Professional Documents
Culture Documents
Elite Controllerof Hiv
Uploaded by
Peter JustinOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Elite Controllerof Hiv
Uploaded by
Peter JustinCopyright:
Available Formats
Review
Elite control of HIV infection:
implications for vaccine design
BM Baker, BL Block, AC Rothchild & BD Walker†
†Partners
AIDS Research Center, Massachusetts General Hospital and Division of AIDS,
1. Introduction Harvard Medical School, Boston, MA, USA
2. Viral genetics and HIV replication
Background: ‘Elite controllers’ are rare HIV-infected individuals who are able
3. Host genetic correlates of
HIV control
to spontaneously control HIV replication without medication, maintaining
viral loads that are consistently below the limits of detection by currently
4. Innate immunity and HIV control
available commercial assays. Objective: To examine studies of elite controllers
5. Acquired immunity and that may elucidate mechanisms of HIV immune control useful in designing
Expert Opin. Biol. Ther. Downloaded from informahealthcare.com by Selcuk Universitesi on 02/11/15
HIV control a vaccine. Methods: Recent literature on HIV controllers and studies that
6. Cellular immunity have evaluated aspects of viral and host immunology that correlate with
7. Conclusions viral control are examined. Results/conclusions: Although many elements of
8. Expert opinion innate and adaptive immunity are associated with control of HIV infection,
the specific mechanism(s) by which elite controllers achieve control remain
undefined. Ongoing studies of elite controllers, including those examining
host genetic polymorphisms, should facilitate the definition of an effective
HIV-specific immune response and guide vaccine design.
Keywords: acquired immune deficiency syndrome (AIDS), CD4+ T cell, CD8+ T cell,
For personal use only.
cell-mediated immunity, elite controller, human immunodeficiency virus (HIV),
human leucocyte antigen (HLA), simian immunodeficiency virus (SIV), vaccine, viral load
Expert Opin. Biol. Ther. (2009) 9(1):55-69
1. Introduction
Every day more than 6,800 people become infected with HIV and more than
5,700 people die of AIDS. There are currently an estimated 33.2 million people
living with HIV worldwide [1]. The number of individuals receiving antiretroviral
(ARV) therapy in both the developed and the developing world has increased
dramatically during the last few years due in part to financial commitments by
organizations such as the Global Fund to fight AIDS, TB, and Malaria (GFATM)
and the President’s Emergency Plan for AIDS Relief (PEPFAR) [2]. However,
the world failed to meet the goals set forth in the WHO’s ‘3 by 5’ plan [3]
and as of the end of 2007 it was estimated that only 31% of persons in low- and
middle-income countries who were in need of treatment were receiving it [2].
The low rates of treatment in resource-limited settings mean that most
HIV+ individuals in these areas have not benefited from highly-active anti-
retroviral therapy (HAART), treatment that has led to significant survival gains
in the US and other developed countries [2,4,5]. As a result, the vast majority
of global AIDS-related deaths during 2007 occurred among people in the
developing world without access to ARVs, with over three-quarters of these in
Sub-Saharan Africa [1].
A prophylactic HIV vaccine that conferred sterilizing immunity, fully preventing
or clearing the infection, could bring an end to the HIV epidemic, and by
preventing new infections it would limit future treatment needs. Although
the generation of a sterilizing vaccine remains the ultimate goal, two decades
of research suggest that it will be difficult to create a vaccine that prevents
infection [6]. Moreover, all effective vaccines currently in use have been shown
10.1517/14712590802571928 © 2009 Informa UK Ltd ISSN 1471-2598 55
All rights reserved: reproduction in whole or in part not permitted
Elite control of HIV infection: implications for vaccine design
A. B. C.
Th
CTL
Expert Opin. Biol. Ther. Downloaded from informahealthcare.com by Selcuk Universitesi on 02/11/15
Infected cell
B cell
Th
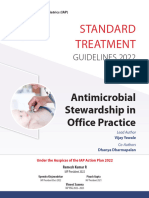
Figure 1. Immune control of HIV infection. A. Prior to cell entry, antibodies produced by B cells may neutralize free virus particles,
For personal use only.
preventing cells from becoming HIV infected. B. Once a cell is infected, cytotoxic T lymphocytes (CTL) may mount effective cytolytic
responses through recognition by a unique T cell receptor (TCR) of a viral peptide presented as a complex with human leukocyte antigen
(HLA) class I on the surface of the infected cell. C. If the immune response is not successful in controlling viral replication at stages A or B,
progeny virions will be produced and will bud from the infected cell, creating new virus particles that can go on to infect other cells,
though these may also be limited by neutralizing antibodies.
Th: T helper cell.
to prevent disease, not infection or colonization by themselves, the risk of transmission [6,9]. Such a T cell vaccine, would
and HIV infection has not yet been shown to be cleared attenuate HIV disease progression by enabling vaccinated
naturally in infected persons. It is unknown whether a vaccine and subsequently infected individuals to control viral replication
can accomplish something that nature has been unable to do. most probably through cytotoxic T lymphocyte (CTL)
Vaccines traditionally rely on the induction of a strong targeting of virus-infected cells [9], thereby limiting progeny
neutralizing antibody response to prevent infection, an approach virus production (Figure 1B).
whose success for controlling HIV is extremely challenging due This reduction of viral load would be anticipated to provide
to a number of unique properties of the virus. Foremost among considerable benefit to the health of the individual while also
these is the enormous sequence diversity of the HIV envelope reducing rates of forward-transmission and treatment demands,
proteins, the propensity for N-linked glycosylation occlude representing a significant public-health accomplishment [10-14].
the most immunogenic and highly-conserved regions of the Remarkably, there are individuals who naturally suppress
envelope protein, and steric constraints that make it difficult HIV replication, spontaneously maintaining viral loads below
for antibodies to attach to the envelope proteins [7,8]. Although the limits of detection without the assistance of ARV
broadly cross-reactive neutralizing antibodies have been therapy [15,16]. Unraveling the mechanism(s) by which these
isolated from some HIV+ individuals and thus serve as a elite controllers limit viral replication could inform design of
proof-of-principle that such antibodies can be generated, people a vaccine that limits HIV disease progression. In this article,
with broadly cross-reactive antibodies are extremely rare [7]. we review the current research on the influence of viral
Due to the many obstacles that HIV presents to the design genetics, host genetics, and host immune responses on HIV
of a neutralizing antibody-mediated sterilizing vaccine which disease progression and viral replication. We also delineate
would have the potential to interact with free virions and the pressing questions that remain in the field, discuss impli-
provide sterilizing immunity (Figure 1A), much of the field cations of a recently terminated T-cell-based HIV vaccine trial,
has turned its attention towards the design of a HIV vaccine and describe a new collaborative study that should help
stimulating cellular immune responses that would provide deepen our understanding of the mechanisms that enable
durable protection from HIV disease progression and reduce elite controllers to suppress viral replication.
56 Expert Opin. Biol. Ther. (2009) 9(1)
Baker, Block, Rothchild & Walker
2. Viral genetics and HIV replication Large cohort studies have shown that certain HLA Class I
alleles correlate with HIV control (Figure 2), providing
Before sensitive HIV RNA assays became clinically available strong evidence that the immune system plays a role in
in the mid 1990’s it was not possible to quantify HIV levels determining the rate of disease progression and implicating
produced in vivo. Hence, early descriptions of individuals CTL immunity in this control. The HLA Class I allele
who did not progress to AIDS were largely based on the with the strongest and most consistently recognized asso-
duration of infection and CD4 counts, not levels of viremia. ciation with viral control is B*5701 [26-29]. HLA-B27 has
Long-term non-progressors (LTNP), HIV-infected individuals also been repeatedly linked with HIV nonprogression [29,30].
with stable CD4 counts and no history of AIDS-defining Interestingly, many individuals with this allele display an
illnesses, were estimated to constitute 5 – 15% of the HIV immunodominant CTL response to a single HIV-Gag
positive population [17,18]. p24 epitope (KK10) that is subject to viral escape. A
With the advent of sensitive assays that quantify the number predictable series of point mutations both within and
of copies of viral RNA in plasma, it became clear that the near this epitope leads to inadequate HLA binding, loss
Expert Opin. Biol. Ther. Downloaded from informahealthcare.com by Selcuk Universitesi on 02/11/15
majority of LTNP have ongoing viral replication at detectable of CTL recognition, and an increase in viral load [31]. In
levels. In fact, some LTNP have been identified who have addition to HLA-B57 and HLA-B27, there are several other
high levels of circulating virus [19]. However, these assays HLA-B alleles that have been associated with viral control
also identified a subset of LTNP, elite controllers, who and others that have been associated with a lack of
consistently maintain undetectable viral loads, defined as control [27,29,32]. The mechanisms underlying these differences
< 50 copies/ml, the limit of detection of standard commercial are not known.
assays used clinically to monitor patients [16]. Studies of In addition to the identification of specific protective or
LTNP have shown that some of these individuals are infected deleterious alleles, several studies have shown that homozygosity
with defective virus [20,21]. A logical question, then, is at one or more HLA loci is associated with faster progression
whether elite controller status is attributable to inefficient to AIDS [29,32]. This heterozygote advantage model suggests
viral replication or due to host immune control or other that heterozygosity at each HLA Class I allele allows for
For personal use only.
host-specific genetic factors. presentation of a greater range of epitopes, producing a
The isolation of replication-competent virus from elite greater breadth of T cell responses and enabling more effective
controllers suggests that control is not entirely due to deficient control of HIV replication [29,32].
virus [22,23]. Findings of discordant couples from a recent HLA-B alleles can be categorized as either Bw4 or Bw6 based
study as well as from our own cohort of elite controllers also on amino acid sequences at positions 77-83, which form a part
implicate host immune responses in the control of HIV of the Class I binding pocket for viral peptides. Interestingly,
replication [24]. Several sets of discordant couples have been most of the alleles associated with HIV disease resistance are
found in which one individual is an HIV controller while members of the HLA-Bw4 motif family, while those associated
the other person experiences standard, progressive infection. with HIV disease susceptibility are part of the Bw6 family.
Viral sequencing analysis has confirmed transmission and Given that HLA-Bw4 alleles can bind the natural killer
all viruses are replication competent. The fact that one (NK) cell receptor killer cell immuno-globulin-like receptor,
of these individuals is viremic while the other is aviremic three domains, long cytoplasmic tail, 1 (KIR3DL1) while
suggests that elite controller status is due to host immune HLA-Bw6 alleles cannot [29], it is possible that poly-
responses or host genetics (T Miura and BD Walker, morphisms within NK cell receptors affect HIV disease
unpublished). Learning precisely what host genetics and progression. Studies to this end have demonstrated an epistatic
immune responses correlate with this protection is thus protective effect for KIR and HLA genes, showing that the
a topic of great importance as it can guide design of a combined genotype of three domains, short cytoplasmic tail,
cell-mediated vaccine. 1 (KIR3Ds1), an activating KIR receptor with high sequence
homology to KIR3DL1, and HLA-Bw4-80I, a HLA-Bw4 motif
3. Host genetic correlates of HIV control with isoleucine at position 80, is enriched in a population of
slow progressors, linked to low viral load set points, and
3.1 The human leukocyte antigens protective against AIDS-defining opportunistic infections [33,34].
During viral infection, Class I human leukocyte antigens Certain KIR3DL1 alleles matched with HLA-Bw4 alleles also
(HLA) present endogenously processed viral antigens on associate with lower mean viral loads and slower progression
the surface of infected cells to CD8+ T cells, which to AIDS [35]. The additive protective effect of certain HLA
then attempt to clear the virus-infected cells by direct and KIR alleles implies coordination between the innate and
lysis of the infected cell and/or production of antiviral adaptive HIV immune responses, suggesting that enhancement
cytokines. HLA loci are the most polymorphic sites in of innate immunity alongside stimulation of adaptive immunity
the human genome [25], and therefore represent a good could be important for HIV vaccine design. However, the
starting point for examining the effect of host genetics on precise mechanisms by which these responses mediate an
HIV disease progression. effect are unknown.
