Professional Documents
Culture Documents
Patient Placement Criteria
Uploaded by
Liliana Muñoz TiqueCopyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Patient Placement Criteria
Uploaded by
Liliana Muñoz TiqueCopyright:
Available Formats
Patient Placement Criteria
Linking Typologies to Managed Care
LESLIE C. MOREY, PH.D.
The proliferation of managed health care systems as a means of controlling rising health
care costs has stimulated efforts to subdivide the heterogeneous population of
alcoholics into more homogeneous subgroups based on their needs for specific levels
of treatment. The American Society of Addiction Bedicine (ASAB) has developed a set
of criteria aimed at helping clinicians select from four levels of care the one most
appropriate for each patient. The ASAB criteria are designed around six criteria
dimensions reflecting the severity of the patients' alcohol-related problems. Although
the ASAB criteria currently are the most widely used placement criteria for alcoholism
treatment and reimbursement, they also have been criticized in several respects.
Boreover, they still require outcome validation to ensure that application of the criteria
improves treatment outcome. K E Y WOR D S : problematic AOD use; patienttreatment
F
matching; patient care; managed care; patient assessment; disease severity; healt h
insurance; treatment cost; disorder classification
or many years, alcoholism treat alcoholrelated problems. Furthermore, treating alcohol and other drug (AOD)
ment providers predominantly as most researchers now believe that no abuse in both the private and public
sumed that people with drinking single form of treatment is effective sectors, the demand for specific types
problems1 were a homogeneous group for all people presenting with alcohol or levels of treatment (e.g., inpatient
that could be treated optimally with related problems (Hester and Miller detoxification or residential rehabili
only one treatment modality. This 1989). Consequently, alcohol researchers tation) now depends on more than just
modality involved inpatient care with now are conducting many studies de the patient’s wishes or the physician’s
a fixed length of stay and a treatment signed to determine what types of in perceptions of what the patient needs.
approach based on the 12step model terventions are most effective for what Patients now must meet utilization re
of Alcoholics Anonymous. In recent types of patients. This approach is view criteria set by the managed care
years, however, both assumptions— founded on the “matching hypothesis,” providers in order to be eligible for
that of patient homogeneity and treat which states that an optimal matching of treatment reimbursement. In addition
ment uniformity—have been abandoned. patients and treatments will produce the to controlling costs, the development
As the articles in this journal issue il greatest overall treatment effectiveness. of such criteria will enable health care
lustrate, researchers and clinicians now The need to acknowledge formally delivery systems to account for mean
recognize that problem drinkers are a the heterogeneity of treatment needs ingful and valid differences among
diverse group and differ substantially among people with alcoholrelated prob problem drinkers and to determine
in the causes and manifestations of their lems recently has received additional more accurately the mix of treatment
impetus from a direction unanticipated
In this article, the terms “people with drinking prob when the subtyping of alcoholics first LESLIE C. MOREY, PH.D., is a visiting
became popular—namely, from the associate professor of psychology at
1
lems” and “problem drinkers” refer to all individuals
whose alcohol consumption has caused them medical, proliferation of managed care systems Harvard Medical School, Boston, Mas
psychological, or social problems. These overarching
as a means of controlling health care sachusetts, and an associate professor
costs (see sidebar, p. 38.). With the of psychology at Vanderbilt University,
terms therefore encompass the more medical diagnoses
of alcohol abuse and alcohol dependence as defined by
the American Psychiatric Association. widespread use of managed care in Nashville, Tennessee.
36 ALCOHOL HEALTH & RESEARCH WORLD
services the patients need. Ultimately, preted cautiously, however, because
the improved match between patient the study also found that treatment
needs and the types of services avail completion rates were higher in the
able within the system will enhance inpatient program (95 percent) than in
the efficiency and effectiveness of the the outpatient program (72 percent).
alcoholism treatment system. This Thus, although the overall effec
matching process likely will focus on tiveness of inpatient care generally is
selecting specific treatment modalities accepted (Finney and Moos 1991;
rather than on the settings in which Walsh et al. 1991), concerns exist that
these modalities are provided. this more costly approach has been
Type II/type B alcoholism illustrated in “Skid
This article reviews the influences applied to many patients who did not
Row Bum.” Original artwork for “Temp
that led to the development of patient require this level of care. Moreover,
erance Tales and the Alcoholic,” 1979. Re
placement criteria as well as the process aside from the actual dollar costs of
produced with permission from the Journal
involved in designing such criteria. It treatment, other costs with potential
of Studies on Alcohol. © Alcohol Research
summarizes the placement criteria de clinical implications may be associated
Documentation, Inc., Rutgers University Center
veloped by the American Society of with inappropriate patienttreatment
of Alcohol Studies.
Addiction Medicine (ASAM), which matching. For example, inpatient care that represented the initial steps toward
currently are the most widely used cri disrupts the patient’s family life, em generating more widely applicable
teria, and presents both their advantages ployment, and social activities far more criteria for establishing treatment
and disadvantages. Finally, the article than does outpatient treatment. based typologies of problem drinkers.
describes the relationships of patient The increasing influence of managed The Northern Ohio Chemical Depen
placement criteria with typological ap health care also has greatly stimulated dency Treatment Directors Associ
proaches based on patient characteristics. patienttreatment matching considera ation developed a set of guidelines
tions. In particular, managed care pro known as the “Cleveland criteria”
viders introduced utilization reviews (Hoffman et al. 1987) that used rat
THE NEED FOR PATIENT that base treatment decisions on the ings in a variety of life areas to gauge
TREATMENT MATCHING patients’ abilities to meet certain cri the appropriateness of six levels of
teria. The requirement for such reviews care. These levels ranged from mutual
As researchers and clinicians began to selfhelp groups to medically managed
provided a significant challenge for
explore the heterogeneity of individuals intensive inpatient units. The second
the alcohol field, because until recently
with drinking problems, their interest in organization, the National Association
no criteria existed that had achieved
differences between the various modal of Addiction Treatment Providers
widespread acceptance. The need to
ities and settings for treating alcohol (NAATP), independently developed a
develop patient placement criteria
related problems also increased. One similar set of criteria (Weedman 1987).
prompted researchers, clinicians, and
issue that stimulated much discussion Many experts who were involved
service providers to examine more
concerned the merits of inpatient treat in developing these two criteria sets
closely existing alcoholism treatment
ment for alcoholrelated problems, and also participated in task forces estab
modalities and their appropriateness
several studies concluded that inpatient lished under ASAM’s direction. These
for various subgroups of people with
treatment programs for alcoholism were task forces developed a set of patient
drinking problems.
