You might also like
- Natural Perfume MakingDocument6 pagesNatural Perfume MakingAnonymous aBzTQbeiNo ratings yet
- DIY Perfume LocketDocument6 pagesDIY Perfume LocketAnonymous aBzTQbei100% (1)
- Essential Oils Perfume PDFDocument2 pagesEssential Oils Perfume PDFAnonymous aBzTQbeiNo ratings yet
- PerfumDocument4 pagesPerfumAnonymous aBzTQbeiNo ratings yet
- CHART - Essential Oil Complimentary Blending Chart - LEGAL PDFDocument3 pagesCHART - Essential Oil Complimentary Blending Chart - LEGAL PDFAnonymous aBzTQbeiNo ratings yet
- 15 DIY Essential Oil Recipes For Gifts HolidaysDocument6 pages15 DIY Essential Oil Recipes For Gifts HolidaysAnonymous aBzTQbeiNo ratings yet
- Twelve Tissue Remedies of Schussler Contents and Reading ExcerptDocument13 pagesTwelve Tissue Remedies of Schussler Contents and Reading ExcerptAnonymous aBzTQbeiNo ratings yet
- CHART - Essential Oil Complimentary Blending Chart - LEGAL PDFDocument3 pagesCHART - Essential Oil Complimentary Blending Chart - LEGAL PDFAnonymous aBzTQbeiNo ratings yet
- Perfum RECIPES LEGALDocument10 pagesPerfum RECIPES LEGALAnonymous aBzTQbeiNo ratings yet
- Deluxe HH Digital Microscope Manual 5lang WebDocument55 pagesDeluxe HH Digital Microscope Manual 5lang WebAnonymous aBzTQbeiNo ratings yet
- Essential Oil Recipes - Com Confidence Perfume RecipesDocument1 pageEssential Oil Recipes - Com Confidence Perfume RecipesAnonymous aBzTQbei100% (1)
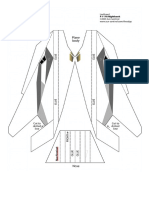
- Paper PlaneDocument1 pagePaper PlaneAnonymous aBzTQbeiNo ratings yet
- Aromatherapy Perfume RecipiesDocument19 pagesAromatherapy Perfume RecipiesAnonymous aBzTQbeiNo ratings yet
- Iridologia Psicoterapeutica VetorialDocument136 pagesIridologia Psicoterapeutica VetorialAnonymous aBzTQbei100% (1)
- Gráficos PDFDocument2 pagesGráficos PDFAnonymous aBzTQbeiNo ratings yet
- Airborne Glider 42in Oz10853Document1 pageAirborne Glider 42in Oz10853Anonymous aBzTQbeiNo ratings yet
- The Central RaceDocument22 pagesThe Central RaceJedidah100% (13)
- Aromatherapy and EpilepsyDocument4 pagesAromatherapy and EpilepsyAnonymous aBzTQbeiNo ratings yet
- Therapy For A New GenerationDocument3 pagesTherapy For A New GenerationAnonymous aBzTQbeiNo ratings yet
- Aromatherapy-Therapeutic Uses PDFDocument46 pagesAromatherapy-Therapeutic Uses PDFsachin.daga881No ratings yet
- ESense Skin Response Manual enDocument53 pagesESense Skin Response Manual enAnonymous aBzTQbeiNo ratings yet
- Therapy For A New GenerationDocument3 pagesTherapy For A New GenerationAnonymous aBzTQbeiNo ratings yet
- Aromatherapy Hand Massage Aromatherapy - GradworksDocument171 pagesAromatherapy Hand Massage Aromatherapy - GradworksAnonymous aBzTQbeiNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Goals of Prenatal CareDocument16 pagesGoals of Prenatal CareLhea Marie Trinidad100% (1)
- Peri ImplantitisDocument11 pagesPeri ImplantitisMuhammad GhifariNo ratings yet
- Research Interest Potential Advisors International StudentsDocument12 pagesResearch Interest Potential Advisors International StudentsAKREDITASI RS KOTA SERANGNo ratings yet
