You might also like
- Complications in UveitisFrom EverandComplications in UveitisFrancesco PichiNo ratings yet
- Blepharitis 2934 2934Document10 pagesBlepharitis 2934 2934Marjan RobarNo ratings yet
- The Dental Pulp: Biology, Pathology, and Regenerative TherapiesFrom EverandThe Dental Pulp: Biology, Pathology, and Regenerative TherapiesNo ratings yet
- Treatment of Blepharitis Recent Clinical TrialsDocument12 pagesTreatment of Blepharitis Recent Clinical TrialsSandra PeñuelaNo ratings yet
- Clinical Practice: Treatment of Blepharitis: Recent Clinical TrialsDocument12 pagesClinical Practice: Treatment of Blepharitis: Recent Clinical TrialsKevin RayadiNo ratings yet
- Medical Management of BlepharitisDocument6 pagesMedical Management of BlepharitisAl NaifNo ratings yet
- Jovr 6 3 192Document8 pagesJovr 6 3 192Felicia JesslynNo ratings yet
- Dry EyeDocument25 pagesDry Eye215045 zulfa laili aNo ratings yet
- An Insight Into Meibomian Gland DysfunctionDocument22 pagesAn Insight Into Meibomian Gland DysfunctionvalbayerosNo ratings yet
- Jovr 6 3 192 PDFDocument7 pagesJovr 6 3 192 PDFShofura AzizahNo ratings yet
- What Is The Best Treatment Approach For Severe Blepharitis?: Key Words: Blepharitis ClinicalDocument3 pagesWhat Is The Best Treatment Approach For Severe Blepharitis?: Key Words: Blepharitis ClinicalnicoNo ratings yet
- Ophthalmic-Blepharitis-A Short Note-Vinod Singh-Rizwan-Ahmad-Mamta-Farswan-SinghDocument6 pagesOphthalmic-Blepharitis-A Short Note-Vinod Singh-Rizwan-Ahmad-Mamta-Farswan-SinghAfri AdiNo ratings yet
- Bron 2017Document73 pagesBron 2017Anggia BungaNo ratings yet
- 1 s2.0 S1542012417301349 MainextDocument75 pages1 s2.0 S1542012417301349 MainextWagner de AvizNo ratings yet
- Effects of Isotretinoin On Meibomian GlandsDocument6 pagesEffects of Isotretinoin On Meibomian GlandsTeddyNo ratings yet
- Dry Eye ThesisDocument5 pagesDry Eye ThesisPaperWritingServiceCollegeUK100% (2)
- Seasonal Monthly Variation Amongst Reported Cataract Surgeries in IndiaDocument92 pagesSeasonal Monthly Variation Amongst Reported Cataract Surgeries in IndiafriendsofindiaNo ratings yet
- Blepharitis - UpToDateDocument22 pagesBlepharitis - UpToDateanisa maria ulfaNo ratings yet
- TaiwanJOphthalmol000-3647805 100758Document11 pagesTaiwanJOphthalmol000-3647805 100758arnanda raizhaNo ratings yet
- Effect of 808-nm Laser Photobiomodulation Treatment in Blepharitis Rat ModelDocument6 pagesEffect of 808-nm Laser Photobiomodulation Treatment in Blepharitis Rat ModelselcanekicierNo ratings yet
- Metabolomics and Lipidomics Approaches in Human TeDocument15 pagesMetabolomics and Lipidomics Approaches in Human TeanxNo ratings yet
- FinalDocument105 pagesFinalBharath BalagaNo ratings yet
- Answer To Ophthaproblem 2. Filamentary KeratitisDocument1 pageAnswer To Ophthaproblem 2. Filamentary KeratitisKoas Saraf Angkatan 96No ratings yet
- Article 2-1619577119Document13 pagesArticle 2-1619577119Omnia ZapharusNo ratings yet
- E000943 Full PDFDocument9 pagesE000943 Full PDFAmayliahNo ratings yet
