You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5796)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
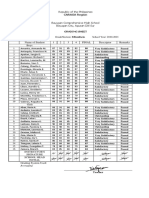
- Ma Angela Kristine Valencia - B. Grading Sheet Fili - 8Document1 pageMa Angela Kristine Valencia - B. Grading Sheet Fili - 8Ma. Angela Kristine ValenciaNo ratings yet
- 1015Document11 pages1015Crystal Audrey Malinda NelsonNo ratings yet
- CMDBuild WorkflowManual ENG V240 PDFDocument70 pagesCMDBuild WorkflowManual ENG V240 PDFPaco De Peco EdmspjpNo ratings yet
- AutacoidsDocument14 pagesAutacoidsMahmoud AboudNo ratings yet
- Parliamentary Election Impact W14299-PDF-ENGDocument8 pagesParliamentary Election Impact W14299-PDF-ENGHarshit ShubhankarNo ratings yet
- Worksheet16 Transcription To TranslationDocument3 pagesWorksheet16 Transcription To Translationliterally deadNo ratings yet
- Module 6Document4 pagesModule 6api-701165246No ratings yet
- Quality of Multiple Choice Questions in Fix Prosthodontic ModuleDocument10 pagesQuality of Multiple Choice Questions in Fix Prosthodontic ModuleInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Turbulence Modeling - BetaDocument88 pagesTurbulence Modeling - BetaMayra ZezattiNo ratings yet
- Running Head: Nurse Leadership and Effective Communication 1Document5 pagesRunning Head: Nurse Leadership and Effective Communication 1Maria O'ConnorNo ratings yet
- Life and Career Skills Survey FinalsDocument3 pagesLife and Career Skills Survey FinalsTopher FernandezNo ratings yet
- Sundaram Questions Assorted From GroupDocument23 pagesSundaram Questions Assorted From GroupAbu Syeed Md. Aurangzeb Al MasumNo ratings yet
- Creativity TechniquesDocument220 pagesCreativity Techniquesjcabbud100% (3)
- Dwnload Full Introduction To Environmental Geology 5th Edition Keller Test Bank PDFDocument35 pagesDwnload Full Introduction To Environmental Geology 5th Edition Keller Test Bank PDFgilmadelaurentis100% (12)
- Asterismos Famosos Observacion Phil HarringtonDocument3 pagesAsterismos Famosos Observacion Phil HarringtonMaria TeresaNo ratings yet
- Ferromagnetic HysteresisDocument4 pagesFerromagnetic HysteresisNedel LabileNo ratings yet
- R in Hydrology - EGUDocument25 pagesR in Hydrology - EGUJulio Montenegro GambiniNo ratings yet
- Sight GagDocument12 pagesSight Gagcecepo4733No ratings yet
- Bilal ThesisDocument63 pagesBilal ThesisKashif Ur RehmanNo ratings yet
- Properties of LogsDocument26 pagesProperties of Logsrcbern2No ratings yet
- Treatment of LeprosyDocument11 pagesTreatment of LeprosyFajar YuniftiadiNo ratings yet
- Material Safety Data Sheet: L IdentificationDocument4 pagesMaterial Safety Data Sheet: L Identificationkesling rsiNo ratings yet
- Task 10 Language TestDocument19 pagesTask 10 Language TestWITNESS NIKEZIWE MATHENJWANo ratings yet
- Carbonation of Steel SlagDocument12 pagesCarbonation of Steel SlagTania Dealina SariNo ratings yet
- Key Players in The Indian Industry TodayDocument46 pagesKey Players in The Indian Industry TodaydakshjainNo ratings yet
- Robert CapaDocument9 pagesRobert Capaapi-319825916No ratings yet
- Call Flow Comparison GSM UMTSDocument5 pagesCall Flow Comparison GSM UMTSSyed Zahid Shah100% (1)
- Insitu GelDocument96 pagesInsitu Gelvinsijuvin555No ratings yet
- LDR Project (Watermark)Document17 pagesLDR Project (Watermark)RakshitaNo ratings yet
- BSCRIM Program Specification AY 2018 2019Document9 pagesBSCRIM Program Specification AY 2018 2019Jezibel MendozaNo ratings yet