Expert Opin. Biol. Ther. (2009) 9(1) 57
Elite control of HIV infection: implications for vaccine design
p < 0.001 Patients: n = 956 p = 0.001 Patients: n = 650
B5701 ( • ) B2705 ( • )
B2705 ( • ) B1302 ( • )
bw4 ( • ) B5101 ( • )
B1401 ( • ) B5201 ( • )
B1302 ( • ) bw4 ( • )
B5201 ( • ) B5701 ( • )
B5101 ( • ) B4403 ( • )
B5801 ( • ) B1401 ( • )
B4403 ( • ) B4402 ( • )
B4402 ( • ) B0801 ( • )
B4002 ( • ) B4002 ( • )
B0801 ( • ) B5801 ( • )
B3801 ( • ) B3801 ( • )
B5301 ( • ) B5301 ( • )
B4901 ( • ) B0702 ( • )
B0702 ( • ) B4901 ( • )
B1501 ( • ) B1501 ( • )
Expert Opin. Biol. Ther. Downloaded from informahealthcare.com by Selcuk Universitesi on 02/11/15
B3701 ( • ) B3701 ( • )
B1402 ( • ) B1402 ( • )
B3901 ( • ) B1801 ( • )
B41 ( • ) B3501 ( • )
B1801 ( • ) B3502 ( • )
B3501 ( • ) bw6 ( • )
B5601 ( • ) B5601 ( • )
B3502 ( • ) B4001 ( • )
bw6 ( • ) B3901 ( • )
B4001 ( • ) B41 ( • )
B5001 ( • ) B3503 ( • )
B5501 ( • ) B5501 ( • )
B3503 ( • ) B5001 ( • )
-3.5 -3.0 -2.5 -2.0 -1.5 -1.0 0.1 0.2 0.3 0.4 0.5 0.6 0.7
Δ Square root CD4 count per year Δ Log viral load per year
For personal use only.
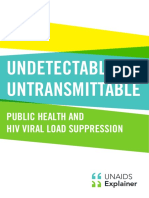
Figure 2. Effect of human leukocyte antigen (HLA)-B alleles on CD4 decline and viral load increase over time after HIV
infection. Average change in the square root CD4 counts (left side) and log viral load measurements (right side) per year and 95%
confidence intervals were determined using a linear mixed effects regression (LMER). HLA-B alleles that are most to least protective are
listed from top to bottom, respectively. The vertical line in the middle of each plot represents the sample average and confidence intervals
for alleles deviating significantly from this value do not cross the line. Alleles shown in green are HLA-B Bw4+, while those in black are
HLA-B Bw6+. Data from both seroconverter and seroprevalent individuals were used in the analysis. Seroconversion date was used as the
intercept in the LMER, but in seroprevalents, the first observed data point was used instead. p values were determined using the Wald test.
3.2 HIV co-receptors and their ligands of these co-receptor polymorphisms on the ability of
3.2.1 CCR5 and CCR2b HIV to infect CD4 cells support blocking chemokine
In order to attach to, fuse with, and enter a cell, HIV must receptors as an effective therapeutic strategy. Indeed, CCR5
bind to both the CD4 receptor and a chemokine co-receptor. antagonists are already being used as a new class of
M-tropic (R5) viruses utilize CCR5 as their co-receptor, while anti-HIV drugs.
T-tropic (X4) viruses, which predominate later in the course
of infection, use CXCR4. A 32-base pair deletion within the 3.2.2 Chemokine receptor ligands
CCR5 gene (CCR5-Δ32) limits CCR5 cell-surface expression The association of certain polymorphisms in HIV-1 co-receptor
of this receptor. In persons heterozygous for this allele, this genes with disease progression has prompted investigation of
mutation correlates with lower viral load set points, and persons whether differences in expression levels of the natural ligands
who are homozygous for this mutated allele experience of the co-receptors, such as regulated upon activation,
complete protection from HIV infection, at least from normally T-expressed, and presumably secreted (RANTES),
viruses requiring CCR5 for entry [36-38]. A polymorphism at mitogen-activated protein kinase interacting protein 1α
position -2459 within the CCR5 promoter region which (MIP-1α), MIP-1β, and stromal cell derived factor 1
leads to lower CCR5 expression on macrophages also associates (SDF-1), also affect disease progression. It is currently
with slower disease progression, lower viral propagation, and suspected that these ligands, such as CCL3L1, can inhibit
higher β-chemokine expression [39,40]. HIV entry into cells by competing for co-receptor binding,
A mutation that similarly affects the ability of HIV and thus retard disease progression [37,41-44]. The extent
to infect CD4+ cells has been identified in another to which these polymorphisms or combinations of these
chemokine co-receptor, CCR2b, which is found primarily polymorphisms may contribute to durable HIV control is
in persons of African descent [37]. Collectively, the effects unclear at this time.
58 Expert Opin. Biol. Ther. (2009) 9(1)
Baker, Block, Rothchild & Walker
3.2.3 Other host factors that influence HIV disease higher cytotoxic capacity, despite showing similar cell surface
progression: APOBEC3G, TRIM5a, and IL-10 expression of inhibitory and activating receptors [55]. Studies
Apolipoprotein B mRNA editing enzyme, catalytic polypeptide- have also shown greater NK killing and production of IFN-γ,
like 3G APOBEC3G (CEM15, hA3G) is a human cytidine TNF-α, and β-chemokines in exposed uninfected individuals
deaminase that limits infectivity of HIV-1 in strains lacking compared with unexposed individuals or seroconverters [55,56].
the viral protein Vif (virion infectivity factor) [45]. A study However, it is still not clear how much of the difference in lytic
that included eight LTNP demonstrated an association ability is due to persistent HIV viremia and immune activation
between APOBEC3G mRNA levels and lower viral loads as that causes NK dysfunction in viremic individuals [57-59].
well as higher CD4 counts, although other studies have not Since very early events following acute HIV infection appear
been able to replicate this association [46,47]. While evidence to have a major effect on subsequent disease progression,
has shown increased levels of APOBEC3G expression in specific features of the innate immune responses may well
exposed-uninfected individuals, expression levels have not play a role in establishing an elite controller state.
been found to be increased in elite controllers [48] leaving
Expert Opin. Biol. Ther. Downloaded from informahealthcare.com by Selcuk Universitesi on 02/11/15
the role of APOBEC3G in attenuating progression and/or 4.2 Toll-like receptors
preventing infection still subject to debate [49]. Toll-like receptors (TLRs) are pattern recognition molecules that
Tripartite motif-containing 5α (TRIM5α) is an innate recognize foreign particles and trigger the production of type 1
immunity factor that can block HIV-1 capsid uncoating in Old interferons and other cytokines [60]. TLR7/8 and TLR9,
World Monkeys but not in humans [50]. Using chimeric which recognize single stranded RNA (ssRNA) and CpG DNA
proteins produced from human and rhesus monkey TRIM5α motifs respectively, have repeatedly been found to play a role in
sequences, the unique amino acid residue within the protein’s modulating HIV-1 disease progression. TLR7/8 activates mono-
specificity protein 1a and ryanodine receptor (SPRY) domain cytes and plasmacytoid dendritic cells (pDCs) through the
that confers HIV-1 resistance in rhesus monkeys has been myeloid differentiation primary response gene 88 (MyD88)
identified [51]. Mimicking this blocking mechanism found in signaling pathway upon recognition of specific HIV-1 RNA
Old World Monkeys could prove to be an effective therapy sequences [61]. These activated pDCs go on to produce
For personal use only.
in humans. However, whether host polymorphisms in these IFN-α that contributes to an apoptotic pathway, leading to
genes might contribute to differences in disease outcome a decline in CD4+ T cells in lymphoid tissue [62]. HIV
remains unclear. nonprogressors were shown to produce lower levels of
IL-10 is a cytokine that induces immunosuppression IFN-α and the apoptotic pathway ligands compared with
through inactivation of T cells and inhibition of a T helper progressors, which suggests a role for the TLR7/8–MyD88
type 1 (Th1) response [25]. Murine studies of lymphocytic activating pathway in disease progression [62]. Certain poly-
choriomeningitis virus (LCMV) have shown that removal of morphisms found within the receptor gene for TLR9 also
IL-10 or inhibition of the IL-10 receptor leads to increases associate with rapid HIV disease progression, providing
in T cell activity and viral clearance [52]. However, IL-10 has further evidence that innate immunity and TLRs may influence
also been shown to reduce HIV-1 replication in macrophages, HIV disease outcome [63].
but not in dendritic cells, through a blockade in an entry
or post-entry stage [53]. A dominant polymorphism in the 5. Acquired immunity and HIV control
promoter region, termed IL10 5′A, which leads to a pronounced
reduction in IL-10 levels, correlates with faster progression 5.1 Neutralizing antibodies
to AIDS [28,36]. These studies highlight the delicate balance Neutralizing antibodies are crucial for preventing infection
of immunosuppression in HIV infection. While cellular of susceptible cells and can facilitate cell killing through
activation may lead to increased susceptibility to infection antibody-dependent cell-cytotoxicity (ADCC) [9,25]. However,
and disease progression [54] it is likely that an effective T cell it is not clear whether neutralizing antibodies help limit
response is needed to durably control HIV infection. HIV disease progression.