- Dry Eye: A Protein Conformational Disease: Biochemistry and Molecular BiologyDocument7 pagesDry Eye: A Protein Conformational Disease: Biochemistry and Molecular BiologyAlinaNo ratings yet
- Lit Review - Contact Lens Associated Pseudomonas KeratitisDocument8 pagesLit Review - Contact Lens Associated Pseudomonas KeratitisAlien4mearthNo ratings yet
- Dry Eye 1Document4 pagesDry Eye 1Leonardo JeversonNo ratings yet
- Graves 508Document6 pagesGraves 508VellaNo ratings yet
- Modern Approach To The Treatment of Dry Eye, A Complex Multifactorial Disease: A P.I.C.A.S.S.O. Board ReviewDocument8 pagesModern Approach To The Treatment of Dry Eye, A Complex Multifactorial Disease: A P.I.C.A.S.S.O. Board Reviewichmatul oktaveniNo ratings yet
- Dry Eye Syndrome - Diagnosis and Management: Dr. Jeffrey CF PONGDocument3 pagesDry Eye Syndrome - Diagnosis and Management: Dr. Jeffrey CF PONGVeronica Yosita AnandaNo ratings yet
- Blepharitis - UpToDateDocument38 pagesBlepharitis - UpToDatecamiloedaza1977No ratings yet
- Modern Approach To The Treatment of Dry Eye, A Complex Multifactorial Disease: A P.I.C.A.S.S.O. Board ReviewDocument8 pagesModern Approach To The Treatment of Dry Eye, A Complex Multifactorial Disease: A P.I.C.A.S.S.O. Board ReviewStephanie AureliaNo ratings yet
- Pterygium 2022Document16 pagesPterygium 2022Jose A BolivarNo ratings yet
- Modern Approach To The Treatment of Dry EyeDocument8 pagesModern Approach To The Treatment of Dry EyeAsma BronkialeNo ratings yet
- OpthaDocument5 pagesOpthavarun2k6No ratings yet
- Modern Approach To The Treatment of Dry EyeDocument8 pagesModern Approach To The Treatment of Dry EyePutri kartiniNo ratings yet
- Pathophysiology: United StatesDocument11 pagesPathophysiology: United StatesNurullia RahmawatiNo ratings yet
- Dry Eye Syndrome - StatPearls - NCBI Bookshelf PDFDocument7 pagesDry Eye Syndrome - StatPearls - NCBI Bookshelf PDFnum padNo ratings yet
- Tgs ReferatDocument44 pagesTgs ReferatlieNo ratings yet
- The Control of Conjunctival Fibrosis As A Paradigm For The Prevention of Ocular Fibrosis-Related Blindness. "Fibrosis Has Many Friends"Document12 pagesThe Control of Conjunctival Fibrosis As A Paradigm For The Prevention of Ocular Fibrosis-Related Blindness. "Fibrosis Has Many Friends"Ginda Chitra PuspitaNo ratings yet
- Bodh 2011Document8 pagesBodh 2011syramadhantiNo ratings yet
- 2022 Baricitinib Liposomes As A New Approach For The Treatment of Sjögren's SyndromeDocument20 pages2022 Baricitinib Liposomes As A New Approach For The Treatment of Sjögren's SyndromemrsilNo ratings yet
- Severe Dry EyeDocument6 pagesSevere Dry EyeAnggia BungaNo ratings yet
- Dry Eye ManagementDocument8 pagesDry Eye ManagementMul YaniNo ratings yet
- CITITDocument8 pagesCITITIoana ElenaNo ratings yet
- 1 s2.0 S0002939412000669 MainDocument1 page1 s2.0 S0002939412000669 MainCupris23No ratings yet
- Mcginn I Gle 2012Document24 pagesMcginn I Gle 2012Keren A. RajaNo ratings yet
- Suppurative KeratitisDocument30 pagesSuppurative KeratitisTatik Handayani100% (1)
- Adult BlepharitisDocument11 pagesAdult BlepharitistrisnatersinandaNo ratings yet