no more effective than formal outpa placement criteria that integrated and
tient programs (Miller and Hester revised various features of both the
1986; Annis 1986; Saxe and Good THE EVOLUTION OF PATIENT Cleveland criteria and the NAATP cri
man 1988). This conclusion forced PLACEMENT CRITERIA teria. These new guidelines, now called
the alcoholism treatment community to the ASAM criteria, were published by
reexamine many of the basic assump As managed care became increasingly ASAM in a volume entitled Patient
tions that for years had dominated popular for both publicly and privately Placement Criteria for the Treatment
treatment programs. funded alcoholism treatment, insurance of Psychoactive Substance Use Dis
The findings particularly raised companies and various State agencies orders (Hoffman et al. 1991). The cri
questions about the costeffectiveness began to establish criteria to determine teria provide guidelines not only for
of prevailing treatments. For example, the appropriate placement or level of alcoholism treatment but also for other
Hayashida and colleagues (1989) dem care for AOD abusers. These standards forms of drug abuse and dependence.
onstrated that inpatient detoxification of differed widely, however, and were
patients with mild to moderate features often kept secret to prevent providers
The ASAM Criteria
of alcohol withdrawal was no more ef from slanting patient information in an
fective than outpatient detoxification effort to obtain more favorable out The ASAM criteria were developed
but costed approximately 10 times comes during utilization review. In 1987 from numerous and widely dissemi
more. These results should be inter two organizations published guidelines nated drafts and revisions and were
VOL. 20, NO. 1, 1996 37
MANAGED HEALTH CARE
The rapid development of managed One outgrowth of this movement control often is accomplished through
care systems has resulted in sweeping was a major shift in the financing of utilization reviews that include pre
changes in the U.S. health care system, health care. In many cases, individual admission certification of patients for in
including alcoholism treatment. Although feeforservice payments were replaced patient care and concurrent reviews of
the forerunners of such systems date by one prepayment covering services patients in inpatient/residential care (and
back to the 1920’s (MacLeod 1993), the provided to each subscriber in the sys sometimes outpatient care) to determine
modern development of managed care tem for a specified period. This process whether the particular level of care is
accelerated during the 1970’s, stimu is known as “capitation.” Under these medically necessary. This process re
lated by the private sector in response new plans, health care providers had to quires using placement criteria that
to years of unchecked inflation in health bear part of the financial risk in provid clearly specify the requirements that pa
care costs and by widespread resistance ing services—for example, if providers tients must meet to be admitted to the
to the concept of a national health in incurred expenses exceeding the budg various levels of care offered within the
surance. The passage of both the Health eted estimates, they had to absorb the program. This requirement for placement
Maintenance Organization Act in 1973, deficit. This financing structure pro criteria, however, significantly chal
which required minimal benefits for vided strong incentives to reduce hospital lenges the alcohol field, because to date
alcohol and other drug abuse treatment, care and shift services to less expensive no universally accepted criteria exist.
and subsequent amendments facilitated outpatient settings. —Leslie C. Morey
the expansion of the corporate practice The term “managed” in “managed
of medicine. Large enrollment health care” refers in part to the control that
care programs developed through new payers (i.e., insurance companies or REFERENCE
means of financing. These programs health maintenance organizations) exert
proliferated, with the expectation that over health care decisions (e.g., which MacLeod, G.K. An overview of managed health
competition between different programs services an individual patient should care. In: Kongstvedt, P.R., ed. The Managed
would help contain health care costs use) in an effort to contain costs while Health Care Handbook. Gaithersburg, MD:
with minimal government intervention. ensuring adequate quality of care. This Aspen Publishers, 1993.
evaluated in field tests at 15 different nonresidential services or office fered in permanent facilities with
sites (MeeLee 1993). The primary goal practices in permanent facilities inpatient beds, include a planned
of the criteria was to provide a common with designated addiction treat regimen of roundtheclock profes
language for both providers and payers ment personnel who provide pro sionally directed evaluation, care,
when determining the severity of a pa fessionally directed evaluation, and treatment for addicted patients
tient’s problems, the different levels treatment, and recovery services provided by designated addiction
or settings of the treatment modalities to addicted patients. The services personnel. The treatment is specific
offered, and the criteria for patient are provided in regularly scheduled to AOD abuse and does not require
placement within the continuum of sessions of usually fewer than the full resources of an acutecare
AOD treatment. These criteria not only 9 hours per week. general hospital.
described patient characteristics that • Level II: Intensive outpatient and
might warrant inpatient care but also • Level IV: Medically managed in
partial hospitalization treatment. In patient treatment. This level of care,
provided guidelines for different types these settings, an organized service
of outpatient treatment and outlined the which also is administered by de
with designated addiction personnel signated addiction professionals,
process of moving across different provides a planned treatment regi
levels of care. provides a roundtheclock planned
men consisting of regularly sched
The ASAM system is built around regimen of medically directed eval
uled sessions of at least 9 hours per
criteria dimensions that are used to uation, care, and treatment for ad
week within a structured program.
place patients in one of four levels of dicted patients in an acutecare
This level of care affords patients
care originally presented in an Institute inpatient setting. Such a service
the opportunity to interact with the
of Medicine report (1990) describing realworld environment while still requires permanent facilities that
transitions in the alcoholism treat benefiting from a programmatically include, at a minimum, inpatient
ment field. The four levels of care are structured therapeutic milieu. beds. A multidisciplinary staff and
as follows: the full resources of a general hos
• Level III: Medically monitored pital are available to provide treat
• Level I: Outpatient treatment. inpatient (residential) treatment. ment for patients with severe acute
Such settings include organized These modalities, which are of problems necessitating primary
38 ALCOHOL HEALTH & RESEARCH WORLD
Patient Placement Criteria
medical and nursing services. Treat care. Moreover, problem drinkers ex and social environment contribute to
ment is specific to AODuse disor hibiting signs of an imminent risk of relapse potential. This dimension ad
ders, although the available support harming themselves (e.g., attempting dresses the personal factors that influ
services allow concurrent treat to commit suicide) or others may re ence the extent to which people can
ment of coexisting acute biomedi quire 24hour monitoring, thus justify control their environments. (Environ
cal and emotional conditions. ing a higher level of clinical care. The mental factors are addressed in di
same holds true for problem drinkers mension 6.) Accordingly, when these
Under the ASAM guidelines, pa whose mental status does not allow elements impede a patient’s control
tients are assigned to the four levels them to understand the nature of the over his or her behavior in the current
of care after being evaluated along six disorder or the treatment process. environment, a higher level of care
criteria dimensions reflecting the sever (e.g., a halfway house rather than out
Dimension 4: Treatment
ity of the patients’ problems. Each di patient care) may be justified to mini
Acceptance/Resistance. Patients in
mension contains several criteria, and mize the relapse risk. For example, if a
alcoholism treatment vary greatly in
the number of specific criteria that must patient experiences marked and per
their willingness to comply with treat
be met depends on the level of care. sistent cravings for alcohol and thus
ment regimens. Patients who seek
These six dimensions are described in has higher relapse potential, treatment
treatment and cooperate by following
the following paragraphs. success may be less likely in an outpa
clinical instructions typically require
Patients are
Dimension 1: Acute Intoxication tient than in an inpatient setting.
