You might also like
- Department of Consumer Affairs Notification of Name ChangeDocument2 pagesDepartment of Consumer Affairs Notification of Name ChangeJae ElkindNo ratings yet
- Cardiac Biomarkers Practice QuestionsDocument1 pageCardiac Biomarkers Practice QuestionsJae ElkindNo ratings yet
- Kade Chan - Fiery Dragon PDFDocument8 pagesKade Chan - Fiery Dragon PDFcoranus50% (6)
- Flight of The Bumblebee CziffraDocument7 pagesFlight of The Bumblebee CziffraIce level 9494% (16)
- Praying Mantis Robert LangDocument7 pagesPraying Mantis Robert LangJae ElkindNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- T Proc Notices Notices 035 K Notice Doc 30556 921021241Document14 pagesT Proc Notices Notices 035 K Notice Doc 30556 921021241Bwanika MarkNo ratings yet
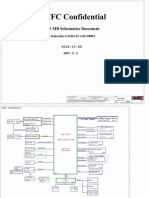
- Lenovo Legion Y920-17IKB LCFC-DS321 NM-B311 R 0.2 SchematicDocument61 pagesLenovo Legion Y920-17IKB LCFC-DS321 NM-B311 R 0.2 SchematicYetawa GuaviareNo ratings yet
- The Transmission of Prajnaparamita BuddhaDocument4 pagesThe Transmission of Prajnaparamita BuddhaFaith JunHaoNo ratings yet
- Vayu Issue Vayu Issue III May Jun 2018Document116 pagesVayu Issue Vayu Issue III May Jun 2018vs_3457000No ratings yet
- 7759 Cad-1Document2 pages7759 Cad-1Samir JainNo ratings yet
- Scout-Handbook Eng PDFDocument11 pagesScout-Handbook Eng PDFTai Nguyen DucNo ratings yet
- Unit Test 7A: 1 Choose The Correct Form of The VerbDocument4 pagesUnit Test 7A: 1 Choose The Correct Form of The VerbAmy PuenteNo ratings yet
- Accomplishment Report For The 2023 GSP Orientation and Update For Troop LeadersDocument6 pagesAccomplishment Report For The 2023 GSP Orientation and Update For Troop LeadersMarianne Hilario100% (1)
- Present SimpleDocument5 pagesPresent SimpleNghi PhuongNo ratings yet
- Launch Your Organization With WebGISDocument17 pagesLaunch Your Organization With WebGISkelembagaan telitiNo ratings yet
- Same Tractor Silver 80-85-90 105 160 180 Parts CatalogDocument17 pagesSame Tractor Silver 80-85-90 105 160 180 Parts Catalogalicebrewer210188ktm100% (64)
- HIE GLPsDocument6 pagesHIE GLPsWilson VerardiNo ratings yet
- Louis Vuitton: by Kallika, Dipti, Anjali, Pranjal, Sachin, ShabnamDocument39 pagesLouis Vuitton: by Kallika, Dipti, Anjali, Pranjal, Sachin, ShabnamkallikaNo ratings yet
- JhdsjkduijhsbsgdDocument3 pagesJhdsjkduijhsbsgdRanvidsNo ratings yet
- Civil 20procedure 20final PalsDocument185 pagesCivil 20procedure 20final PalsPaul EspinosaNo ratings yet
- The Effect of Big-Data On The HEC of ChinaDocument9 pagesThe Effect of Big-Data On The HEC of ChinaAbdulGhaffarNo ratings yet
- The IS - LM CurveDocument28 pagesThe IS - LM CurveVikku AgarwalNo ratings yet
- Key Area IIIDocument26 pagesKey Area IIIRobert M. MaluyaNo ratings yet
- George Moses Federal ComplaintDocument11 pagesGeorge Moses Federal ComplaintWXXI NewsNo ratings yet
- Mark The Letter A, B, C, or D On Your Answer Sheet To Indicate The Word(s) OPPOSITE in Meaning To The Underlined Word(s) in Each of The Following QuestionsDocument10 pagesMark The Letter A, B, C, or D On Your Answer Sheet To Indicate The Word(s) OPPOSITE in Meaning To The Underlined Word(s) in Each of The Following QuestionsPhạm Trần Gia HuyNo ratings yet
- Formation Burgos RefozarDocument10 pagesFormation Burgos RefozarJasmine ActaNo ratings yet
- Problem Set 1Document2 pagesProblem Set 1edhuguetNo ratings yet
- C-Profile Text - 2015 PT. Hydroraya Adhi PerkasaDocument11 pagesC-Profile Text - 2015 PT. Hydroraya Adhi Perkasadaniel_dwi_rahma100% (1)
- Network Protocol Analyzer With Wireshark: March 2015Document18 pagesNetwork Protocol Analyzer With Wireshark: March 2015Ziaul HaqueNo ratings yet
- TNCDA Monthly Journal NovemberDocument36 pagesTNCDA Monthly Journal Novemberrammvr05No ratings yet
- Alexandra Marotta Writing Sample 1Document3 pagesAlexandra Marotta Writing Sample 1api-315852783No ratings yet
- CH 04 Personal Safety and Social ResponsibilityDocument41 pagesCH 04 Personal Safety and Social ResponsibilityFirdauz RahmatNo ratings yet
- Resort Operations ManagementDocument15 pagesResort Operations Managementasif2022coursesNo ratings yet
- Pointers To Review For Long QuizDocument1 pagePointers To Review For Long QuizJoice Ann PolinarNo ratings yet
- ACCA - Generation Next - Managing Talent in Large Accountancy FirmsDocument34 pagesACCA - Generation Next - Managing Talent in Large Accountancy FirmsIoana RotaruNo ratings yet