- Modern Approach To The Treatment of Dry Eye, A Complex Multifactorial Disease: A P.I.C.A.S.S.O. Board ReviewDocument8 pagesModern Approach To The Treatment of Dry Eye, A Complex Multifactorial Disease: A P.I.C.A.S.S.O. Board ReviewdiancahyaNo ratings yet
- ProstesisDocument9 pagesProstesisjuslan kasmarNo ratings yet
- The Power of Tears How Tear Proteomics Research Could Revolutionize The ClinicDocument4 pagesThe Power of Tears How Tear Proteomics Research Could Revolutionize The ClinicAlinaNo ratings yet
- Vernal Keratoconjunctivitis: Mast Cell StabilizersDocument1 pageVernal Keratoconjunctivitis: Mast Cell StabilizersIntan MayangsariNo ratings yet
- Ocular Hypotony - A Comprehensive ReviewDocument20 pagesOcular Hypotony - A Comprehensive ReviewJavier Infantes MolinaNo ratings yet
- Vitreomacular Traction SyndromeDocument15 pagesVitreomacular Traction SyndromeCamila Andrea Gutiérrez CandiaNo ratings yet
- False Myths Versus Medical Facts: Ten Common Misconceptions Related To Dry Eye DiseaseDocument10 pagesFalse Myths Versus Medical Facts: Ten Common Misconceptions Related To Dry Eye DiseaseEduardo PiresNo ratings yet
- JurnalDocument18 pagesJurnalJean UsmanyNo ratings yet
- Prevention of Blindness in Leprosy: An Overview of The Relevant Clinical and Programme-Planning IssuesDocument9 pagesPrevention of Blindness in Leprosy: An Overview of The Relevant Clinical and Programme-Planning IssuesBudi KhangNo ratings yet
- International Journal of Surgery OpenDocument4 pagesInternational Journal of Surgery OpenPerdana SihiteNo ratings yet
- 2017 AHA Kawasaki DiseaseDocument74 pages2017 AHA Kawasaki DiseaseEdwin WijayaNo ratings yet
- Jaga 18-24 NovDocument2 pagesJaga 18-24 NovnicoNo ratings yet
- Lion Air Eticket Itinerary / Receipt: Hutagaol/Nicolas Trivolta MRDocument3 pagesLion Air Eticket Itinerary / Receipt: Hutagaol/Nicolas Trivolta MRnicoNo ratings yet
- Kjped 57 479Document6 pagesKjped 57 479nicoNo ratings yet
- 2017 AHA Kawasaki DiseaseDocument74 pages2017 AHA Kawasaki DiseaseEdwin WijayaNo ratings yet
- Lion Air Eticket Itinerary / Receipt: Hutagaol/Nicolas Trivolta MRDocument3 pagesLion Air Eticket Itinerary / Receipt: Hutagaol/Nicolas Trivolta MRnicoNo ratings yet
- Lion Air Eticket Itinerary / Receipt: Hutagaol/Nicolas Trivolta MRDocument3 pagesLion Air Eticket Itinerary / Receipt: Hutagaol/Nicolas Trivolta MRnicoNo ratings yet
- Nicolas Trivolta Hutagaol-Pku-Mdvzcl-Kno-Flight - Originating PDFDocument2 pagesNicolas Trivolta Hutagaol-Pku-Mdvzcl-Kno-Flight - Originating PDFnicoNo ratings yet
- Contoh 2Document10 pagesContoh 2nugroho2212No ratings yet
- Itchy Eyes Case Study: Eye Series - 17Document2 pagesItchy Eyes Case Study: Eye Series - 17nicoNo ratings yet
- Status OftalmikusDocument2 pagesStatus OftalmikusnicoNo ratings yet
- WWW - Unlock PDF - Com RATNASARIDocument12 pagesWWW - Unlock PDF - Com RATNASARIPutraNo ratings yet
- 1 PB PDFDocument4 pages1 PB PDFnicoNo ratings yet
- What Is The Best Treatment Approach For Severe Blepharitis?: Key Words: Blepharitis ClinicalDocument3 pagesWhat Is The Best Treatment Approach For Severe Blepharitis?: Key Words: Blepharitis ClinicalnicoNo ratings yet