- Deciding When To Submit A 510 (K) For A Change To An Existing Device - Guidance For Industry and Food and Drug Administration StaffDocument77 pagesDeciding When To Submit A 510 (K) For A Change To An Existing Device - Guidance For Industry and Food and Drug Administration StaffsomzNo ratings yet
- The Impact of Nutrition Education On Knowledge, Attitude, and Practiceregarding Iron Deficiency Anemia Among Female Adolescent Studentsin JordanDocument7 pagesThe Impact of Nutrition Education On Knowledge, Attitude, and Practiceregarding Iron Deficiency Anemia Among Female Adolescent Studentsin JordanAppierien 4No ratings yet
- Antenatal CareDocument11 pagesAntenatal CareManasi ChaskarNo ratings yet
- What Is Medical DeontologyDocument11 pagesWhat Is Medical DeontologyExorticNo ratings yet
- Telemetry Recognition WorkbookDocument29 pagesTelemetry Recognition WorkbookQueenNo ratings yet
- Current Status of Child Health in IndiaDocument26 pagesCurrent Status of Child Health in IndiaAmy Lalringhluani100% (3)
- Air Quality Guidelines For EuropeDocument288 pagesAir Quality Guidelines For EuropeAlex OliveiraNo ratings yet
- Banking - Diksha Book On Effective Study Techniques PDFDocument66 pagesBanking - Diksha Book On Effective Study Techniques PDFHemrajSainiNo ratings yet
- Household 1Document2 pagesHousehold 1ainun rapikaNo ratings yet
- Pediatrics Wards History Taking TemplateDocument2 pagesPediatrics Wards History Taking TemplateBobet Reña80% (5)
- Nursing Care Plan Output (NCP) 50 Points: Activity 14Document2 pagesNursing Care Plan Output (NCP) 50 Points: Activity 14Nathaniel Pulido50% (2)
- f3 November Monthly TestDocument16 pagesf3 November Monthly TestNaqi SDARNo ratings yet
- Nursing Care PlanDocument4 pagesNursing Care PlanAde HerlambangNo ratings yet
- Ab'Asanas (Expanded & Updated)Document56 pagesAb'Asanas (Expanded & Updated)Nicola AvonNo ratings yet
- Emergency ManagementDocument78 pagesEmergency ManagementHuey Calabines50% (2)
- AnemiaDocument33 pagesAnemiaDiwiasti Firdausi YasminNo ratings yet
- PE UNIT 1 Active Recreation (Lifestyle and Weight Management)Document26 pagesPE UNIT 1 Active Recreation (Lifestyle and Weight Management)Charmaine RamosNo ratings yet
- Black Book Project 3Document69 pagesBlack Book Project 3Pragya SinghNo ratings yet
- FOOTBALL (SOCCER) INJURY REPORTING FORM English WordsDocument3 pagesFOOTBALL (SOCCER) INJURY REPORTING FORM English WordsNinNo ratings yet
- 457 CBT UpdatedDocument82 pages457 CBT UpdatedDass DavidNo ratings yet
- Aat Dementia PDFDocument3 pagesAat Dementia PDFMinodora MilenaNo ratings yet
- Capillary Blood Glucose Performance Checklist: Numerical Rating Adjectival Description DescriptionDocument2 pagesCapillary Blood Glucose Performance Checklist: Numerical Rating Adjectival Description DescriptionAngeline NavarroNo ratings yet
- Textbook of Paediatric Emergency Medicine, 2ndDocument628 pagesTextbook of Paediatric Emergency Medicine, 2ndPhruek Hinhumpetch100% (1)
- EXSA - Gold Award Recipients 2006Document15 pagesEXSA - Gold Award Recipients 2006applebarrel100% (1)
- Ojs FianaDocument13 pagesOjs FianadespalitaNo ratings yet
- Approved Harmonized National RD Agenda 2017-2022 PDFDocument90 pagesApproved Harmonized National RD Agenda 2017-2022 PDFJoemel Bautista100% (1)