Recent evidence from the rhesus macaque model has shown
4. Innate immunity and HIV control that the presence of a late broadly reactive neutralizing antibody
response spanning two years does not associate with lower
4.1 Natural killer cells viral loads or slowed disease progression, and that these high
NK cells control infection by detecting changes in HLA antibody titers could merely be a result of continual exposure
Class I expression through inhibitory and activating receptors, to high levels of viremia [64]. Although this study seems
leading to both lytic activity and cytokine production [25]. The to downplay the importance of neutralizing antibodies in
viral control associated with this interaction has been control of SIV disease progression, there is also evidence that
described above through the epistatic relationship between NK post-infection passive immunization with anti-SIV neutralizing
KIR inhibitory receptor subtypes and HLA alleles [33-35]. antibodies in rhesus macaques can lead to viral load suppression
Studies comparing NK cells derived from LTNP and through dendritic cell antigen uptake and T cell stimulation [65].
progressors have found that LTNP possess NK cells with a A similar study has shown that passive immunization with
Expert Opin. Biol. Ther. (2009) 9(1) 59
Elite control of HIV infection: implications for vaccine design
anti-SIV IgG can lead to a decrease in the number of 6.2Associations between CD8+ T-cell phenotype and
SIV-infected cells, most probably through ADCC [66]. disease outcome
Analyses of our own cohort of elite controllers have Recently, several groups have demonstrated an inverse
shown that very few of them have broadly cross-reacting correlation between the quality of CTL responses and
neutralizing antibodies, suggesting that antibodies are not the rate of disease progression [82-84]. T cell quality, in
the main mechanism mediating control of replication, this case, is defined by either the presence of multi- or
despite other studies that have found patient sera capable polyfunctional responses, or the absence of negative
of broadly neutralizing a panel of different viruses [67-69]. immunoregulatory molecules, such as Programmed Death-1
This observation supports a previous study that demon- (PD-1 or CD279).
strated that plasma from elite controllers lacked the ability CTL are termed polyfunctional if they are able to produce
to neutralize autologous virus [70]. In contrast, a study multiple cytokines [83]. The most frequently assessed cytokines
examining neutralizing antibody responses to autologous are IFN-γ, MIP-1β, interleukin-2, TNF-α, and the degranu-
viruses in acute and chronically infected patients found lation marker CD107α. Production of multiple cytokines is
Expert Opin. Biol. Ther. Downloaded from informahealthcare.com by Selcuk Universitesi on 02/11/15
low levels of neutralizing antibody responses during thought to be indicative of a high quality response and has
chronic infection, but not during acute stages, and greater been correlated with viral control and a vigorous proliferative
responses among controllers than among other chronically capacity in murine models [85]. In contrast, cells that are
infected patients [71]. only capable of producing IFN-γ display a diminished ability
to proliferate in response to antigenic stimulation [82].
6. Cellular immunity Not surprisingly, HIV controllers seem to possess a higher
proportion of durable, multi-functional CD8+ T cells that
6.1 Cytotoxic T-lymphocytes persist in the systemic circulation throughout the course of
Numerous lines of evidence suggest that cytotoxic T-lymphocyte infection compared with progressors [83] – suggesting that
(CTL) responses are critically important for controlling polyfunctional CTL may contribute to control of HIV
HIV replication, but their exact role in elite control infection (Figure 4).
For personal use only.
remains unclear. It has long been known that CTL can Interestingly, these polyfunctional T cells from controllers
recognize and kill HIV-infected cells [72], and that the are not only capable of rapid proliferation, but they also
appearance of the CTL response coincides temporally seem to be particularly potent killers. Recent studies have
with the reduction of viremia and resolution of symptoms shown that the ability to proliferate is coupled to increased
of acute infection [73,74]. Furthermore, studies in rhesus perforin expression. These higher levels probably facilitate
macaques, including one that specifically looked at an cell killing and thus contribute to the efficacy of the CTL
‘elite controller’ animal model with rhesus macaques response [86]. Together, these findings indicate that control of
that controlled a pathogenic SIV infection for 1 – 5 years, HIV replication is marked by the presence of polyfunctional,
have shown that depletion of CD8+ T cells leads to a loss potent cellular immune responses that persist throughout
of viral control that is restored upon reappearance of the course of infection. Unfortunately, however, it is impossible
SIV-specific CTL [75,76]. The correlation between certain to be certain whether this is cause or effect. It may be that
HLA Class I alleles and HIV disease progression [29], prolonged low-level viremia allows for accumulation of these
coupled with HIV’s propensity for mutating to evade CTL cells, and therefore it is not certain that they contribute
responses, provides more evidence for the importance of to control.
CTL in controlling HIV disease progression [77,78]. Further data have revealed that certain combinations of
Due to CD8+ T cells’ apparent ability to affect disease CTL surface markers associate predictably with varying levels
progression, it was initially suspected that elite controllers of viral control and immunologic differentiation. Significant
would display a high breadth and magnitude of CTL responses attention has been given to HLA-DR and CD38 molecules.
to HIV. However, studies have failed to demonstrate a HLA-DR is a marker of effector CD8+ T cells and CD38 is
correlation between the quantity of CTL responses, as an activation marker. In HIV controllers, HLA-DR+/CD38-
determined by IFN-γ Enzyme-linked immunosorbent spot expressing cells predominate, whereas in non-controllers,
(ELISPOT) assay, and viral load [79,80]. In fact, the number CTL are more frequently HLA-DR+/CD38+ as a result of
of responses appears to be driven by viremia, with those chronic stimulation [87]. HLA-DR+/CD38- CTL exist in
individuals exposed to more virus mounting greater CTL a state of low immune activation with the capacity for
responses [68]. However, even among elite controllers there is extensive proliferation [87].
substantial heterogeneity in CD8 T cell responses, with Other studies have shown that HIV controllers have
some controllers having very few HIV-specific CTL a higher proportion of circulating effector CTL that are
responses, as described in a recently published study and terminally-differentiated (CD45RA+ and CCR7-) than HIV
observed within our own cohort (Figure 3) [81]. Attention progressors [88]. A block in the full differentiation of memory
has thus shifted to the quality and specificity of CTL effector cells may contribute to a lack of valuable CTL
responses, rather than the breadth of the response alone. responses produced by HIV progressors.
60 Expert Opin. Biol. Ther. (2009) 9(1)
Baker, Block, Rothchild & Walker
Elite controller with low responses to overlapping HIV peptides
1750
1500
1250
SFC/106 PBMC
1000 Breadth: 2
750
Magnitude: 440
500
250
0
F
T
EF
L
EV
R
V
AG
VI
TA
PO
EN
VP
VP
N
R
G
Expert Opin. Biol. Ther. Downloaded from informahealthcare.com by Selcuk Universitesi on 02/11/15
Elite controller with high responses to overlapping HIV peptides
1750
1500
Breadth: 41
1250
SFC/106 PBMC
Magnitude: 8433
1000
750
500
250
0
For personal use only.
F
T
EF
L
EV
R
AG
VI
PO
TA
VP
VP
EN
N
R
G
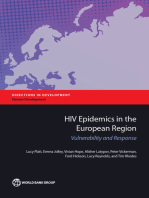
Figure 3. Heterogeneity of CTL responses in elite controllers measure by IFN-g ELISPOT. IFN-γ responses [spot-forming cells
(SFC)/106 peripheral blood mononuclear cells (PBMC)] from two elite controllers measured by enzyme-linked immunosorbent spot
(ELISPOT) assay. Each subject was tested against. 410 peptides overlapping by 10 amino acids and spanning the whole HIV proteome,
they exhibit significant differences in both the breadth and the magnitude of their responses.
6.3 Associations between CTL specificity and IFN-γ responses that were conserved in B*57 positive LTNP
disease outcome but not progressors [92]. However, a recent report has
When it comes to CTL targeting of HIV-infected cells, it suggested that in spite of significant selection pressure
appears that not all responses are created equal. In cohort applied to the virus by B*57-restricted CTL responses, elite
studies of individuals in South Africa with chronic clade controllers have the capacity to maintain responses to
C HIV infection, increased breadth of targeting of HIV-Gag wild-type sequence and to generate de novo responses to
protein, taken as a percentage of total HIV-directed CTL viral variants [93].
responses, correlates with lower viral load. In contrast, The discordant inhibitory capacity of cells targeting
individuals with higher viral loads focus more of their CTL epitopes in different HIV proteins is probably due to a
against HIV-Env [89]. Studies of our Clade-B-infected combination of viral and host factors. The nine HIV proteins
controller population have found a similar trend – individuals vary in their ability to accommodate escape mutations
with lower viral loads tend to more extensively target without inducing a fitness cost. In the case of Gag and Env,
HIV-Gag [90]. Similarly, a study in pigtail macaques showed it is likely that Gag is subject to more stringent sequence
that monkeys that generated SIV-Gag-specific CTL responses constraints than Env, making it more difficult for HIV to
following prime/boost vaccination had lower viral loads and mutate away from Gag-specific CTL responses [94]. More
increased retention of CD4+ T cells after challenge with generally, eliciting immune responses against the most
SHIVmn229 than monkeys who made similar CTL responses highly-conserved regions of HIV appears to be a good
against SIV-Env or monkeys who made no CTL responses strategy [95], given HIV’s high mutation rate and evidence
at all [91]. that escape mutations can result in a loss of suppressive ability
Even within a single HIV protein, there are differences in in HIV controllers [31]. In the case of elite controllers, a recent
response patterns to different epitopes. A recent study found publication has highlighted the ability of elite controllers to
that just one out of four B*57-restricted epitopes in Nef had maintain CTL responses in spite of the rise of viral mutants,
Expert Opin. Biol. Ther. (2009) 9(1) 61
Elite control of HIV infection: implications for vaccine design
CD4+ cells CD8+ cells
0.03 0.28 < 0.004 0.04 Elite
controller
0.12 0.43
IL-2
Expert Opin. Biol. Ther. Downloaded from informahealthcare.com by Selcuk Universitesi on 02/11/15
< 0.004 <0.004 0.01 < 0.004 Chronic
progressor
0.05 0.97
For personal use only.
IFN-γ
Figure 4. Comparison of flow cytometric-measured HIV-specific T cell responses between an elite controller and an untreated
chronic progressor. Flow analysis of Gag-specific CD4+ and CD8+ T cell responses measured by intracellular cytokine staining. Dead
cells are excluded from analysis by gating only on dead-cell-dye-negative cells, CD3+ CD14/19- cells are identified as T cells. CD4+ and
CD8+ subpopulations are identified based on the presence of surface markers. The percentage of cells within the CD4+ and CD8+
subpopulations that produce Il-2, IFN-γ or both cytokines is measured for a representative elite controller and a chronic progressor.
which may be one of the key characteristics separating of polyfunctional CD4+ T cell responses that include IL-2
controllers from non-controllers and allowing for prolonged production, although it is unclear whether or not viremia
resistance to progressive infection [96]. levels are driving CD4+ T cell dysfunction [84,97-100]. As was
Host factors may also contribute to the discordant efficacy observed for CD8+ T Cells, IL-2 production by CD4+
of CTL responses against different HIV proteins. It is possible T cells is positively correlated with the ability to proliferate
that CD8+ T cells specific for certain HIV proteins bind with following exposure to antigen [101]. A recent study suggests
a higher avidity, proliferate more extensively and thus inhibit that inactivation of the forkhead box, sub-group O 3a
more efficiently. Recent data from our cohort indicates that (FOXO3a) pathway, which regulates Fas-mediated apoptosis,
even clonal populations that are specific for the same epitope may contribute to the preservation of CD4+ T cells observed
can have varying anti-viral effects due to the specific T cell in elite controllers [102].
receptor (TCR) that is engaged (H Chen and B Walker, Interestingly, while classical immunology characterizes
unpublished). Further studies into antigen processing, presentation, CD4+ T cells as helper cells, CD4+ cells in controllers
and CD8 recognition of the HLA-peptide complex are can also carry out cytolytic activity and thus directly
needed to elucidate the mechanisms responsible for the contribute to viral suppression. This killing is probably
observed differences in order to gain a better understanding perforin-dependent, as is evidenced by a statistically significant
of how to optimize the cytolytic functions of CD8+ T cells. difference in levels of perforin expression between controllers
and uninfected controls [103].
