Dee SobriNo ratings yet
- Post-Splenectomy Vaccine ProphylaxisDocument6 pagesPost-Splenectomy Vaccine ProphylaxisDavinPannaaustenNo ratings yet
- Adult Immunization Schedule and RecommendationsDocument3 pagesAdult Immunization Schedule and RecommendationsdrmanojvimalNo ratings yet
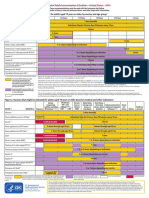
- Figure 1. Recommended Immunization Schedule For Adults Aged 19 Years or Older, by Vaccine and Age GroupDocument2 pagesFigure 1. Recommended Immunization Schedule For Adults Aged 19 Years or Older, by Vaccine and Age GroupmsarasNo ratings yet
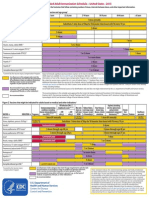
- Contraindications and Precautionary Conditions For VaccinatiDocument25 pagesContraindications and Precautionary Conditions For VaccinatikrishnasreeNo ratings yet
- Stay Healthy, Stay On Top of Vaccinations: CDC Click Here For The CDC's Full Vaccination ChartDocument4 pagesStay Healthy, Stay On Top of Vaccinations: CDC Click Here For The CDC's Full Vaccination ChartcircularreasoningNo ratings yet
- Jama Sha 2019 It 190019Document2 pagesJama Sha 2019 It 190019xtineNo ratings yet
- COVID-19 Vaccine Surveillance Report: Week 2Document55 pagesCOVID-19 Vaccine Surveillance Report: Week 2Kosta GavrasNo ratings yet
- Adult ImmunizationDocument6 pagesAdult ImmunizationAmit GoelNo ratings yet
- Adult Immunization Recommendations SummaryDocument5 pagesAdult Immunization Recommendations SummaryHannah Caburian RemoNo ratings yet
- Typhoid Fever Follow-Up PDFDocument16 pagesTyphoid Fever Follow-Up PDFPlot BUnniesNo ratings yet
- COVID-19 Vaccine Surveillance Report: Week 1Document54 pagesCOVID-19 Vaccine Surveillance Report: Week 1camaferNo ratings yet
- Adult Immunization ScheduleDocument3 pagesAdult Immunization ScheduleBryan Mae H. DegorioNo ratings yet
- Mourtzoukou Et Al-2008-British Journal of SurgeryDocument8 pagesMourtzoukou Et Al-2008-British Journal of SurgeryTony AdeosunNo ratings yet
- 60-Vaccination UpdatedDocument17 pages60-Vaccination UpdatedSeegah JoNo ratings yet
- HipomagnesenuaDocument32 pagesHipomagnesenuaAlbertoMarteNo ratings yet
- IMMUNIZATIONDocument35 pagesIMMUNIZATIONAkshay H.No ratings yet
- Immunogenesity & ImmunizationDocument7 pagesImmunogenesity & ImmunizationLoren SangalangNo ratings yet
- Atagi Recommendations On The Use of A Booster Dose of Covid 19 VaccineDocument9 pagesAtagi Recommendations On The Use of A Booster Dose of Covid 19 VaccinenickjoshNo ratings yet
- Clinical trial of self-administered influenza vaccineDocument34 pagesClinical trial of self-administered influenza vaccinevũ đình dũngNo ratings yet
- COVID-19 Vaccine Surveillance Report: Week 51Document53 pagesCOVID-19 Vaccine Surveillance Report: Week 51RicardoNo ratings yet
- Adult Pocafeket SizeDocument2 pagesAdult Pocafeket SizedadfNo ratings yet
- Who should get COVID vaccines firstDocument4 pagesWho should get COVID vaccines firstClaire FernandezNo ratings yet
- Adult ScheduleDocument3 pagesAdult SchedulelcmurilloNo ratings yet
- Varilrix SMPC JAN16Document10 pagesVarilrix SMPC JAN16TotochaNo ratings yet
- UKHSA Vaccine Surveillance Report Week 48Document47 pagesUKHSA Vaccine Surveillance Report Week 48Al StatiliusNo ratings yet