and/or Withdrawal Potential. The Dimension 6: Recovery Environ
assigned to the
ASAM criteria assume that a person ment. The patient’s environment can
who is acutely intoxicated cannot be facilitate recovery or increase the risk
four levels of
monitored adequately as an outpatient of relapse. When the social setting is
and should receive more intensive care. supportive (e.g., family members and
When assessing withdrawal potential,
one of the most important considera care after being friends agree with and encourage re
evaluated along six
covery) or the patient seeks out social
tions is whether the patient is at risk surroundings that discourage alcohol
of experiencing lifethreatening with
criteria dimensions.
abusing behavior patterns, a lower level
drawal symptoms or requires medica of clinical care may be justified. How
tion or other support services to cope ever, when a recovering person’s social
with or reduce the discomfort of with setting is compromised—for example,
drawal, which otherwise might cause a lower level of care. However, alco by inadequate transportation to the
him or her to terminate treatment. hol dependence often compromises a treatment provider, a higher level of
Dimension 2: Biomedical Condi person’s capacity to cooperate with family stress, or friends and cowork
tions or Complications. Higher levels treatment protocols. Patients often ers who regularly use alcohol—a
of care are indicated when continued present for treatment with some level higher level of care may be required.
AOD use would put the patient in dan of understanding that alcohol is re Table 1 summarizes the correlations
ger of health complications. For ex sponsible for their alcohol problems between the treatment settings and
ample, an alcoholdependent woman but are still unwilling to participate in criteria dimensions specified by the
who is pregnant might benefit from a the clinical process. Other patients may ASAM guidelines. The actual criteria
higher level of care. Similarly, problem deny that they have a drinking problem. for placing an individual into a given
drinkers with cardiovascular, liver, or Thus, some problem drinkers may be level of care vary according to the care
gastrointestinal diseases requiring med unlikely to enter the treatment system level, and placement ultimately de
ical monitoring or treatment should without first receiving some form of pends on the combination of patient
receive a higher level of care. therapeutic preparation directed at characteristics in the six assessment
Dimension 3: Emotional and addressing their denial and their resis dimensions. For example, treatment
Behavioral Conditions and Compli tance to treatment. Under these condi in an outpatient setting (i.e., level I)
cations. A wide range of emotional tions, a high level of clinical care may requires that the patient meets level I
and behavioral conditions and com be appropriate. criteria in all six assessment dimen
plications exist in problem drinkers, Dimension 5: Relapse Potential. sions, whereas treatment in an inpa
either as manifestations of alcohol Because alcoholrelated problems in tient setting (i.e., level III or IV)
abuse or as independent, coexisting volve recurrent patterns of behavior, requires that the patient meets the
psychiatric disorders. These conditions relapse is a frequent and integral part corresponding severity criteria in at
(e.g., debilitating anxiety, guilt, or de of the natural history of the disorder. least two of the six dimensions. Fur
pression) deserve special attention Two major sets of factors that derive thermore, not all dimensions are rele
during treatment and therefore may from the patient’s personal (i.e., psy vant to all placement decisions. For
necessitate a higher level of clinical chological and biological) background example, treatment resistance, relapse
VOL. 20, NO. 1, 1996 39
Table 1 Summary of the ASAM1 Criteria Dimensions of Assessment
Level II: Intensive Level III: Medically Level IV: Medically
Criteria Level I: Outpatient Outpatient or Partial Monitored Inpatient Managed Inpatient
Dimension Treatment Hospitalization Treatment (Residential) Treatment Treatment
Acute Minimal to no risk of Minimal risk of severe with Risk of severe but manage Risk of severe withdrawal;
Intoxication/ severe withdrawal; drawal; will enter detoxifica able withdrawal, or has detoxification requires fre
Withdrawal will enter detoxification tion if needed and responds failed detoxification at lower quent monitoring.
Potential if needed. to social support when com levels of care.
bined with treatment.
Biomedical None or noninterfering May interfere with treatment Continued use means imminent Complications (e.g., recur
Conditions with treatment. but patient does not require danger, or complications or rent seizures or disulfiram
inpatient care. other illness requires medical reactions) that require
monitoring. medical management.
Emotional/ Some anxiety, guilt, or Inability to maintain behav Symptoms require structured Uncontrolled behavior,
Behavioral depression related to ioral stability, abuse/neglect environment, moderate risk of confusion/disorientation, ex
Conditions abuse, but no risk of of family, or mild risk of harm harm to self or others, or treme depression, thought
harm to self or others. to self or others. history of violence during disorder, or alcohol
Mental status permits intoxication. hallucinosis/psychosis.
treatment comprehen
sion and participation.
Treatment Willing to cooperate Attributes problems exter Does not accept severity of Any difficulties noted in
Acceptance/ and attend treatment; nally; not severely resistant. problems despite serious levels I, II, or III.
Resistance admits problem. consequences.
Relapse Able to achieve goals Deteriorating during level I Deteriorating and in crisis Any difficulties noted in
Potential with support and ther treatment, or will drink with during outpatient care, or at levels I, II, or III.
apeutic contact. out close monitoring and tempts to control drinking
support. without success.
Recovery Supportive social en Current job environment dis Environment disruptive to Any difficulties noted in
Environment vironment or motivated ruptive, family/support sys treatment, logistic impedi levels I, II, or III.
to obtain social support. tem nonsupportive, or lack ments to outpatient care, or
of social contacts. occupation places public at
risk if patient continues to drink.