6.4 CD4+ T cell responses
Preservation of CD4+ T cell responses throughout HIV 6.5 Immune activation
infection also appears to be crucial for immune control of HIV HIV viral load is widely regarded as a good indicator for
replication. Studies have demonstrated statistically significant risk of disease progression [10,13,14]. However, it is becoming
correlations between disease progression and the proportion apparent that the level of immune activation in an individual
62 Expert Opin. Biol. Ther. (2009) 9(1)
Baker, Block, Rothchild & Walker
is one of the strongest predictors of disease progression [104], However, the theory that PD-1 expression levels on CTL
even among elite controllers [105]. determine their ability to mount an effective immune
Low viral loads generally correlate with low levels of response may have the causal relationship reversed. A newly
immune activation, making it difficult to determine whether published report offers evidence that the high levels of circu-
HIV disease progression is driven by HIV viremia, immune lating antigen in persons failing to effectively control HIV
activation, or both. A recent study describes several HIV-infected viremia may in fact cause T cell exhaustion, rather than
persons experiencing non-progressive infection despite being a result of T cell exhaustion [112]. This finding would
having very high levels of viremia [19]. These individuals seem to corroborate the report of another recent publication
have similar immune patterns to Sooty Mangabees, the which found that CD8+ cells specific for the HLA B*27
reservoir species for HIV-2 and the source of many lab KK10 epitope, which one would expect to be highly effective
strains of SIV, in that they live with high levels of virus but CTL because this epitope is highly-immunodominant and
do not mount a vigorous anti-viral cellular immune response seems to be a critical CTL target, express just as much PD-1
to it and do not experience disease [106]. The lack of disease as those CTL that do not target this epitope [113].
Expert Opin. Biol. Ther. Downloaded from informahealthcare.com by Selcuk Universitesi on 02/11/15
progression despite chronically high viremia in these individuals To sum up, there does seem to be a strong correlation
suggests that immune activation, rather than HIV itself, between PD-1 expression and disease progression, but the
may cause disease progression. directionality of this relationship is unclear. Further studies,
Further evidence that immune activation could be in particular those looking at elite controllers, are thus
deleterious is available in both the macaque model and in needed to clarify the relationship between PD-1 expression
human studies. A recent report in the SIV literature described and control of HIV infection.
extensive depletion of CD4+ T cells with a regulatory phenotype Like PD-1, CD152 (CTLA-4) is often upregulated during
during acute infection [107], suggesting that the removal of a HIV infection [114]. CTLA-4 is an immunoregulatory
barrier to T cell activation may be partly responsible for the molecule that is primarily expressed on CD4+ T lymphocytes.
rapid infection and depletion of CD4+ T cells during acute It has been implicated in the loss of CTL responses observed
infection. In humans, studies examining the level of the in some individuals during chronic HIV infection [115].
For personal use only.
inhibitory cytokine IL-10 have found that decreased levels of Currently, the leading hypothesis is that CTLA-4high T cells
IL-10 correlate with increased immune activation and faster decrease IL-2 secretion, thus preventing the initiation of an
HIV disease progression [28,36]. Finally, studies of elite controllers immune response [114].
have shown that among individuals with undetectable viremia, Recent studies looking at both HIV and Cytomegalovirus
those with higher levels of T cell activation, marked by the (CMV) infection have found that CTLA-4 expression correlates
HLA-DR+CD38+ phenotype, have lower CD4 counts [105]. inversely with CD4 count in both acutely and chronically
infected individuals [114,115]. Interestingly, HIV controllers
6.6 Negative regulators of immune activation do not demonstrate an upregulation of CTLA-4 on CD4+
6.6.1 PD-1 and CTL antigen 4 (CTLA-4) T cells and do not develop an exhausted phenotype [114].
Inhibitory immunoregulatory markers are elevated on both Learning why the PD-1 and CTLA-4 pathways are not
CD4+ and CD8+ T cells in individuals experiencing progressive upregulated on T lymphocytes in elite controllers will help
HIV-infection [108-110]. Binding of PD-1 (CD279) with the development of strategies for circumventing upregulation
either of its ligands, PD-L1 or PD-L2, on CD8+ T cells of these immunoregulatory pathways in recipients of a
delivers an immunosuppressive signal presumably aimed at cell-mediated HIV vaccine.
preventing autoimmunity. PD-1 binding leads to decreased
cytokine production by CD8+ cells, and in turn, a reduction 6.6.2 Regulatory T cells
in the proliferative capacity of these cells [110]. PD-1 expression Regulatory T cells, or Tregs, are T cells that inhibit the
is increased on the surface of HIV-specific T lymphocytes, effector functions of other T cells. Tregs are characterized by
suggesting that these cells are somehow being selectively the presence of the transcription factor forkhead box P3
blocked from carrying out their cytolytic activity [109]. In (FOXP3), which is critical for Treg development, and surface
fact, PD-1 expression levels on both CD4+ and CD8+ expression of the inhibitory ligand CTLA-4, which binds to
lymphocytes correlate positively with viral load and negatively the CD80 and CD86 receptors on T lymphocytes [116]. The
with CD4 count [108,110]. vast majority of Tregs are CD4+, although some CD8+
HIV controllers express significantly lower levels of PD-1 T cells also express FOXP3 [117].
than people with progressive disease [111]. It has been suggested Tregs constitute approximately 5% of overall CD4+ T cells
that the lower levels of PD-1 in controllers enable them to and are probably involved in the prevention of autoimmunity,
maintain competent, polyfunctional HIV-specific CTL. as their depletion in healthy hosts leads to autoimmune
Conversely, T cells in individuals with high levels of PD-1 complications [117]. Tregs have been the subject of extensive
are thought to be ‘exhausted’ because they are unable to research in many cancers as they are thought to prevent
efficiently carry out their cytolytic activity, and this exhaustion anti-tumor immune activity. For example, studies of ovarian
could permit HIV to replicate virtually unchecked. cancer have shown that higher concentrations of circulating
Expert Opin. Biol. Ther. (2009) 9(1) 63
Elite control of HIV infection: implications for vaccine design
Tregs correlate with poorer prognosis, and that higher 8. Expert opinion
CTL:Treg ratios predict increased survival [118,119].
In the case of HIV, it remains unclear whether Tregs are HIV vaccine design efforts were recently paused by the
protective or deleterious, and it may be that Tregs exert termination of Merck’s Phase II trial of its recombinant
different effects in different anatomical locations and/or stages adenovirus vaccine. This vaccine consisted of HIV Gag, Pol
of infection [120]. For instance, Tregs capable of suppressing and Nef genes delivered by an adenovirus vector. Early
lymphoproliferative responses against HIV have been identified results of the trial showed that the vaccine failed to demon-
in the blood of HIV-infected persons, and cohort studies strate any protection from acquisition, an endpoint that is
have shown that the percentage of Tregs correlates with viral not expected for a T-cell-based vaccine, or a lowered viral set
load [121] and is elevated in patients with CD4 < 200/µl [122]. point, a marker of viral control and a more realistic endpoint
These findings seem to indicate that Treg levels during the of a T-cell-based vaccine. In fact, the vaccine may have actually
chronic phase correlate with disease progression. However, increased susceptibility to HIV in persons seropositive for
research in the SIV model has shown that Tregs are severely adenovirus prior to immunization [124]. This unexpected
Expert Opin. Biol. Ther. Downloaded from informahealthcare.com by Selcuk Universitesi on 02/11/15
depleted in the intestinal lamina propria during acute SIV finding raises questions as to whether induction of strong
infection [107]. This depletion of Tregs is coincident with the cellular immune responses alone, at least with this particular
initial burst of HIV viremia, which suggests that depletion of vaccine vector and protocol, guarantees vaccine efficacy or
Tregs increases cell-susceptibility to HIV infection and that even safety. Because of these safety concerns and the fact that
Tregs may actually be protective during acute infection. no HIV vaccine candidates so far have produced beneficial
results in Phase II/III efficacy trials, we are in agreement with
7. Conclusions others [125] who suggest that more basic research into what
defines an effective HIV-specific immune response is necessary
More than a quarter of a century after the start of the AIDS before proceeding with human clinical trials. Studying elite
epidemic, HIV continues to kill millions worldwide while controllers, individuals who by definition are effectively
affecting countless more. Vast improvements in treatment suppressing HIV replication, can help us answer this question.
For personal use only.
have transformed HIV into a chronic, manageable disease for Though much is now known about elite controllers, no
some [4], however many people in need of treatment are still single genetic characteristic has been identified that is shared
not receiving it [3]. With tens of millions of people infected by a majority of elite controllers; however, it is clear that
and several million new infections occurring each year, an HIV there are several genetic components that account for at
vaccine remains the best hope for ending the epidemic. least part of their viral control. Similarly, while there is
The ideal HIV vaccine would be 100% effective at strong evidence for cellular immunity contributing to control
preventing new infections. Unfortunately, it is unlikely that and we are beginning to develop an understanding of which
a first generation HIV vaccine will be able to confer sterilizing HIV proteins make the best CTL targets, we have yet to
immunity [6]. Vaccines that achieve protective immunity rely identify any cellular responses that are either necessary or
on the induction of a strong neutralizing antibody response, sufficient for control. Therefore, we should continue to pursue
which is proving extremely difficult to achieve in HIV vaccine avenues of basic research, identifying differences between the
design. Neutralizing antibodies against HIV are rarely immune responses observed in HIV controllers and progressors,
detected in HIV+ individuals [7], and vaccines that have and also seeking to define new genes that are implicated in
elicited neutralizing antibodies in vitro have failed to confer protection from disease progression. As we learn more about
any degree of protection [123]. elite controllers, our understanding of precisely what genetic
Given the difficulty of eliciting an effective neutralizing factors and immune responses naturally correlate with HIV
antibody response, the focus of vaccine design has turned to control will guide vaccine design.
a cell-mediated approach. Although it would permit infection, New technologies that allow for rapid and affordable
a T cell vaccine would ideally attenuate disease progression and sequencing of the human genome may be useful in evaluating
reduce the risk of transmission. In order to create a successful genetic associations with HIV disease outcome [126]. Indeed,
HIV vaccine, we must first dissect the correlates of immune this technique has already enabled researchers to scan across the
protection. Specifically, we must learn: i) how we can generate entire human genome for polymorphisms that correlate with
highly functional CTL? ii) what are the most potent CTL outcomes in other disease settings. As part of the International
targets? and iii) how we can make effective immune responses HIV Controllers Study [127] we are performing a genome
durable? Elite controllers probably hold the key to answering wide association scan looking at 650,000 single-nucleotide
some of these questions and learning what factors are needed polymorphisms (SNPs) in HIV controllers and progressors,
to create a T-cell-based vaccine that enables individuals to mount in order to find previously unidentified genetic associations
an immune response that is both effective and durable. While with HIV disease outcome. 1,500 subjects have already been
the answers to these questions are unlikely to surmount the scanned by this genome-wide association scan (GWAS) method,
current obstacles to designing a sterilizing vaccine, they will and preliminary analyses are underway. A similar study has
hopefully guide us towards an effective T cell vaccine. already yielded genetic associations with lower level viremia
64 Expert Opin. Biol. Ther. (2009) 9(1)
Baker, Block, Rothchild & Walker
following acute infection [128]. Two of the polymorphisms Acknowledgements
discovered, however, were not found in a majority of a cohort
of elite controllers that was subsequently studied [129]. This The authors acknowledge M Carrington, PhD, Laboratory of
disparity underscores the need for more and larger studies like Genomic Diversity, NCI-Frederick, and F Pereyra, MD, Partners
the International HIV Controllers Study, which take a AIDS Research Center, for providing Figures 2 and 4, respectively.
systematic, focused and unbiased approach to trying to The authors also acknowledge the following members of the HIV
learn how elite controllers mediate their suppression of Elite Controller Study for their input and guidance: M Addo,
HIV replication. Indeed, it is our hope that by focusing MD PhD, B Julg, MD and A Piechocka-Trocha, DVM.
specifically on comparing elite controllers, who are by
definition exceptional, with patients who have high viral Declaration of interest
loads, the International HIV Controllers Study will be
powered to uncover novel mechanisms of immune control This work was supported by grants from the NIH (AI28568),
of HIV infection and could thus have major implications for the International AIDS Vaccine Initiative, and the Harvard
Expert Opin. Biol. Ther. Downloaded from informahealthcare.com by Selcuk Universitesi on 02/11/15
generation of HIV vaccines. University Center for AIDS Research.