- Splenectomy - Factsheet - For - Health - Professionals 2022 FinalDocument4 pagesSplenectomy - Factsheet - For - Health - Professionals 2022 Finalalpha.blocker11No ratings yet
- Immunization and Prophylaxis: Childhood Immunization Has Reduced The Impact - Active Immunization Is TheDocument18 pagesImmunization and Prophylaxis: Childhood Immunization Has Reduced The Impact - Active Immunization Is TheCabdiNo ratings yet
- Are COVID Vaccines Effective for Immunocompromised PeopleDocument4 pagesAre COVID Vaccines Effective for Immunocompromised PeopleMARHUMA HAPSIN. ABBASNo ratings yet
- Government 211016 134210Document27 pagesGovernment 211016 134210KemNo ratings yet
- Epidemiology by Sahil KhanDocument33 pagesEpidemiology by Sahil KhanDikshant DaswatNo ratings yet
- Prospect Prevenar EnglezaDocument63 pagesProspect Prevenar EnglezaNicoleta CiobotarNo ratings yet
- Non Kepi Vaccines RevisedDocument28 pagesNon Kepi Vaccines Revisedokwadha simionNo ratings yet
- H Od M I A I N: Directed by Dr.J. Halazoun Presented By: Dr.Y. Abu ZanounaDocument33 pagesH Od M I A I N: Directed by Dr.J. Halazoun Presented By: Dr.Y. Abu ZanounaMarini SiagianNo ratings yet
- DR Swati Rajagopal - Adult VaccinationDocument50 pagesDR Swati Rajagopal - Adult VaccinationYabooNo ratings yet
- CDC Healthcare Personnel Vaccination RecommendationsDocument1 pageCDC Healthcare Personnel Vaccination RecommendationsdocktpNo ratings yet
- M M Rvaxpro ProspectDocument57 pagesM M Rvaxpro ProspectNicoleta CiobotarNo ratings yet
- 2020-04-18 3p Pediatric Convalescent PlasmaDocument20 pages2020-04-18 3p Pediatric Convalescent PlasmaCamilo VallejoNo ratings yet
- UK Vaccine Surveillance Report Week 42Document29 pagesUK Vaccine Surveillance Report Week 42Cam SlaterNo ratings yet
- Vaccination: Passive ImmunityDocument12 pagesVaccination: Passive ImmunityuouoNo ratings yet
- Preventing and Treating Infections in Children With Asplenia or HypospleniaDocument5 pagesPreventing and Treating Infections in Children With Asplenia or HypospleniaAmélieNo ratings yet
- COVID-19 Vaccine Surveillance Report: Week 3Document50 pagesCOVID-19 Vaccine Surveillance Report: Week 3FrankNo ratings yet
- Philippine COVID-19 Booster Guidelines SummarizedDocument35 pagesPhilippine COVID-19 Booster Guidelines SummarizedSherre Nicole CuentaNo ratings yet
- Vaccine Surveillance Report - Week 37 v2Document33 pagesVaccine Surveillance Report - Week 37 v2Abby EscorzaNo ratings yet
- Adult Combined ScheduleDocument6 pagesAdult Combined ScheduleAstrid Elaine RosalesNo ratings yet
- Vaccin OlogyDocument79 pagesVaccin Ologyhamzabinamjad987No ratings yet
- s12879 020 05656 6Document10 pagess12879 020 05656 6Marsya Yulinesia LoppiesNo ratings yet
- VaccinesDocument8 pagesVaccinesRaul MuresanNo ratings yet
- Evaluation and Prevention of Infections Associated With Biologic Agents and JAK Inhibitors in Adults - UpToDateDocument76 pagesEvaluation and Prevention of Infections Associated With Biologic Agents and JAK Inhibitors in Adults - UpToDatemayteveronica1000No ratings yet
- Pneumococcal Vaccination in AdultsDocument23 pagesPneumococcal Vaccination in AdultsIvelisse TaverasNo ratings yet
- Health Advice and Immunizations for TravelersFrom EverandHealth Advice and Immunizations for TravelersNo ratings yet