1
ASAM = American Society of Addiction Medicine.
potential, and recovery environment substance abuse counselors. Perhaps eligibility. Thus, the ASAM criteria
are not used to distinguish between because of this comprehensive input, are among the few treatmentmatching
patients requiring level III and level the dimensions composing the criteria guidelines flexible enough to respond
IV care. relate to actual patient dispositions as to changes in a patient’s status during
well as to treatment dropout (Gastfriend the course of treatment.
et al. 1995). Second, the criteria have Although the ASAM criteria cur
ADVANTAGES AND DISADVANTAGES achieved much national visibility, far rently are the most widely used pa
OF THE ASAM CRITERIA exceeding the impact of other criteria tient placement criteria for treatment
sets. Third, the ASAM guidelines sep and reimbursement in the addiction
The ASAM criteria have become the arately consider factors influencing field, they also have been criticized in
most widely distributed and discussed care for adults and for adolescents. several respects (Book et al. 1995;
criteria available, and several States This is important because the social Gartner and MeeLee 1995). For ex
have used them or some of their adap factors associated with a need for ample, relatively few studies to date
tations as guidelines for patient place higher treatment intensity may vary have assessed the validity of the ASAM
ment and medicaid reimbursement. depending on age. Finally, the criteria criteria, and although relevant projects
Many aspects of the ASAM criteria specify guidelines for a broader con currently are under way, no evidence
make them reasonably well suited for tinuum of care than traditionally found yet exists that matching patients to
such use. First, the criteria were de treatments based on the ASAM criteria
in the alcoholism treatment field. For
veloped by a multidisciplinary con actually improves treatment outcome.
example, the criteria include guide
In the most relevant study, McKay
sensus group, including physicians, lines for continued treatment at each
and colleagues (1992) examined the
social workers, psychologists, and level of care as well as for discharge
40 ALCOHOL HEALTH & RESEARCH WORLD
Patient Placement Criteria
validity of the Cleveland criteria, which marked resistance to treatment) would did not meet the ASAM criteria for
were a precursor to the ASAM guide impair their ability to benefit from ex either outpatient treatment, because of
lines. The researchers studied alco pensive residential treatments. Conse their potentially complicated detoxifi
holic and cocainedependent patients quently, these writers recommend that cation, or inpatient treatment (i.e., level
who were treated in a day treatment individuals who either are not yet ready III), which require problems in at least
program (i.e., ASAM level II). As for such treatments or not able to real two of the six domains. Consequently,
sessment according to the Cleveland ize the benefits of residential treatment these patients were excluded from both
criteria revealed that 76 percent of be treated in less expensive settings, outpatient and inpatient care.
these patients should have been as such as halfway houses.
signed to inpatient rehabilitation (i.e., Other critics of the ASAM guide
level III). The assumptions underlying lines have noted significant conceptual RELATIONSHIPS OF PATIENT
the ASAM criteria would predict that and empirical gaps in the criteria, such PLACEMENT CRITERIA TO OTHER
patients who were “mismatched” to as the lack of provisions for prevention TYPOLOGICAL APPROACHES
Large alcoholism
the level of care they received should
have had poorer outcomes than those Unlike most of the earlier alcoholism
treatment “campuses”
who were appropriately matched. How typologies that were based on patient
ever, the study found no differences characteristics, the typologies inspired
might deliver
in outcomes between matched and mis by the managed care movement focus
matched patients. Although the mis on service systems. In other words, the
matched group drank slightly more different types of traditional approach to subtyping people
with drinking problems has involved
services all with
frequently than the matched group be
fore they entered treatment—consistent identifying presumably fundamental
in one setting.
with the conclusion that severity of differences among problem drinkers,
problem drinking is related to patient followed by attempts to identify the
placement decisions resulting from most effective treatment for each sub
the application of these criteria—the type. In contrast, the managed care
two groups did not differ significantly and/or early intervention efforts (Gart inspired typologies have focused on
in their frequency of alcohol use after ner and MeeLee 1995). Moreover, the critical differences between the vari
4 or 7month followup. Overall, all criteria do not cover several “sublevels” ous forms of treatment, with a partic
subjects appeared to respond well to within each ASAM level. For example, ular emphasis on the costs of different
treatment regardless of whether they intensive outpatient treatment and par treatment approaches. In the interests
were matched or mismatched accord tial hospitalization (both regarded as of costcontainment and optimal allo
ing to patient placement criteria. ASAM level II) clearly differ in terms cation of resources, managed care has
McKay and colleagues (1992) con of treatment intensity. Similarly, half sought to develop patient placement
cluded that the Cleveland criteria may way houses, therapeutic communities, criteria that restrict the most expen
be overinclusive in identifying patients and shortterm intensive rehabilitation sive forms of treatment—particularly
who require inpatient treatment. Simi centers, which all can be considered inpatient services—to those patients
lar criticism has been raised against residential treatment programs (i.e., who need them. The resulting subtyp
the ASAM criteria, in part because the ASAM level III), may vary widely in ing strategy is treatment driven and
continuum of care represented in these terms of treatment intensity. typically arranged around treatment
guidelines does not include some im Other gaps involve patient types intensity. Consequently, these typolo
portant alternatives to traditional in rather than types of treatment settings. gies often bear little resemblance to
patient care (e.g., halfway houses or For example, Morey (1995) found that the typologies described elsewhere in
therapeutic communities). Other re after strict application of the ASAM this journal issue.
searchers have expressed concerns that criteria, as many as 13 percent of in The common denominator under
the ASAM criteria overemphasize the dividuals who met the criteria of the lying patient placement typologies as
medical elements of treatment and con Diagnostic and Statistical Manual of well as many other patientbased ty
sistently place patients in higher levels Mental Disorders, Third Edition, Re pologies is general problem severity.
of care than needed (Book et al. 1995). vised (DSM–III–R) for alcohol abuse Although the ASAM criteria them
The ASAM criteria also have been or dependence did not meet the criteria selves are multidimensional, the types
criticized for assuming that a linear re for any of the four levels specified by of problems described across the six
lationship exists between the severity ASAM. For instance, the ASAM guide dimensions tend to be interrelated, and
of the alcoholrelated problems and the lines commonly failed to include prob most studies demonstrate significant
treatment level needed. For example, lem drinkers who were at risk for a correlations between the level of care
Book and colleagues (1995) indicate problematic withdrawal but manifested recommended according to the ASAM
that in some patients, very severe prob no other biological, emotional, or psy guidelines and global problem severity.
lems (e.g., cognitive impairment or chosocial complications. These people For example, McKay and colleagues
VOL. 20, NO. 1, 1996 41
(1992) found a greater degree of psy
chological disturbance as measured by
the Addiction Severity Index among
Mean Number of Alcohol-Dependence Features
7
patients identified as needing inpatient
treatments than among those suited for
outpatient treatment.
6
In a study assessing the applicability
of the ASAM criteria in a community
5
sample, Morey (1995) used the guide
lines to estimate level of care needs in a
4
household survey of more than 18,000
people, roughly 6.5 percent of whom
3
met the DSM–III–R diagnostic criteria
for current alcohol abuse or dependence.