Bibliography RNA level on rate of CD4 T-cell decline virus type 1 infection. N Engl J Med
1. UNAIDS, AIDS epidemic update: in untreated HIV infection. JAMA 1995;332(4):201-8
a special report on HIV/AIDS. 2007. 2006;296(12):1498-506 19. Choudhary SK, Vrisekoop N, Jansen CA,
UNAIDS. Geneva 11. Walensky RP, Paltiel AD, Goldie SJ, et al. et al. Low immune activation despite
2. WHO, Towards universal access: A therapeutic HIV vaccine: how good is good high levels of pathogenic human
Scaling up priority HIV/AIDS enough? Vaccine 2004;22(29-30):4044-53 immunodeficiency virus type 1 results
interventions in the health sector: 12. Gupta SB, Jacobson LP, Margolick JB, in long-term asymptomatic disease.
Progress Report 2008 WHO Press: Geneva et al. Estimating the benefit of an HIV-1 J Virol 2007;81(16):8838-42
vaccine that reduces viral load set point. 20. Alexander L, Weiskopf E, Greenough TC,
For personal use only.
3. WHO. Coverage and need for antiretroviral
treatment. 2007; Available from: J Infect Dis 2007;195(4):546-50 et al. Unusual polymorphisms in human
http://www.who.int/hiv/facts/cov0605/en/. 13. Mellors JW, Muñoz A, Giorgi JV, et al. immunodeficiency virus type 1 associated
[Last accessed 27 November 2008] Plasma viral load and CD4+ lymphocytes with nonprogressive infection. J Virol
as prognostic markers of HIV-1 infection. 2000;74(9):4361-76
4. Walensky RP, Paltiel AD, Losina E,
et al. The survival benefits of AIDS Ann Intern Med 1997;126(12):946-54 21. Learmont JC, Geczy AF, Mills J, et al.
treatment in the United States. J Infect Dis 14. Lyles RH, Muñoz A, Yamashita TE, et al. Immunologic and virologic status after
2006;194(1):11-9 Natural history of human immunodeficiency 14 to 18 years of infection with an
virus type 1 viremia after seroconversion attenuated strain of HIV-1. A report
5. Palella FJ Jr, Delaney KM, Moorman AC,
and proximal to AIDS in a large cohort of from the Sydney Blood Bank Cohort.
et al. Declining morbidity and mortality
homosexual men. Multicenter AIDS N Engl J Med 1999;340(22):1715-22
among patients with advanced human
immunodeficiency virus infection. Cohort Study. J Infect Dis 22. Blankson JN, Bailey JR, Thayil S, et al.
HIV Outpatient Study Investigators. 2000;181(3):872-80 Isolation and characterization of
N Engl J Med 1998;338(13):853-60 15. Lambotte O, Boufassa F, Madec Y, et al. replication-competent human
HIV controllers: a homogeneous group of immunodeficiency virus type 1 from a
6. Johnston MI, Fauci AS. An HIV
HIV-1-infected patients with spontaneous subset of elite suppressors. J Virol
vaccine–evolving concepts. N Engl J Med
control of viral replication. Clin Infect Dis 2007;81(5):2508-18
2007;356(20):2073-81
2005;41(7):1053-6 23. Miura T, Brockman MA, Brumme CJ,
7. Burton DR, Desrosiers RC, Doms RW,
16. Deeks SG, Walker BD. Human et al. Genetic characterization of human
et al. HIV vaccine design and the
immunodeficiency virus controllers: immunodeficiency virus type 1 in elite
neutralizing antibody problem.
mechanisms of durable virus control in controllers: Lack of gross genetic defects or
Nat Immunol 2004;5(3):233-6
the absence of antiretroviral therapy. common amino acid changes. J Virol
8. Wyatt R, Sodroski J. The HIV-1 2008;82(15):7395-410
Immunity 2007;27(3):406-16
envelope glycoproteins: fusogens,
17. Munoz A, Kirby AJ, He YD, et al. 24. Bailey JR, O’Connell K, Yang HC, et al.
antigens, and immunogens. Science
Long-term survivors with HIV-1 Transmission of human immunodeficiency
1998;280(5371):1884-8
infection: incubation period and virus type 1 from a patient who developed
9. Pantaleo G, Koup RA. Correlates of AIDS to an elite suppressor. J Virol
longitudinal patterns of CD4+ lymphocytes.
immune protection in HIV-1 infection: 2008;82(15):7395-410
J Acquir Immune Defic Syndr Hum Retrovirol
what we know, what we don’t know,
1995;8(5):496-505 25. Janeway C, Walport M, Shlomchik M.
what we should know. Nat Med
18. Cao Y, Qin L, Zhang L, et al. Virologic and Immunobiology: the immune system in
2004;10(8):806-10
immunologic characterization of long-term health and disease. sixth edition. 2005,
10. Rodriguez B, Sethi AK, Cheruvu VK, New York: Garland Science Publishing
survivors of human immunodeficiency
et al. Predictive value of plasma HIV
Expert Opin. Biol. Ther. (2009) 9(1) 65
Elite control of HIV infection: implications for vaccine design
26. Migueles SA, Sabbaghian MS, Shupert the CCR-5 chemokine receptor gene. 49. Biasin M, Piacentini L, Lo Caputo S,
WL, et al. HLA B*5701 is highly associated Nature 1996;382(6593):722-5 et al. Apolipoprotein B mRNA-editing
with restriction of virus replication in a 39. Salkowitz JR, Bruse SE, Meyerson H, et al. enzyme, catalytic polypeptide-like 3G:
subgroup of HIV-infected long term CCR5 promoter polymorphism determines a possible role in the resistance to HIV
nonprogressors. Proc Natl Acad Sci USA macrophage CCR5 density and magnitude of HIV-exposed seronegative individuals.
2000;97(6):2709-14 of HIV-1 propagation in vitro. Clin Immunol J Infect Dis 2007;195(7):960-4
27. Kiepiela P, Leslie AJ, Honeyborne I, et al. 2003;108(3):234-40 50. Stremlau M, Owens CM, Perron MJ, et al.
Dominant influence of HLA-B in mediating 40. Hladik F, Liu H, Speelmon E, et al. The cytoplasmic body component TRIM5α
the potential co-evolution of HIV and Combined effect of CCR5-Δ32 restricts HIV-1 infection in Old World
HLA. Nature 2004;432(7018):769-75 heterozygosity and the CCR5 promoter monkeys. Nature 2004;427(6977):848-53
28. O’Brien SJ, Nelson GW, Human genes that polymorphism -2459 A/G on CCR5 51. Yap MW, Nisole S, Stoye JP. A single
limit AIDS. Nat Genet 2004;36(6):565-74 expression and resistance to human amino acid change in the SPRY domain of
29. Carrington M, O’Brien SJ, The immunodeficiency virus type 1 transmission. human Trim5α leads to HIV-1 restriction.
influence of HLA genotype on AIDS. J Virol 2005;79(18):11677-84 Curr Biol 2005;15(1):73-8
Expert Opin. Biol. Ther. Downloaded from informahealthcare.com by Selcuk Universitesi on 02/11/15
Annu Rev Med 2003;54:535-51 41. Liu H, Chao D, Nakayama EE, et al. 52. Brooks DG, Trifilo MJ, Edelmann KH,
30. Magierowska M, Theodorou I, Debré P, Polymorphism in RANTES chemokine et al. Interleukin-10 determines viral
et al. Combined genotypes of CCR5, promoter affects HIV-1 disease progression. clearance or persistence in vivo.
CCR2, SDF1, and HLA genes can predict Proc Natl Acad Sci USA Nat Med 2006;12(11):1301-9
the long-term nonprogressor status in 1999;96(8):4581-5 53. Ancuta P, Bakri Y, Chomont N, et al.
human immunodeficiency virus-1-infected 42. Vidal F, Peraire J, Domingo P, et al. Opposite effects of IL-10 on the ability of
individuals. Blood 1999;93(3):936-41 Polymorphism of RANTES chemokine dendritic cells and macrophages to replicate
31. Kelleher AD, Long C, Holmes EC, et al. gene promoter is not associated with primary CXCR4-dependent HIV-1 strains.
Clustered mutations in HIV-1 gag are long-term nonprogressive HIV-1 infection J Immunol 2001;166(6):4244-53
consistently required for escape from of more than 16 years. J Acquir Immune 54. Castelli JC, Deeks SG, Shiboski S, et al.
HLA-B27-restricted cytotoxic T lymphocyte Defic Syndr 2006;41(1):17-22 Relationship of CD8+ T cell noncytotoxic
For personal use only.
responses. J Exp Med 2001;193(3):375-86 43. Modi WS, Lautenberger J, An P, et al. Genetic anti-HIV response to CD4+ T cell number
32. Carrington M, Nelson GW, Martin MP, variation in the CCL18.-CCL3.-CCL4. in untreated asymptomatic HIV-infected
et al. HLA and HIV-1: heterozygote chemokine gene cluster influences HIV individuals. Blood 2002;99(11):4225-7
advantage and B*35-Cw*04 disadvantage. Type 1 transmission and AIDS disease 55. O’Connor GM, Holmes A, Mulcahy F,
Science 1999;283(5408):1748-52 progression. Am J Hum Genet et al. Natural killer cells from long-term
2006;79(1):120-8 non-progressor HIV patients are
33. Martin MP, Gao X, Lee JH, et al. Epistatic
interaction between KIR3DS1 and HLA-B 44. McDermott DH, Beecroft MJ, characterized by altered phenotype
delays the progression to AIDS. Nat Genet Kleeberger CA, et al. Chemokine RANTES and function. Clin Immunol
2002;31(4):429-34 promoter polymorphism affects risk of 2007);124(3):277-83
both HIV infection and disease progression 56. Scott-Algara D, Truong LX, Versmisse P,
34. Qi Y, Martin MP, Gao X, et al. KIR/HLA
in the Multicenter AIDS Cohort Study. et al. Cutting edge: increased NK cell
pleiotropism: protection against both HIV
AIDS 2000;14(17):2671-8 activity in HIV-1-exposed but uninfected
and opportunistic infections. PLoS Pathog
2006;28:e79. Published online 18 August, 45. Sheehy AM, Gaddis NC, Choi JD, et al. Vietnamese intravascular drug users.
