You might also like
- 4LEDocument1 page4LEShannen Christelle AndradeNo ratings yet
- Goal 3 - PH SDG - As of 18oct2019Document2 pagesGoal 3 - PH SDG - As of 18oct2019Shannen Christelle AndradeNo ratings yet
- (Med Ii) 4.04 Chronic Obstructive Pulmonary Disease (Copd) (Dr. Pingol) PDFDocument3 pages(Med Ii) 4.04 Chronic Obstructive Pulmonary Disease (Copd) (Dr. Pingol) PDFShannen Christelle AndradeNo ratings yet
- ACS Patho (HysioDocument3 pagesACS Patho (HysioShannen Christelle AndradeNo ratings yet
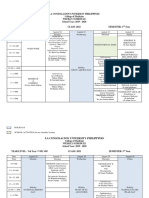
- Final3rd Year Schedule 1st Semester A.Y 2019-2020 As of August 21, 2019Document19 pagesFinal3rd Year Schedule 1st Semester A.Y 2019-2020 As of August 21, 2019Shannen Christelle AndradeNo ratings yet
- Examination of The EyesDocument5 pagesExamination of The EyesShannen Christelle AndradeNo ratings yet
- Diagnosing Leptospirosis with Lab TestsDocument41 pagesDiagnosing Leptospirosis with Lab TestsShannen Christelle AndradeNo ratings yet
- VaxDocument1 pageVaxShannen Christelle AndradeNo ratings yet
- Doctors' Emotional Experiences Impact Patient and Student CareDocument2 pagesDoctors' Emotional Experiences Impact Patient and Student CareShannen Christelle AndradeNo ratings yet
- Clinical Pathology ANDRADE, Shannen Christelle A. 17-4759-251 HomeworkDocument2 pagesClinical Pathology ANDRADE, Shannen Christelle A. 17-4759-251 HomeworkShannen Christelle AndradeNo ratings yet
- Trogens Propylthiouracil: HyperthyroidismDocument3 pagesTrogens Propylthiouracil: HyperthyroidismShannen Christelle AndradeNo ratings yet
- La Consolacion University Philippines College of Medicine Weekly ScheduleDocument3 pagesLa Consolacion University Philippines College of Medicine Weekly ScheduleShannen Christelle AndradeNo ratings yet
- Sensory ExamDocument2 pagesSensory ExamShannen Christelle AndradeNo ratings yet
- Methodology ResDocument4 pagesMethodology ResShannen Christelle AndradeNo ratings yet
- Sensory ExamDocument2 pagesSensory ExamShannen Christelle AndradeNo ratings yet
- Sensory ExamDocument2 pagesSensory ExamShannen Christelle AndradeNo ratings yet
- Tuberculosis - Causes, Symptoms, Diagnosis, Treatment & PathologyDocument11 pagesTuberculosis - Causes, Symptoms, Diagnosis, Treatment & PathologyShannen Christelle AndradeNo ratings yet
- 5.01 Introduction To Endocrine: ObjectivesDocument1 page5.01 Introduction To Endocrine: ObjectivesShannen Christelle AndradeNo ratings yet
- Med ChecklistDocument2 pagesMed ChecklistShannen Christelle AndradeNo ratings yet
- Patient RRDocument15 pagesPatient RRShannen Christelle AndradeNo ratings yet
- Radiopharmaceutical Safety Assessment in HospitalsDocument3 pagesRadiopharmaceutical Safety Assessment in HospitalsShannen Christelle AndradeNo ratings yet
- Swaitrmday 2 Floor 25 CMDocument2 pagesSwaitrmday 2 Floor 25 CMShannen Christelle AndradeNo ratings yet
- La Consolacion University Philippines College of Medicine Exam Week ScheduleDocument1 pageLa Consolacion University Philippines College of Medicine Exam Week ScheduleShannen Christelle AndradeNo ratings yet
- 5th Long ExamDocument1 page5th Long ExamShannen Christelle AndradeNo ratings yet
- Spreprmday 2 Floor 25 CMDocument1 pageSpreprmday 2 Floor 25 CMShannen Christelle AndradeNo ratings yet
- Experiment 1 What Is PhysicsDocument2 pagesExperiment 1 What Is PhysicsShannen Christelle AndradeNo ratings yet