2
The study related the number of alco
hol dependence criteria met by the re
1
spondents (out of a possible nine) to
the ASAM care levels that would have
been assigned to these people. The re
0
sults demonstrated that the number of
Outpatient Treatment Intensive Outpatient Medically Monitored Medically Managed
or Partial Inpatient Treatment Inpatient Treatment
dependence features reported by re
Hospitalization
spondents who would have been as
Treatment
signed to inpatient treatments was
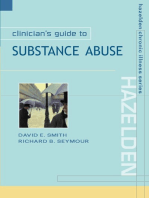
Figure 1 The correlation between the level of care of alcoholism treatment and the
considerably greater than for respon
severity of the patients’ alcohol dependence. Based on telephone inter-
dents who would have been assigned
views with approximately 1,150 subjects from a community sample who
to outpatient treatment (figure 1). In
met the criteria of the Diagnostic and Statistical Manual of Mental Disorders,
fact, the respondents identified as
Third Edition, Revised (DSM–III–R) for alcohol abuse and dependence,
the researchers assessed the subjects’ severity of alcohol dependence and
needing intensive hospital care (i.e.,
the level of care 1 that they should receive during treatment. Dependence
ASAM level IV) on average fulfilled
severity was indicated by the mean number of DSM–III–R criteria (of which
severity
nearly seven DSM–III–R criteria, in
nine were possible) that the subjects met.
dicating severe dependence according
to that diagnostic scheme.
1Level of care was determined according to the guidelines established by the American
American Society of
Addiction Medicine.
The ASAM criteria’s focus on
F = 38.14, p < 0.001.
global problem severity when making
SOURCE: Adapted from Morey 1995.
placement decisions emphasizes quan these dependence problems can pre (For more information on this typology
titative differences among problem dict relapse as well as posttreatment and how it was derived, see the article
drinkers (i.e., people with more severe craving in abstinent individuals (Babor by Allen, pp. 24–29.) This typology
problems require greater treatment in et al. 1988). This dimensional approach distinguishes three types of people with
tensity). Many of the other alcoholism also forms the basis of the DSM–III–R drinking problems: lateonset problem
typologies, in contrast, have focused definition of alcoholdependence syn drinkers, affiliative/impulsive alcoholics,
on qualitative differences (e.g., Clon drome with its subdivisions of mild, and isolative/anxious alcoholics. The
inger’s type I versus type II classifi moderate, and severe forms. Subtyping lateonset problem drinkers demon
cation or Babor’s type A versus type alcoholics along a continuum of alcohol strate significant signs of alcohol abuse
B classification; for more information dependence severity therefore will but develop only mild manifestations
on these other typologies, see the arti capture many important differences of the alcoholdependence syndrome.
cles by Babor, pp. 6–14, and by Clon among people with drinking problems. According to the ASAM criteria, nearly
inger and colleagues, pp. 18–23). A An exclusive focus on dependence all these patients could be treated in
review of the literature justifies care severity, however, may overlook critical outpatient programs. Lateonset problem
ful consideration of the quantitative ap qualitative differences among problem drinkers differ quantitatively in their
proach, which dates back to Jellinek’s drinkers that might assist in tailoring problem severity from the affiliative/
four phases in the development of al treatment approaches, particularly those impulsive and isolative/anxious alco
coholism that fell along a severity con offered within a given level of care. holics, who both are at an advanced
tinuum (Jellinek 1962). Subsequent To avoid such a onesided focus, level of alcohol dependence. Con
research has supported the contentions Morey and colleagues (1984) developed versely, the latter two types differ
that features of alcohol dependence the “hybrid” model, combining the qualitatively from each other with re
tend to form a unidimensional scale quantitative and qualitative models of spect to interpersonal style, personality
and that the cumulative severity of alcoholrelated problems (figure 2). traits, concomitant symptoms of mental
42 ALCOHOL HEALTH & RESEARCH WORLD
Patient Placement Criteria
therefore suitable for patients with
greater problem severity.
A review of the current status of pa
tient placement criteria by a consensus
panel organized by the Center for Sub
ALCOHOL USE
tance Abuse Treatment (CSAT) sug
Severity of Alcohol-Dependence Syndrome
gested that the future acceptance of
uniform patient placement criteria will
hinge on several critical issues (Gartner
Type A:
Late-onset problem drinkers
and MeeLee 1995):
• The criteria should accurately reflect
the different levels of care available.
• The criteria should have documented
validity regarding recommended
Type B: placement levels.
• The criteria should be easy to use in
Affiliative/impulsive alcoholics
daytoday clinical decisionmaking.
• The criteria should be measurable
using reliable and objective tools.
Type C:
• The criteria should encourage
Isolative/anxious alcoholics
positive treatment outcomes by
recommending treatments in the
Figure 2 The hybrid model of alcoholic subtypes. This model distinguishes three
least restrictive environments.
categories of alcoholics: late-onset problem drinkers, affiliative/impulsive
alcoholics, and isolative/anxious alcoholics. Late-onset problem drinkers
• The criteria should optimally match
differ
differ in the severity of alcoholism (i.e., quantitatively) from drinkers in the
patients to specific treatment modal
other two categories. Affiliative/impulsive alcoholics and isolative/anxious
ities and levels of care.
alcoholics differ in certain personal characteristics (i.e., qualitatively) from
each other.
The last point is particularly im
portant because it addresses what is
SOURCE: Adapted from Morey et al. 1984.
disorder, and specific features of their new development in a rapidly evolv perceived as the inflexibility of current
alcohol use. Consequently, although ing field. Although the ASAM cri patient placement criteria. The CSAT
both affiliative/impulsive alcoholics teria have been disseminated widely in panel recommended to “unbundle” the
and isolative/anxious alcoholics man the 5 years since their publication, they guidelines for the modality and inten
ifest severe dependence problems that have not been uniformly accepted in sity of treatment from the setting in
likely necessitate relatively intensive either the public or private service de which treatment is provided. Un
treatment, they respond differently to livery sector. Several States have re bundling means that the type and in
the various elements of intensive treat vised the criteria to include treatment tensity of treatment are based more on
ment (e.g., group therapy as opposed modalities that are not well covered the patient’s needs than on the setting
to individual counseling) (Morey and by the ASAM guidelines (e.g., meth in which they are provided; thus, psy
Jones 1992). The hybrid model provides adone maintenance for treating heroin chiatric consultation could be offered
one example of how patientbased ty addiction). Furthermore, the patient in outpatient as well as inpatient set
pologies can be integrated with the placement criteria used by managed tings, or intensive outpatient treatment
servicedriven considerations that pro care companies tend to be more re could be offered in conjunction with a
vide the foundation of patient place strictive than the ASAM guidelines halfwayhouse setting. For example,
ment typologies. regarding access to the more intensive large alcoholism treatment “campuses”
levels of care (Book et al. 1995). These might deliver different types of ser
CURRENT STATUS OF PATIENT companies also typically separate the vices all within one setting. Similarly,
PLACEMENT CRITERIA level II services outlined in the ASAM McGee (1995) has described a “human
criteria, with partial hospitalization service matrix” in which the intensity
The use of criteria, such as the ASAM regarded as more intensive treatment of social support services needed (e.g.,
standards, for guiding patients into dif with more extensive patient contact housing needs, child care, community
ferent forms of treatment is a relatively than intensive outpatient programs and support services, and occupational or
VOL. 20, NO. 1, 1996 43
legal assistance) is considered indepen need treatments of similar intensity but HOFFMAN, N.G.; HALIKAS, J.A.; AND MEELEE, D. The
dently of the intensity of the clinical with differing emphases. The literature Cleveland Admission, Discharge, and Transfer Criteria:
services provided (e.g., counseling or on the subtyping of alcoholics includes
Model for Chemical Dependency Treatment Programs.