- Management of Infections in the Immunocompromised HostFrom EverandManagement of Infections in the Immunocompromised HostBrahm H. SegalNo ratings yet
- Prevalence of Dengue Viral Infections Among Febrile Patients in Mombasa County, KenyaDocument95 pagesPrevalence of Dengue Viral Infections Among Febrile Patients in Mombasa County, KenyaMuhammad AyazNo ratings yet
- UT Dallas Syllabus For Biol4v00.001.10s Taught by Mehmet Candas (Candas)Document8 pagesUT Dallas Syllabus For Biol4v00.001.10s Taught by Mehmet Candas (Candas)UT Dallas Provost's Technology GroupNo ratings yet
- Virus: Jump To Navigation Jump To SearchDocument2 pagesVirus: Jump To Navigation Jump To SearchAiko M TagabanNo ratings yet
- Therapy of Acute Respiratory Infections in Children: NoveltiesDocument11 pagesTherapy of Acute Respiratory Infections in Children: NoveltiesrizkaNo ratings yet
- Mechanism of Disease ResistanceDocument6 pagesMechanism of Disease ResistanceJiem PlazaNo ratings yet
- Pathology of InvertebratesDocument42 pagesPathology of InvertebratesAgnitaNo ratings yet
- 11th Biology Minimum Study Material emDocument39 pages11th Biology Minimum Study Material emJay senthilNo ratings yet
- PMC Paper 2022 PracticeDocument130 pagesPMC Paper 2022 PracticeMusharaf RehmanNo ratings yet
- Biology of Sars-Cov-2Document5 pagesBiology of Sars-Cov-2Nicole Sanchez100% (1)
- Lecture 12-Plant Virus-Vector Interactions-Circulative, PropagativeDocument11 pagesLecture 12-Plant Virus-Vector Interactions-Circulative, PropagativeSonicca ReyesNo ratings yet
- Nucleic AcidsDocument56 pagesNucleic AcidsShane G.No ratings yet
- Recombinant DNA Safety Guidelines - ANNEX - 5Document58 pagesRecombinant DNA Safety Guidelines - ANNEX - 5kunalkp88No ratings yet
- 0062 Vet VaccDocument6 pages0062 Vet VaccChimico ChimicoNo ratings yet
- Global Tekno Indonesia Provides Water ServicesDocument24 pagesGlobal Tekno Indonesia Provides Water Servicesgd sutawijayaNo ratings yet
- Viro 1Document6 pagesViro 1Elsa YuniaNo ratings yet
- Microbe and Animal InteractionDocument25 pagesMicrobe and Animal InteractionariNo ratings yet
- Why Do We Fall IllDocument6 pagesWhy Do We Fall IllMonika Mehan100% (10)
- Nicolas - Speech - Maintain Health and Productive During Pandemic Covid 19Document2 pagesNicolas - Speech - Maintain Health and Productive During Pandemic Covid 19Alan KrisnaNo ratings yet
- International Immunopharmacology: Akram Aminjafari, Sorayya Ghasemi TDocument4 pagesInternational Immunopharmacology: Akram Aminjafari, Sorayya Ghasemi TAmirNo ratings yet
- Assay Development and High-ThroughputDocument12 pagesAssay Development and High-ThroughputJuan AspilcuetaNo ratings yet
- BiomedPap - Bio 202003 0001Document9 pagesBiomedPap - Bio 202003 0001Edison Chiriboga OrtegaNo ratings yet
- "Snake Pneumonia" - Coronavirus Outbreak in China Traced To Snakes by Genetic AnalysisDocument10 pages"Snake Pneumonia" - Coronavirus Outbreak in China Traced To Snakes by Genetic Analysistd5xb7w4dpNo ratings yet
- Workshop Programme and Abstracts Workshop Programme and AbstractsDocument42 pagesWorkshop Programme and Abstracts Workshop Programme and AbstractshieucfavnNo ratings yet