- ABR WorksheetDocument19 pagesABR WorksheetShannen Christelle AndradeNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Master's Degree in Periodontology: COURSE 2023-2024Document14 pagesMaster's Degree in Periodontology: COURSE 2023-2024Liseth CarreñoNo ratings yet
- ER Utilization Budget AmendmentDocument2 pagesER Utilization Budget AmendmentLia PaulineNo ratings yet
- Suprarenal GlandDocument13 pagesSuprarenal GlandAaa JjjjNo ratings yet
- Baby Vaccination ProgramDocument1 pageBaby Vaccination Programplainspeak100% (1)
- Pain47, 295Document4 pagesPain47, 295Ezel RitmoNo ratings yet
- Dengue Disease Model With The Effect of Extrinsic Incubation PeriodDocument6 pagesDengue Disease Model With The Effect of Extrinsic Incubation PeriodDilruk GallageNo ratings yet
- Manual On Evacuation Camp Management DraftDocument47 pagesManual On Evacuation Camp Management DraftTelNo ratings yet
- Maxillary Impacted Canines: A Clinical Review: DR Rajiv Yadav, DR Basanta K. ShresthaDocument6 pagesMaxillary Impacted Canines: A Clinical Review: DR Rajiv Yadav, DR Basanta K. Shresthadrzana78No ratings yet
- Fibromyalgia: Annals of Internal MedicineDocument16 pagesFibromyalgia: Annals of Internal MedicineTeofanes PonceNo ratings yet
- AnatomyDocument93 pagesAnatomyHiba V.ANo ratings yet
- Novi Lestari 1911304150 B3Document3 pagesNovi Lestari 1911304150 B3FarahNo ratings yet
- VSL TB Workplace Policy ProgramDocument3 pagesVSL TB Workplace Policy ProgramAlexander John AlixNo ratings yet
- Viparita Karani - The Great Rejuvenator PoseDocument7 pagesViparita Karani - The Great Rejuvenator PoseDr Srinivasan Nenmeli -K100% (1)
- Topics: Nasopharyngeal CarcinomaDocument21 pagesTopics: Nasopharyngeal CarcinomaShruthi Y nursingNo ratings yet
- 10 1097@CCM 0b013e31818b35f2Document7 pages10 1097@CCM 0b013e31818b35f2omarihuanoNo ratings yet
- Colchicum Autumnale and The GoutDocument6 pagesColchicum Autumnale and The GoutLuluk HMNo ratings yet
- CBC ReportDocument1 pageCBC ReportPranay BhosaleNo ratings yet
- Potassium Sulphate vs Potassium Chloride: Their Influence on Crop Yield and QualityDocument109 pagesPotassium Sulphate vs Potassium Chloride: Their Influence on Crop Yield and QualityManuel SosaNo ratings yet
- Efficacy ClotrimazoleDocument4 pagesEfficacy ClotrimazoleAlexandra ConstantinescuNo ratings yet
- Frame Denture - Metal Frame BenefitsDocument8 pagesFrame Denture - Metal Frame BenefitsJennieNo ratings yet
- 1577un 2026-01Document79 pages1577un 2026-01ngovantienNo ratings yet
- Urinary EliminationDocument9 pagesUrinary EliminationTuTitNo ratings yet
- Human Anatomy 8th Edition Marieb Solutions Manual DownloadDocument14 pagesHuman Anatomy 8th Edition Marieb Solutions Manual DownloadMary Brown100% (23)
- Bronquiolite Guidelines AAPDocument32 pagesBronquiolite Guidelines AAPDiego Guedes da SilvaNo ratings yet
- MSDS Castrol Perfecto XPG 32Document4 pagesMSDS Castrol Perfecto XPG 32Teguh SNo ratings yet
- Hepatite B CoinfeçãoDocument31 pagesHepatite B Coinfeçãojefferson2392No ratings yet
- Treaty 6Document6 pagesTreaty 6api-541140582No ratings yet
- Farnsworth D15 Color Test KitDocument4 pagesFarnsworth D15 Color Test Kitdian eka saputraNo ratings yet
- J.P Final ThesisDocument54 pagesJ.P Final Thesislloydmarkagris143100% (1)
- Health, Safety & Nutrition for Young ChildrenDocument50 pagesHealth, Safety & Nutrition for Young ChildrenChen Lee WanNo ratings yet