Cleveland: Northern Ohio Chemical Dependency Treat
psychotherapy, nursing, or biomedical numerous typologies that have assem ment Directors Association, 1987.
interventions). Separating some of the bled impressive evidence of validity.
elements that appear inherently included Ultimately, managed care may repre
HOFFMAN, N.G.; HALIKAS, J.A.; MEELEE, D.; AND
WEEDMAN, R.D. Patient Placement Criteria for the
in prevailing views of certain treatment sent a means by which typologies dem Treatment of Psychoactive Substance Use Disorders.
settings would allow a much greater onstrating validity in the realm of Washington, DC: American Society of Addiction Med
matching of specific interventions to treatment outcome can substantially icine, 1991.
different types of individual problems. influence alcoholism treatment prac Institute of Medicine. Broadening the Base for Treat
tices in this country. ■ ment of Alcohol Problems. Washington, DC: National
Academy Press, 1990.
CONCLUSIONS
REFERENCES
JELLINEK, E.M. Phases of alcohol addiction. In: Pittman,
Managed care undoubtedly has changed
D.J., and Snyder, C.R., eds. Society, Culture, and Drink
ing Patterns. New York: Wiley, 1962. pp. 356–368.
the alcoholism treatment field dramat ANNIS, H.M. Is inpatient rehabilitation of the alcoholic
ically, and its influence will likely only cost effective? A composition. Advances in Alcohol MCGEE, M.D. Interagency collaboration: Improving
increase in the near future. Although ism and Substance Abuse 5:175–190, 1986. outcomes in the treatment of addictions. Directions in
many concerns have been voiced about
Substance Abuse Counseling 3:2–10, 1995.
BABOR, T.; COONEY, N.; HUBBARD, R.; JAFFE, J.; KOSTEN,
the effects of managed care on treat T.; LAUERMAN, R.; MCLELLAN, T.; RANKIN, H.; ROUN MCKAY, J.R.; MCLELLAN, A.T.; AND ALTERMAN, A.I.
ment, this new form of health care SAVILLE, B.; AND SKINNER, H. The syndrome concept of An evaluation of the Cleveland criteria for inpatient
delivery presents extraordinary oppor
alcohol and drug dependence: Results of the secondary treatment of substance abuse. American Journal of
analysis project. In: Harris, L.S., ed. Problems of Drug Psychiatry 149:1212–1218, 1992.
tunities for research results to directly Dependence, 1987: Proceedings of the 49th Annual
affect clinical practice. Managed care
MEELEE, D. Patient placement criteria for chemical
Scientific Meeting, The Committee on Problems of
offers strong incentives to match pa
dependency: Progress toward validation. Behavioral
Drug Dependence, Inc. National Institute of Drug
Healthcare Tomorrow 28–31, 1993.
tients with alcohol problems to the Abuse Research Monograph No. 81. Rockville, MD:
appropriate levels and types of treat
the Institute, 1988. pp. 33–39. MILLER, W.H., AND HESTER, R.K. Inpatient alcohol
ment services, a goal that alcohol re
ism treatment: Who benefits? American Psychologist
BOOK, J.; HARBIN, H.; MARQUES, C.; SILVERMAN, C.;
41:794–805, 1986.
searchers have been striving to attain LIZANICHARO, S.; AND LAZARUS, A. The ASAM and
for the past two decades. Inherent in
Green Spring alcohol and drug detoxification and re MOREY, L.C. “Epidemiological Assessment of Patient
this movement will be a greater em
habilitation criteria for utilization review. American Placement Criteria for Substance Abuse Treatment.”
Journal on Addictions 4:187–197, 1995. Paper presented at the meeting of the International
phasis on evaluating outcome in differ Conference on Health Policy Research, Boston, MA,
ent treatments. The array of data that
FINNEY, J.W., AND MOOS, R.H. The longterm course
December 1995.
will be collected in this area should
of treated alcoholism: I. Mortality, relapse, and remis
sion rates and comparisons with community controls. MOREY, L.C., AND JONES, J.K. Treatment implications
help elucidate the fundamental distinc Journal of Studies on Alcohol 52:44 –54, 1991. of a hybrid model for the classification of alcoholism.
tions among problem drinkers that are In: Watson, R.R., ed. Alcohol and Drug Abuse Reviews:
most relevant to treatment planning.
GARTNER, L., AND MEELEE, D. The Role and Current
Treatment of Drug and Alcohol Abuse. Clifton, NJ:
Despite their outward—and, to some
Status of Patient Placement Criteria in the Treatment
Humana Press, 1992. pp. 257–282.
of Substance Use Disorders: Treatment Improvement
extent, concurrent—validity, however, Protocol Series 13. Rockville, MD: Center for Substance MOREY, L.C.; SKINNER, H.A.; AND BLASHFIELD, R.K. A
placement criteria, such as the ASAM Abuse Treatment, 1995. typology of alcohol abusers: Correlates and implications.
guideline, still require outcome valida GASTFRIEND, D.R.; FILSTEAD, W.J.; REIF, S.; NAJAVITS,
Journal of Abnormal Psychology 93:408–417, 1984.
tion to ensure that they are indeed re L.M.; AND PARRELLA, D.P. Validity of assessing treat SAXE, L., AND GOODMAN, L. The Effectiveness of Out
lated to differential treatment outcomes. ment readiness in patients with substance use disorders. patient vs. Inpatient Treatment: Updating the OTA Re
Concurrently, the evolution of pa American Journal on Addictions 4:254–260, 1995. port. Hartford, CT: Prudential Insurance Company, 1988.
tient placement criteria could be en HAYASHIDA, M.; ALTERMAN, A.I.; MCLELLAN, A.T.; WALSH, D.C.; HINGSON, R.W.; MERRIGAN, D.M.;
hanced by carefully considering and O’BRIEN, C.P.; PURTILL, J.J.; VOLPICELLI, J.R.; LEVENSON, S.M.; CUPPLES, A.; HEEREN, T.; COFFMAN,
integrating existing guidelines with RAPHAELSON, A.H.; AND HALL, C.P. Comparative ef G.A.; BECKER, C.A.; BARKER, T.A.; HAMILTON, S.K.;
the results of typological research. As
fectiveness and costs of inpatient and outpatient detox MCGUIRE, T.G.; AND KELLY, C.A. A randomized trial
the alcoholism treatment field moves
ification of patients with mildtomoderate alcohol of treatment options for alcoholabusing workers. New
withdrawal syndrome. New England Journal of Med England Journal of Medicine 325:775–782, 1991.
toward unbundling treatment modali icine 320:358–365, 1989.
ties from treatment settings, it also WEEDMAN, R.D. Admission, Continued Stay and Dis
must understand the qualitative differ
HESTER, R.K., AND MILLER, W.H. Handbook of Alco charge Criteria for Adult Alcoholism and Drug De
holism Treatment Approaches: Effective Alternatives. pendence Treatment Services. Irvine, CA: National
ences between individuals who may New York: Pergamon Press, 1989. Association of Addiction Treatment Providers, 1987.