2006, doi:10.1371/journal.ppat.0020079 Isolation of a human gene that inhibits HIV-1 J Immunol 2003;171(11):5663-7
infection and is suppressed by the viral Vif 57. Fauci AS, Mavilio D, Kottilil S. NK cells in
35. Martin MP, Qi Y, Gao X, et al. Innate
protein. Nature 2002;418(6898):646-50 HIV infection: paradigm for protection or
partnership of HLA-B and KIR3DL1
subtypes against HIV-1. Nat Genet 46. Jin X, Brooks A, Chen H, et al. targets for ambush. Nat Rev Immunol
2007;39(6):733-40 APOBEC3G/CEM15 (hA3G) mRNA 2005;5(11):835-43
levels associate inversely with human 58. Kottilil S, Shin K, Planta M, et al.
36. Carrington M, Nelson G, O’Brien SJ.
immunodeficiency virus viremia. Expression of chemokine and inhibitory
Considering genetic profiles in functional
J Virol 2005;79(17):11513-6 receptors on natural killer cells: effect
studies of immune responsiveness to
HIV-1. Immunol Lett 2001;79(1-2):131-40 47. Cho SJ, Drechsler H, Burke RC, et al. of immune activation and HIV viremia.
APOBEC3F and APOBEC3G mRNA J Infect Dis 2004;189(7):1193-8
37. Ioannidis JP, Rosenberg PS, Goedert JJ,
levels do not correlate with human 59. Mavilio D, Lombardo G, Benjamin J, et al.
et al. Effects of CCR5.-32., CCR2.-64I.,
immunodeficiency virus type 1 plasma Characterization of CD56-/CD16+ natural
and SDF.-1.3.′A. alleles on HIV-1 disease
viremia or CD4+ T-cell count. J Virol killer (NK) cells: a highly dysfunctional NK
progression: An international meta-analysis
2006;80(4):2069-72 subset expanded in HIV-infected viremic
of individual-patient data. Ann Intern Med
2001;135(9):782-95 48. Gandhi SK, Siliciano JD, Bailey JR, et al. individuals. Proc Natl Acad Sci USA
Role of APOBEC3G/F-mediated 2005;102(8):2886-91
38. Samson M, Libert F, Doranz BJ, et al.
hypermutation in the control of human 60. Kawai T, Akira S. Innate immune
Resistance to HIV-1 infection in caucasian
immunodeficiency virus type 1 in elite recognition of viral infection.
individuals bearing mutant alleles of
suppressors. J Virol 2008;82(6):3125-30 Nat Immunol 2006;7(2):131-7
66 Expert Opin. Biol. Ther. (2009) 9(1)
Baker, Block, Rothchild & Walker
61. Meier A, Alter G, Frahm N, et al. autologous and heterologous viruses in but no correlation to viral load. J Virol
MyD88-dependent immune activation acute versus chronic human 2003;77(3):2081-92
mediated by human immunodeficiency immunodeficiency virus (HIV) infection: 81. Emu B, Sinclair E, Hatano H, et al. HLA
virus type 1-encoded toll-like receptor evidence for a constraint on the ability of class I-restricted T-cell responses may
ligands. J Virol 2007;81(15):8180-91 HIV to completely evade neutralizing contribute to the control of human
62. Herbeuval JP, Nilsson J, Boasso A, et al. antibody responses. J Virol immunodeficiency virus infection, but
Differential expression of IFN-α and 2006;80(12):6155-64 such responses are not always necessary
TRAIL/DR5 in lymphoid tissue 72. Walker BD, Chakrabarti S, Moss B, for long-term virus control. J Virol
of progressor versus nonprogressor et al. HIV-specific cytotoxic 2008;82(11):5398-407
HIV-1-infected patients. Proc Natl Acad T lymphocytes in seropositive individuals. 82. Peretz Y, Ndongala ML, Boulet S, et al.
Sci USA 2006;103(18):7000-5 Nature 1987;328(6128):345-8 Functional T cell subsets contribute
63. Bochud PY, Hersberger M, Taffé P, et al. 73. Koup RA, Safrit JT, Cao Y, et al. Temporal differentially to HIV peptide-specific
Polymorphisms in Toll-like receptor 9 association of cellular immune responses responses within infected individuals:
influence the clinical course of HIV-1 with the initial control of viremia in correlation of these functional T cell
Expert Opin. Biol. Ther. Downloaded from informahealthcare.com by Selcuk Universitesi on 02/11/15
infection. Aids 2007;21(4):441-6 primary human immunodeficiency virus subsets with markers of disease progression.
64. Kraft Z, Derby NR, McCaffrey RA, et al. type 1 syndrome. J Virol 1994;68(7):4650-5 Clin Immunol 2007;124(1):57-68
Macaques infected with a CCR5-tropic 74. Borrow P, Lewicki H, Hahn BH, et al. 83. Betts MR, Nason MC, West SM, et al.
simian/human immunodeficiency virus Virus-specific CD8+ cytotoxic HIV nonprogressors preferentially maintain
(SHIV) develop broadly reactive anti-HIV T-lymphocyte activity associated with highly functional HIV-specific CD8+
neutralizing antibodies. J Virol control of viremia in primary human T cells. Blood 2006;107(12):4781-9
2007;81(12):6402-11 immunodeficiency virus type 1 infection. 84. Emu B, Sinclair E, Favre D, et al.
65. Yamamoto H, Kawada M, Takeda A, et al. J Virol 1994;68(9):6103-10 Phenotypic, functional, and kinetic
Post-infection immunodeficiency virus 75. Schmitz JE, Kuroda MJ, Santra S, et al. parameters associated with apparent
control by neutralizing antibodies. Control of viremia in simian T-cell control of human immunodeficiency
PLoS One 2007;2:e540. Published online immunodeficiency virus infection by virus replication in individuals with and
For personal use only.
20 June 2007, doi:10.1371/journal. CD8+ lymphocytes. Science without antiretroviral treatment. J Virol
pone.0000540 1999;283(5403):857-60 2005;79(22):14169-78
66. Binley JM, Clas B, Gettie A, et al. Passive 76. Friedrich TC, Valentine LE, Yant LJ, et al. 85. Wherry EJ, Blattman JN, Murali-Krishna K,
infusion of immune serum into simian Subdominant CD8+ T-cell responses are et al. Viral persistence alters CD8 T-cell
immunodeficiency virus-infected rhesus involved in durable control of AIDS virus immunodominance and tissue distribution
macaques undergoing a rapid disease course replication. J Virol 2007;81(7):3465-76 and results in distinct stages of functional
has minimal effect on plasma viremia. 77. Allen TM, Altfeld M, Geer SC, et al. impairment. J Virol 2003;77(8):4911-27
Virology 2000;270(1):237-49 Selective escape from CD8+ T-cell responses 86. Migueles SA, Laborico AC, Shupert WL,
67. Harrer T, Harrer E, Kalams SA, et al. represents a major driving force of human et al. HIV-specific CD8+ T cell
Strong cytotoxic T cell and weak immunodeficiency virus type 1 (HIV-1) proliferation is coupled to perforin
neutralizing antibody responses in a subset sequence diversity and reveals constraints expression and is maintained in
of persons with stable nonprogressing on HIV-1 evolution. J Virol nonprogressors. Nat Immunol
HIV type 1 infection. AIDS Res 2005;79(21):13239-49 2002;3(11):1061-8
Hum Retroviruses 1996;12(7):585-92 78. Schneidewind A, Brockman MA, Yang R, 87. Saez-Cirion A, Lacabaratz C, Lambotte O,
68. Pereyra F, Addo MM, Kaufmann DE, et al. et al. Escape from the dominant et al. HIV controllers exhibit potent CD8
Genetic and immunologic heterogeneity HLA-B27-restricted cytotoxic T cell capacity to suppress HIV infection
among persons who control HIV infection T-lymphocyte response in Gag is associated ex vivo and peculiar cytotoxic T lymphocyte
in the absence of therapy. J Infect Dis with a dramatic reduction in human activation phenotype. Proc Natl Acad
2008;197(4):563-71 immunodeficiency virus type 1 replication. Sci USA 2007;104(16):6776-81
69. Li Y, Migueles SA, Welcher B, et al. Broad J Virol 2007;81(22):12382-93 88. Addo MM, Draenert R, Rathod A, et al.
HIV-1 neutralization mediated by 79. Betts MR, Ambrozak DR, Douek DC, Fully differentiated HIV-1 specific CD8+
CD4-binding site antibodies. Nat Med et al. Analysis of total human T effector cells are more frequently
2007;13(9):1032-4 immunodeficiency virus (HIV)-specific detectable in controlled than in progressive
70. Bailey JR, Lassen KG, Yang HC, et al. CD4+ and CD8+ T-cell responses: HIV-1 infection. PLoS One 2007;23:e321.
Neutralizing antibodies do not mediate relationship to viral load in untreated HIV Published online 28 march 2007,
suppression of human immunodeficiency infection. J Virol 2001;75(24):11983-91 doi:10.1371/journal.pone.0000321
virus type 1 in elite suppressors or selection 80. Addo MM, Yu XG, Rathod A, et al. 89. Kiepiela P, Ngumbela K, Thobakgale C,
of plasma virus variants in patients on Comprehensive epitope analysis of et al. CD8+ T-cell responses to different
highly active antiretroviral therapy. human immunodeficiency virus type 1 HIV proteins have discordant associations
J Virol 2006;80(10):4758-70 (HIV-1)-specific T-cell responses directed with viral load. Nat Med 2007;13(1):46-53
71. Deeks SG, Schweighardt B, Wrin T, et al. against the entire expressed HIV-1 genome 90. Florencia Pereyra BB, Rothchild A, Baker B,
Neutralizing antibody responses against demonstrate broadly directed responses, et al. Preferential targeting of HIV-Gag
Expert Opin. Biol. Ther. (2009) 9(1) 67
Elite control of HIV infection: implications for vaccine design
epitopes in elite controllers. In: HIV immunodeficiency virus-specific CD4+ HIV-specific memory CD8+ T-cell
vaccines: from basic research to clinical T cells are a consequence of antigen load. exhaustion in typical progressors but
trials. Whistler, British Columbia. J Virol 2007;81(6):2713-25 not in long-term nonprogressors.
March 25–30; 2007 101. Boaz MJ, Waters A, Murad S, et al. CD4 Blood 2007;109(11):4671-8
91. Peut V, Kent SJ. Utility of human responses to conserved HIV-1 T helper 112. Streeck H, Brumme ZL, Anastario M, et al.
immunodeficiency virus type 1 epitopes show both negative and positive Antigen load and viral sequence
envelope as a T-cell immunogen. associations with virus load in chronically diversification determine the functional
J Virol 2007;81(23):13125-34 infected subjects. Clin Exp Immunol profile of HIV-1-specific CD8+ T cells.
92. Navis M, Schellens IM, van Swieten P, 2003;134(3):454-63 PLoS Med 2008;55:e100. Published online
et al. A nonprogressive clinical course in 102. van Grevenynghe J, Procopio FA, He Z, 6 May 2008, doi:10.1371/journal.