44 ALCOHOL HEALTH & RESEARCH WORLD
You might also like
- Case StudiesDocument17 pagesCase StudiesDamian Maguire100% (4)
- ASI Treatment Planning ManualDocument22 pagesASI Treatment Planning Manualdrmss100% (1)
- The Prevalence of Substance Use and Other Mental Health Concerns Among American AttorneysDocument7 pagesThe Prevalence of Substance Use and Other Mental Health Concerns Among American AttorneysDavid AndreattaNo ratings yet
- Case Study Paper Final ValentineDocument10 pagesCase Study Paper Final Valentineapi-3166145030% (1)
- Psychoactive Substances: Journey To The Center of The MindDocument43 pagesPsychoactive Substances: Journey To The Center of The Mindninkasi1No ratings yet
- Mental Health Case StudyDocument10 pagesMental Health Case Studyapi-403506258100% (1)
- Florida Substance Abuse Program Details Levels of CareDocument105 pagesFlorida Substance Abuse Program Details Levels of CareE M Sturdivant Gallieshaw100% (2)
- BiopsychosocialDocument6 pagesBiopsychosocialapi-307244919No ratings yet
- Psychiatric Mental Health Comprehensive Case StudyDocument8 pagesPsychiatric Mental Health Comprehensive Case Studyapi-544869292No ratings yet
- Group NotesDocument9 pagesGroup NotesD'Wayne HolidayNo ratings yet
- Annual Review of Addictions and Offender Counseling, Volume III: Best PracticesFrom EverandAnnual Review of Addictions and Offender Counseling, Volume III: Best PracticesNo ratings yet
- Sample EssayDocument9 pagesSample EssayBrian SrotaNo ratings yet
- Case Analysis: Bipolar 1 Diagnosis & Treatment PlanDocument2 pagesCase Analysis: Bipolar 1 Diagnosis & Treatment PlanJoshua Ringor100% (1)
- ASAM CriteriaDocument11 pagesASAM CriteriaÁngela Medina G100% (1)
- Mental Health Nursing Chapter 1: Defining Mental Health and IllnessDocument10 pagesMental Health Nursing Chapter 1: Defining Mental Health and IllnessChalcey PolsonNo ratings yet
- Clincial Paper - PsychDocument12 pagesClincial Paper - Psychapi-651130562100% (1)
- Treatment Improvement Protocol (TIP) Series 34: Brief Interventions and Brief Therapies For Substance AbuseDocument292 pagesTreatment Improvement Protocol (TIP) Series 34: Brief Interventions and Brief Therapies For Substance AbuseCorina IcaNo ratings yet
- Na ReflectionDocument6 pagesNa Reflectionapi-433710976No ratings yet
- CV Vivek Benegal 0610Document16 pagesCV Vivek Benegal 0610bhaskarsg0% (1)
- 2015 Final Case Studies Asam Fundamentals Final UpdatedDocument68 pages2015 Final Case Studies Asam Fundamentals Final UpdatedTrampa AdelinaNo ratings yet
- Alcohol Use Disorder MGMT Guideline - Final... EstDocument83 pagesAlcohol Use Disorder MGMT Guideline - Final... EstMuluken TesfayeNo ratings yet
- Narcotics Anonymous Meeting 3Document6 pagesNarcotics Anonymous Meeting 3api-401390929No ratings yet
- Chapter 7 Individual TreatmentDocument4 pagesChapter 7 Individual TreatmentCory HarnessNo ratings yet
- 12 Core FunctionsDocument14 pages12 Core Functionszaelany jrNo ratings yet
- CDI Patient VersionDocument9 pagesCDI Patient VersionalotfyaNo ratings yet
- DSM-5 Diagnosis Reference GuideDocument2 pagesDSM-5 Diagnosis Reference GuideDeAn White100% (1)
- Shortened REM Latency and Increased REM: Previous AttemptDocument19 pagesShortened REM Latency and Increased REM: Previous AttemptActeen MyoseenNo ratings yet
- Counselor's Manual For Relapse Prevention With Chemically Dependent Criminal Offenders Technical Assistance Publication Series 19Document133 pagesCounselor's Manual For Relapse Prevention With Chemically Dependent Criminal Offenders Technical Assistance Publication Series 19Norma FloresNo ratings yet
- Alcohol Withdrawal Syndrome: Benzodiazepines and Beyond: Abst TDocument7 pagesAlcohol Withdrawal Syndrome: Benzodiazepines and Beyond: Abst Taria tristayanthiNo ratings yet
- Mental Health Case StudyDocument11 pagesMental Health Case Studyapi-546878677No ratings yet
- Fig psychiatricAssessmentFormDocument4 pagesFig psychiatricAssessmentFormabbey jane mallillin100% (1)
- The Matrix Model in Outpatiens Substances AbuseDocument9 pagesThe Matrix Model in Outpatiens Substances AbuseEduardo Garza GarzaNo ratings yet
- Check List For PT ETOH Alcohol UseDocument12 pagesCheck List For PT ETOH Alcohol Usesen ANo ratings yet
- C2 Mod 6 Components of TXDocument105 pagesC2 Mod 6 Components of TXPUSAT LATIHAN AADKNo ratings yet
- Unit 9 - Mental HealthDocument35 pagesUnit 9 - Mental HealthKhushi GillNo ratings yet
- Interventions For Families of Substance AbuseDocument7 pagesInterventions For Families of Substance Abuseapi-284406278No ratings yet
- Community Meeting Paper Substance Abuse and SocietyDocument10 pagesCommunity Meeting Paper Substance Abuse and SocietyGabriela VasconcelosNo ratings yet
- Observations of An AA MeetingDocument2 pagesObservations of An AA MeetingKaryn Ives Kerr100% (1)
- Psychiatric Interview (Autosaved)Document22 pagesPsychiatric Interview (Autosaved)Jana Victor100% (1)
- Educational Training Manual: Certification Board, IncDocument58 pagesEducational Training Manual: Certification Board, IncAlexander MaukinNo ratings yet
- ASAM Application Guidance 8 2019Document22 pagesASAM Application Guidance 8 2019Victor Daniel Rivera Carrion100% (1)
- Borderline Personality DisorderDocument6 pagesBorderline Personality DisorderPersephona13No ratings yet
- Biopsychosocial InterviewDocument14 pagesBiopsychosocial Interviewapi-242734564100% (1)
- Suicide Risk and Assessment of Suicide-1Document33 pagesSuicide Risk and Assessment of Suicide-1Omeerul RafieNo ratings yet
- Substance Use Disorders A Guide For Primary CareDocument362 pagesSubstance Use Disorders A Guide For Primary CareDillart SpaceNo ratings yet
- Cns 780-Responding To Ethical Dilemmas Discussion 5 1Document2 pagesCns 780-Responding To Ethical Dilemmas Discussion 5 1api-326209227100% (1)
- CAGE Questionnaire For Alcohol MisuseDocument10 pagesCAGE Questionnaire For Alcohol MisuseJeremy BergerNo ratings yet
- bEST pRACTICEDocument23 pagesbEST pRACTICERusti Aisya DillianaNo ratings yet
- PsychopharmacologyDocument49 pagesPsychopharmacologysazaki224No ratings yet
- Background PaperDocument36 pagesBackground PaperSaad MotawéaNo ratings yet
- Alcohol and Substance Abuse Statistics and ModelsDocument30 pagesAlcohol and Substance Abuse Statistics and ModelsjackrosesNo ratings yet
- Group Therapy Time-Limited GroupsDocument5 pagesGroup Therapy Time-Limited GroupsNaida KarasalihovicNo ratings yet
- Alcohol in Health and DiseaseDocument648 pagesAlcohol in Health and DiseaseYuli KiaNo ratings yet
- Mckenzie St. Clair: Intervention Plan For Community Client With ReflectionDocument3 pagesMckenzie St. Clair: Intervention Plan For Community Client With Reflectionapi-518621879100% (1)
- Mental Status ExamDocument7 pagesMental Status ExamDanielle BanNo ratings yet
- TADCP 9th Annual Drug Court Conference AgendaDocument15 pagesTADCP 9th Annual Drug Court Conference AgendatadcpNo ratings yet
- Schizophrenia Spectrum and Other Psychotic DisordersDocument41 pagesSchizophrenia Spectrum and Other Psychotic DisordersNoelle Grace Ulep BaromanNo ratings yet
- Anti Anxiety DrugsDocument26 pagesAnti Anxiety DrugsHamze Abdullah Al-ShawaheenNo ratings yet
- Delirium TremensDocument15 pagesDelirium Tremensgiseladelarosa2006No ratings yet
- Medical Surgical and PsychiatricDocument10 pagesMedical Surgical and PsychiatricKusumadewi WidiarsaNo ratings yet
- 2015 Final Case Studies Asam Fundamentals Final UpdatedDocument68 pages2015 Final Case Studies Asam Fundamentals Final UpdatedTrampa AdelinaNo ratings yet
- Nursing Diagnosis Planning Interventions Rationale Evaluation Risk For Ineffective Breathing Pattern IndependentDocument5 pagesNursing Diagnosis Planning Interventions Rationale Evaluation Risk For Ineffective Breathing Pattern Independentjeff_scarlet26No ratings yet
- Nursing Diagnosis Impaired Gas ExchangeDocument7 pagesNursing Diagnosis Impaired Gas ExchangeZycon Rodney Ae'zecquel Gachallan50% (2)
- CIWA GuidelinesDocument5 pagesCIWA Guidelinesnavya sharmaNo ratings yet
- AssDocument54 pagesAssilmiah neuro unpadNo ratings yet
- What Effects Does Alcohol Have On HealthDocument22 pagesWhat Effects Does Alcohol Have On HealthChristopher ProsperoNo ratings yet
- Substance Abuse, Eating Disorders and Impulse ControlDocument14 pagesSubstance Abuse, Eating Disorders and Impulse ControlAaronAgulayNo ratings yet
- Baclofen in Alcohol DependenceDocument49 pagesBaclofen in Alcohol Dependenceanon_47568257No ratings yet
- Check List For PT ETOH Alcohol UseDocument12 pagesCheck List For PT ETOH Alcohol Usesen ANo ratings yet
- Alcohol Abuse Effects and Anorexia TreatmentDocument64 pagesAlcohol Abuse Effects and Anorexia TreatmentBrianMarBeltranNo ratings yet
- Nursing Bullets - Psychiatric NursingDocument13 pagesNursing Bullets - Psychiatric NursingDr. Jayesh PatidarNo ratings yet
- Substance Abuse VidebeckDocument48 pagesSubstance Abuse VidebeckFatima Hyghia Himpon100% (1)
- Management of Moderate and Severe Alcohol Withdrawal Syndromes - UpToDateDocument21 pagesManagement of Moderate and Severe Alcohol Withdrawal Syndromes - UpToDateSanti HerreraNo ratings yet
- Acute PsychosisDocument13 pagesAcute PsychosisIlyes FerenczNo ratings yet
- Psychological DisordersDocument403 pagesPsychological DisordersHHDSNo ratings yet
- Med Surg 2 BulletsDocument19 pagesMed Surg 2 BulletsShiraishiNo ratings yet
- Psychiatry SamsonDocument12 pagesPsychiatry Samsonamina100% (1)
- Case StudyDocument15 pagesCase StudyGaurav Kumar0% (1)
- Drug-Induced Psychosis GuideDocument32 pagesDrug-Induced Psychosis Guidemarkleacock100% (1)
- Community Ati Study GuideDocument16 pagesCommunity Ati Study Guidemaria sandoval100% (2)
- Program Rawatan, Pemulihan Dan Penagihan Alkohol Dan NikotinDocument42 pagesProgram Rawatan, Pemulihan Dan Penagihan Alkohol Dan NikotinPUSAT LATIHAN AADKNo ratings yet
- AustAlctreatguidelines 2009 PDFDocument255 pagesAustAlctreatguidelines 2009 PDFFrizam DwindamuldanNo ratings yet
- Psychiatric Exam SmpleDocument18 pagesPsychiatric Exam SmpleAngie MandeoyaNo ratings yet
- Alcohol Use DisorderDocument68 pagesAlcohol Use DisorderSarvess Muniandy100% (3)
- Epilepsia - UpToDateDocument28 pagesEpilepsia - UpToDateMiguelQuispeZeladaNo ratings yet
- Manage Alcohol Withdrawal Safely with CIWA-ArDocument28 pagesManage Alcohol Withdrawal Safely with CIWA-ArMohammed AlshamsiNo ratings yet