HIV-infected individuals expressing human et al. Transcription factor FOXO3a controls pmed.0050100
leukocyte antigen B57/5801 is associated the persistence of memory CD4+ T cells 113. Almeida JR, Price DA, Papagno L, et al.
with preserved CD8+ T lymphocyte during HIV infection. Nat Med Superior control of HIV-1 replication by
responsiveness to the HW9 epitope in Nef. 2008;14(3):266-74 CD8+ T cells is reflected by their avidity,
Expert Opin. Biol. Ther. Downloaded from informahealthcare.com by Selcuk Universitesi on 02/11/15
J Infect Dis 2008;197(6):871-9 103. Norris PJ, Moffett HF, Yang OO, et al. polyfunctionality, and clonal turnover.
93. Bailey JR, Williams TM, Siliciano RF, et al. Beyond help: direct effector functions J Exp Med 2007;204(10):2473-85
Maintenance of viral suppression in of human immunodeficiency virus 114. Kaufmann DE, Kavanagh DG, Pereyra F,
HIV-1-infected HLA-B*57+ elite type 1-specific CD4+ T cells. J Virol et al. Upregulation of CTLA-4 by
suppressors despite CTL escape mutations. 2004;78(16):8844-51 HIV-specific CD4+ T cells correlates with
J Exp Med 2006;203(5):1357-69 104. Deeks SG, Kitchen CM, Liu L, et al. disease progression and defines a reversible
94. LANL, HIV Sequence Database. 2008. Immune activation set point during early immune dysfunction. Nat Immunol
Available from: http://www.hiv.lanl.gov/ HIV infection predicts subsequent CD4+ 2007;8(11):1246-54
content/sequence/HIV/mainpage.html T-cell changes independent of viral load. 115. Zaunders JJ, Ip S, Munier ML, et al.
[Last accessed 27 October 2008] Blood 2004;104(4):942-7 Infection of CD127+ (interleukin-7
95. Altfeld M, Allen TM. Hitting HIV 105. Hunt PW, Brenchley J, Sinclair E, et al. receptor+) CD4+ cells and overexpression
For personal use only.
where it hurts: an alternative approach to Relationship between T cell activation and of CTLA-4 are linked to loss of
HIV vaccine design. Trends Immunol CD4+ T cell count in HIV-seropositive antigen-specific CD4 T cells during
2006;27(11):504-10 individuals with undetectable plasma HIV primary human immunodeficiency
RNA levels in the absence of therapy. virus type 1 infection. J Virol
96. Migueles SA, Laborico AC, Imamichi H,
J Infect Dis 2008;197(1):126-33 2006;80(20):10162-72
et al. The differential ability of HLA
B*5701+ long-term nonprogressors and 106. Rey-Cuille MA, Berthier JL, 116. von Boehmer H. Mechanisms of
progressors to restrict human Bomsel-Demontoy MC, et al. Simian suppression by suppressor T cells.
immunodeficiency virus replication is immunodeficiency virus replicates to high Nat Immunol 2005;6(4):338-44
not caused by loss of recognition of levels in sooty mangabeys without inducing 117. Wang HY, Wang RF. Regulatory T cells
autologous viral gag sequences. disease. J Virol 1998;72(5):3872-86 and cancer. Curr Opin Immunol
J Virol 2003;77(12):6889-98 107. Chase AJ, Sedaghat AR, German JR, et al. 2007;19(2):217-23
97. Boaz MJ, Waters A, Murad S, et al. Severe depletion of CD4+CD25+ regulatory 118. Curiel TJ, Coukos G, Zou L, et al. Specific
Presence of HIV-1 Gag-specific T cells from the intestinal lamina propria recruitment of regulatory T cells in ovarian
IFN-γ+IL-2+ and CD28+IL-2+ CD4 T cell but not peripheral blood or lymph nodes carcinoma fosters immune privilege and
responses is associated with nonprogression during acute SIV infection. J Virol predicts reduced survival. Nat Med
in HIV-1 infection. J Immunol 2007;81(23):12748-57 2004;10(9):942-9
2002;169(11):6376-85 108. Day CL, Kaufmann DE, Kiepiela P, 119. Sato E, Olson SH, Ahn J, et al.
98. Harari A, Vallelian F, Meylan PR, et al. et al. PD-1 expression on HIV-specific Intraepithelial CD8+ tumor-infiltrating
Functional heterogeneity of memory CD4 T cells is associated with T-cell lymphocytes and a high CD8+/regulatory
T cell responses in different conditions exhaustion and disease progression. T cell ratio are associated with favorable
of antigen exposure and persistence. Nature 2006);443(7109):350-4 prognosis in ovarian cancer. Proc Natl Acad
J Immunol 2005;174(2):1037-45 109. Petrovas C, Casazza JP, Brenchley JM, et al. Sci USA 2005;102(51):18538-43
99. Younes SA, Yassine-Diab B, Dumont AR, PD-1 is a regulator of virus-specific CD8+ 120. de St Groth BF, Landay AL. Regulatory
et al. HIV-1 viremia prevents the T cell survival in HIV infection. J Exp Med T cells in HIV infection: pathogenic or
establishment of interleukin 2-producing 2006;203(10):2281-92 protective participants in the immune
HIV-specific memory CD4+ T cells 110. Trautmann L, Janbazian L, Chomont N, response? AIDS 2008;22(6):671-83
endowed with proliferative capacity. et al. Upregulation of PD-1 expression on 121. Andersson J, Boasso A, Nilsson J, et al.
J Exp Med 2003;198(12):1909-22 HIV-specific CD8+ T cells leads to The prevalence of regulatory T cells in
100. Tilton JC, Luskin MR, Johnson AJ, et al. reversible immune dysfunction. Nat Med lymphoid tissue is correlated with viral
Changes in paracrine interleukin-2 2006;12(10):1198-202 load in HIV-infected patients. J Immunol
requirement, CCR7 expression, frequency, 111. Zhang JY, Zhang Z, Wang X, et al. 2005;174(6):3143-7
and cytokine secretion of human PD-1 up-regulation is correlated with
68 Expert Opin. Biol. Ther. (2009) 9(1)
Baker, Block, Rothchild & Walker
122. Montes M, Lewis DE, Sanchez C, 126. Telenti A, Goldstein DB. Genomics Affiliation
et al. Foxp3+ regulatory T cells in meets HIV-1. Nat Rev Microbiol BM Baker*1, BL Block*1,
antiretroviral-naive HIV patients. 2006;4(11):865-73 AC Rothchild*1 & BD Walker†1,2
Aids 2006;20(12):1669-71 127. Study IHC. International HIV
†Author for correspondence
†1Partners AIDS Research Center,
123. Pitisuttithum P, Gilbert P, Gurwith M, Controllers Study website. 2007.
et al. Randomized, double-blind, Available from: http://www.hivcontrollers.org. Massachusetts General Hospital and
placebo-controlled efficacy trial of a [Last accessed 27 October 2008] Division of AIDS,
bivalent recombinant glycoprotein 120 Harvard Medical School,
128. Fellay J, Shianna KV, Ge D, et al.
HIV-1 vaccine among injection drug users 149 13th Street, Room 5212D,
A whole-genome association study of major
in Bangkok, Thailand. J Infect Dis Charlestown, MA 02129, Boston, USA
determinants for host control of HIV-1.
2006;194(12):1661-71 Tel: +1 617 724 8332; Fax: +1 617 726 4691;
Science 2007;317(5840):944-7
E-mail: bwalker@partners.org
124. HIV vaccine failure prompts Merck to halt 129. Han Y, Lai J, Barditch-Crovo P, et al. The 2Howard Hughes Medical Institute,
trial. Nature 2007;449(7161):390 role of protective HCP5 and HLA-C MD 20815, Chevy Chase, USA
125. Cohen J. Retrovirus meeting. Back-to-basics associated polymorphisms in the control of
Expert Opin. Biol. Ther. Downloaded from informahealthcare.com by Selcuk Universitesi on 02/11/15
*These authors contributed equally to this work
push as HIV prevention struggles. HIV-1 replication in a subset of elite
Science 2008;319(5865):888 suppressors. AIDS 2008;22(4):541-4
For personal use only.
Expert Opin. Biol. Ther. (2009) 9(1) 69
You might also like
- HIVPreventionVaccines FS enDocument2 pagesHIVPreventionVaccines FS enGV Elaugos De LeonNo ratings yet
- Perspective: New England Journal MedicineDocument3 pagesPerspective: New England Journal Medicineerika quitianNo ratings yet
- A4 - TRACE Brochure Web 1Document4 pagesA4 - TRACE Brochure Web 1hmounguiNo ratings yet
- Topic 6 HIV DiagnosisDocument30 pagesTopic 6 HIV DiagnosisPhilip MutuaNo ratings yet
- Self-Reported Adherence To Antiretroviral Therapy in HIV+ Colombian PopulationDocument7 pagesSelf-Reported Adherence To Antiretroviral Therapy in HIV+ Colombian PopulationnukarevaNo ratings yet
- Laboratory Diagnosis of Virus DiseasesDocument21 pagesLaboratory Diagnosis of Virus DiseasesVictor CostaNo ratings yet
- Computational Tools For Modern Vaccine DevelopmentDocument14 pagesComputational Tools For Modern Vaccine DevelopmentShahbaz AhmedNo ratings yet
- Mucosal Immunity in Viral DX Ann Immunol 2016Document37 pagesMucosal Immunity in Viral DX Ann Immunol 2016prasannasimhaNo ratings yet
- Sample Powerpoint Presentations: 1. The Essentials of Hiv and AidsDocument27 pagesSample Powerpoint Presentations: 1. The Essentials of Hiv and AidsAiman ButtNo ratings yet
- Viral VaccinesDocument7 pagesViral VaccinesMoon nieNo ratings yet
- Scaling Up Human Immunodeficiency Virus Screening.11Document7 pagesScaling Up Human Immunodeficiency Virus Screening.11DikshaNo ratings yet
- Review: Prevalence of Cognitive DisordersDocument10 pagesReview: Prevalence of Cognitive DisordersMartha OktaviaNo ratings yet
- Evaluation of Rapid Diagnostic Test Compared WithDocument4 pagesEvaluation of Rapid Diagnostic Test Compared WithHidenNo ratings yet
- Abbott Realtime Hiv-1: Key To Symbols UsedDocument11 pagesAbbott Realtime Hiv-1: Key To Symbols UsedNavin GuptaNo ratings yet
- MainDocument26 pagesMainRETNO GUMELARNo ratings yet
- An of Novel Adjuvants Designed For Improving Vaccine Ef FicacyDocument23 pagesAn of Novel Adjuvants Designed For Improving Vaccine Ef Ficacymi.miriyahoo.comNo ratings yet
- Integral Backstepping and Synergetic Control For Tracking of Infected Cells During Early Antiretroviral Therapy PDFDocument9 pagesIntegral Backstepping and Synergetic Control For Tracking of Infected Cells During Early Antiretroviral Therapy PDFSamama ZafarNo ratings yet
- Pathogenic Mechanisms of HIV Disease: FurtherDocument28 pagesPathogenic Mechanisms of HIV Disease: FurtherSefren TumilaarNo ratings yet
- CH 142 Antimicrobial Stewardship in Office PracticeDocument10 pagesCH 142 Antimicrobial Stewardship in Office Practiceroshen02No ratings yet
- NCP Sangalang PDFDocument3 pagesNCP Sangalang PDFCamille Joy BaliliNo ratings yet
- ZOOL 143 Topic 7 Detection of HIV Infection 1Document10 pagesZOOL 143 Topic 7 Detection of HIV Infection 1nattydreadfathelahNo ratings yet
- Antiviral Neutralizing Antibodies: From in Vitro To in Vivo ActivityDocument15 pagesAntiviral Neutralizing Antibodies: From in Vitro To in Vivo ActivityCher IshNo ratings yet
- DescargarDocument14 pagesDescargarDelia JMNo ratings yet
- Cover StoryDocument3 pagesCover StoryaggarsandeepNo ratings yet
- Autoimmunity and Covid-19Document21 pagesAutoimmunity and Covid-19laboratorium spektrumNo ratings yet
- AskrpDocument6 pagesAskrpNia marethaNo ratings yet
- Viral Vectors SlideDocument16 pagesViral Vectors SlideTemidayoNo ratings yet
- Economic Importance of VirusesDocument24 pagesEconomic Importance of VirusesFakhir Rahmani100% (2)
- HIV Vaccine Basics May 2019Document21 pagesHIV Vaccine Basics May 2019Priyo SadewoNo ratings yet
- Non-Invasive Diagnosis and Follow-Up of Chronic Infection With Hepatitis B Virus.Document10 pagesNon-Invasive Diagnosis and Follow-Up of Chronic Infection With Hepatitis B Virus.Laura Valentina GarcíaNo ratings yet
- Ast Booklet GB Final PDFDocument19 pagesAst Booklet GB Final PDFAhmed GaberNo ratings yet
- COVID-19 Vaccine - RBDocument15 pagesCOVID-19 Vaccine - RBRajNo ratings yet
- Vih GuidlineDocument21 pagesVih GuidlineDavid MonroyNo ratings yet
- Pharmaceuticals 14 00417 v2Document27 pagesPharmaceuticals 14 00417 v2Mida AdinaNo ratings yet
- Vaccine Development Strategies For Improving Immunization: The Role of Modern ImmunologyDocument6 pagesVaccine Development Strategies For Improving Immunization: The Role of Modern ImmunologyVya PrabandariNo ratings yet
- Ni 1296Document6 pagesNi 1296Samer ShamshadNo ratings yet
- Clinical Diagnostic Testing For Human CytomegalovirusDocument12 pagesClinical Diagnostic Testing For Human Cytomegalovirusdossantoselaine212No ratings yet
- 1 s2.0 S1201971223000255 MainDocument12 pages1 s2.0 S1201971223000255 MainArie RahadiNo ratings yet
- 10 1016@j Prosdent 2020 04 001Document8 pages10 1016@j Prosdent 2020 04 001Luis Miguel ValenciaNo ratings yet
- Syndemics in Patients With HIVDocument11 pagesSyndemics in Patients With HIVantinoo888No ratings yet
- 1 - PPT Dr. Agnes R. Indrati KONAS 2022Document33 pages1 - PPT Dr. Agnes R. Indrati KONAS 2022Mustakim DuharingNo ratings yet
- Bahan Ajar Meniere 2Document4 pagesBahan Ajar Meniere 2Afri AdiNo ratings yet
- Guillain-Barré Syndrome. 2023Document30 pagesGuillain-Barré Syndrome. 2023Arbey Aponte PuertoNo ratings yet
- Diagnostic Virology: Special Section: Medical MicrobiologyDocument13 pagesDiagnostic Virology: Special Section: Medical MicrobiologyEl FatihNo ratings yet
- Infection Control BasicsDocument10 pagesInfection Control BasicsAlan Amato100% (1)
- Harnessing B Cell Responses For Personalized Approaches in HIV ManagementDocument15 pagesHarnessing B Cell Responses For Personalized Approaches in HIV ManagementKIU PUBLICATION AND EXTENSIONNo ratings yet
- TB2 EFA AhmadFuadi 43219110142Document4 pagesTB2 EFA AhmadFuadi 43219110142Fuadi AhmadNo ratings yet
- TN - Diagnosing Infectious Diseases - INFOGRAPHICDocument1 pageTN - Diagnosing Infectious Diseases - INFOGRAPHICmicrobehunter007No ratings yet
- Functional Cure of Hiv Using Crispr - Adlene Jenitta, Vikrant Thokchom, W. Jasmine Karunya Institute of Technology and Sciences, CoimbatoreDocument2 pagesFunctional Cure of Hiv Using Crispr - Adlene Jenitta, Vikrant Thokchom, W. Jasmine Karunya Institute of Technology and Sciences, CoimbatoreRaj WillseeNo ratings yet
- 1 s2.0 S156757692031105X Main DikonversiDocument25 pages1 s2.0 S156757692031105X Main DikonversiAida H.djamhuriNo ratings yet
- Ni Hms 612555Document14 pagesNi Hms 612555romanNo ratings yet
- HIV/AIDS: Biology and Treatment: Learning ObjectivesDocument10 pagesHIV/AIDS: Biology and Treatment: Learning Objectiveschrispine ochiengNo ratings yet
- Differentiation Systematic: LiteratureDocument7 pagesDifferentiation Systematic: LiteratureDewi DelfienellaNo ratings yet
- Bio Factsheet: The Biology of HIVDocument3 pagesBio Factsheet: The Biology of HIVAriful IslamNo ratings yet
- Australian National Guidelines For The Management of Health Care Workers Known To Be Infected With Blood-Borne Viruses.Document24 pagesAustralian National Guidelines For The Management of Health Care Workers Known To Be Infected With Blood-Borne Viruses.Rincy MartinNo ratings yet
- Hiv GeneralidadesDocument6 pagesHiv GeneralidadesJoel MartinNo ratings yet
- Immune Response in Hepatitis B Virus InfectionDocument18 pagesImmune Response in Hepatitis B Virus InfectionaaryaachokshiNo ratings yet
- Digital Health in Enhancing Antiretroviral Therapy Adherence A Systematic Review and Meta AnalysisDocument10 pagesDigital Health in Enhancing Antiretroviral Therapy Adherence A Systematic Review and Meta AnalysisTeam DIVANo ratings yet
- HIV Epidemics in the European Region: Vulnerability and ResponseFrom EverandHIV Epidemics in the European Region: Vulnerability and ResponseNo ratings yet
- SPM 2019 Tips V1Document45 pagesSPM 2019 Tips V1Cikgu RafiNo ratings yet
- Rast TutorialDocument10 pagesRast TutorialPeter JustinNo ratings yet
- Suc Biology F4 VNotes 2017 PDFDocument32 pagesSuc Biology F4 VNotes 2017 PDFPang Chuan KianNo ratings yet
- Brochure Guide To QPCR IN70200CDocument114 pagesBrochure Guide To QPCR IN70200Cprakush_prakushNo ratings yet
- 336 EngDocument158 pages336 EngMahdi HayNo ratings yet
- Infections FlyerDocument2 pagesInfections FlyerPeter JustinNo ratings yet
- Infections FlyerDocument2 pagesInfections FlyerPeter JustinNo ratings yet
- Pathogenesis of HIVDocument11 pagesPathogenesis of HIVPeter JustinNo ratings yet
- AST 2 - FastCloning2Document9 pagesAST 2 - FastCloning2Peter JustinNo ratings yet
- Cell Organelle Homework PacketDocument24 pagesCell Organelle Homework PacketPeter JustinNo ratings yet
- MbbsDocument1 pageMbbsPeter JustinNo ratings yet
- Appa Poem PresentationDocument6 pagesAppa Poem PresentationPeter JustinNo ratings yet
- HIV - WikipediaDocument27 pagesHIV - WikipediaChandrashekhar SinghNo ratings yet
- Tropical Infectious Diseases PDFDocument1,788 pagesTropical Infectious Diseases PDFMax Izarra Almonacid0% (1)
- Cluster of Differentiation Antigen PosterDocument1 pageCluster of Differentiation Antigen PosterReeti R. Bhat100% (1)
- ACE3 Exp PDFDocument6 pagesACE3 Exp PDFVinodh VijayanNo ratings yet
- Aptamers in HIV Research Diagnosis and TherapyDocument11 pagesAptamers in HIV Research Diagnosis and TherapymikiNo ratings yet
- Anti Viral DrugsDocument70 pagesAnti Viral DrugsDereje DZ100% (2)
- Directorate of Learning Systems Directorate of Learning SystemsDocument50 pagesDirectorate of Learning Systems Directorate of Learning SystemsMatin Ahmad KhanNo ratings yet
- Herron Evolutionary Analysis 5eDocument7 pagesHerron Evolutionary Analysis 5eJose Angel Valdez Jr.No ratings yet
- A Reconstructed Historical Aetiology of The Sars-Cov-2 SpikeDocument8 pagesA Reconstructed Historical Aetiology of The Sars-Cov-2 Spikemikhaelyosia100% (1)
- Pathophysiology: HIV Infection and AIDSDocument7 pagesPathophysiology: HIV Infection and AIDSmeylin SNo ratings yet
- Thesis + CoverDocument108 pagesThesis + CoverPutriAstriNo ratings yet
- McGraw-Hill Education NAPLEX Review GuideDocument77 pagesMcGraw-Hill Education NAPLEX Review Guidebobfoo100% (1)
- Male Qbank PDFDocument126 pagesMale Qbank PDFgabby_54everNo ratings yet
- Clase 1-Fisiopatología de La Artritis ReumatoideaDocument45 pagesClase 1-Fisiopatología de La Artritis ReumatoideaPercy Williams Mendoza EscobarNo ratings yet
- 3A Membranos BaltymaiDocument1 page3A Membranos BaltymaiMonika LožytėNo ratings yet
- Cancer CellDocument140 pagesCancer CellmanbastiNo ratings yet
- Immunology MCQDocument51 pagesImmunology MCQLouise Marie Palamos DamascoNo ratings yet
- Viruses 15 00107Document30 pagesViruses 15 00107Trần T. MơNo ratings yet
- Cell-Mediated Immune ResponsesDocument53 pagesCell-Mediated Immune ResponsesFarahdina UmarellaNo ratings yet
- Hiv and Aids Hiv and AidsDocument78 pagesHiv and Aids Hiv and Aidsblue_blooded23No ratings yet
- Art DrugsDocument70 pagesArt DrugsDr Daulat Ram DhakedNo ratings yet
- HIV Drug TreatmentDocument121 pagesHIV Drug TreatmentAlbert EdoNo ratings yet
- Final HIV Written ReportDocument19 pagesFinal HIV Written ReportJohara MacasindelNo ratings yet
- Mother-to-Child Transmission of HIV: Pathogenesis, Mechanisms and PathwaysDocument18 pagesMother-to-Child Transmission of HIV: Pathogenesis, Mechanisms and Pathwaysnegara ipdNo ratings yet
- AIDS Case StudyDocument4 pagesAIDS Case StudyAlexandria BrooksNo ratings yet
- Kenya Treatment GuidelinesDocument230 pagesKenya Treatment GuidelinesKevin ChapleyNo ratings yet
- Science - 20 September 2013Document131 pagesScience - 20 September 2013Marius BălanNo ratings yet
- Bahan Kuliah HIV-AIDSDocument17 pagesBahan Kuliah HIV-AIDSKiki Rizky Andani NasutionNo ratings yet
- WWW Namrata CoDocument55 pagesWWW Namrata CoMunesh SherawatNo ratings yet
- Hiv Life Cycle: Fact Sheet Number 106Document2 pagesHiv Life Cycle: Fact Sheet Number 106eviNo ratings yet