- ABSTRACT ADocument2 pagesABSTRACT AnicoNo ratings yet
- Presentations Day 1 - Session 1 - Presentation 06 - Sri LankaDocument29 pagesPresentations Day 1 - Session 1 - Presentation 06 - Sri LankaAnkur MishraNo ratings yet
- DIY Mineral MakeupDocument1 pageDIY Mineral MakeupDirek JP NinalgaNo ratings yet
- Data Legacy InsuranceCos SourceRSDocument48 pagesData Legacy InsuranceCos SourceRSrishu1527No ratings yet
- Intrebari Interviu Asistent MedicalDocument3 pagesIntrebari Interviu Asistent MedicalanaNo ratings yet
- Common Causes of Calf Pain in Endurance Athletes: by Brad J. Bernardini, MD, FAAOS, Reconstructive OrthopedicsDocument2 pagesCommon Causes of Calf Pain in Endurance Athletes: by Brad J. Bernardini, MD, FAAOS, Reconstructive Orthopedicsbila inunNo ratings yet
- 48069B - Ferrofos 5260 (GB-ENG)Document6 pages48069B - Ferrofos 5260 (GB-ENG)danielNo ratings yet
- Flux Cored Arc Welding NC IIDocument73 pagesFlux Cored Arc Welding NC IIAJ AcuñaNo ratings yet
- BD Product ListDocument48 pagesBD Product Listanish_10677953100% (1)
- Persona Partial Knee Brochure PDFDocument12 pagesPersona Partial Knee Brochure PDF洪侊增No ratings yet
- Zinc in Wound Healing Theoretical, ExperimentalDocument15 pagesZinc in Wound Healing Theoretical, ExperimentalRifky Budi TriyatnoNo ratings yet
- PERDEV DLL Unit 1 - M3 (Developmental Stages Handout)Document4 pagesPERDEV DLL Unit 1 - M3 (Developmental Stages Handout)Leonila MirandaNo ratings yet
- Abnormal Illness BehaviorDocument7 pagesAbnormal Illness Behavioransha2011p0% (1)
- Transdiagnostic TreatmentDocument9 pagesTransdiagnostic Treatmentvalentina chistrugaNo ratings yet
- Bus Man Unit 3 SAC 3Document13 pagesBus Man Unit 3 SAC 3Mohamad ZackuanNo ratings yet
- How May I Make My Penis More Robust? Answer That NowDocument2 pagesHow May I Make My Penis More Robust? Answer That NowEsbensen59TRUENo ratings yet
- UJA-Federation of New York Donor Recognition List 2022Document17 pagesUJA-Federation of New York Donor Recognition List 2022ericlkaplanNo ratings yet
- Lab # 5 Use Case and Activity Diagram: ObjectivesDocument7 pagesLab # 5 Use Case and Activity Diagram: ObjectivesmexiweNo ratings yet
- Suplemento 1Document56 pagesSuplemento 1Dessirhe LaraNo ratings yet
- Drug Dispensing Practices at Pharmacies in Bengaluru: A Cross Sectional StudyDocument5 pagesDrug Dispensing Practices at Pharmacies in Bengaluru: A Cross Sectional StudySoumya RatnalaNo ratings yet
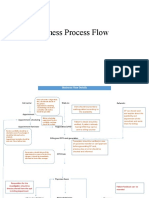
- Business Process FlowDocument12 pagesBusiness Process FlowKumar BalramNo ratings yet
- Why Is Research Important - NHS GroupDocument8 pagesWhy Is Research Important - NHS GroupRoxan PacsayNo ratings yet
- Lung Cancer Report Sample High enDocument1 pageLung Cancer Report Sample High enSiddhesh PawarNo ratings yet
- Smith Slides CH 4Document26 pagesSmith Slides CH 4USHA RANI SONOWALNo ratings yet
- Open Versus Closed Kinetic Chain Exercises For Patellofemoral Pain Syndrome - TsaiDocument44 pagesOpen Versus Closed Kinetic Chain Exercises For Patellofemoral Pain Syndrome - TsaiBaykal Çelik100% (1)
- HSC 430 - Lesson Plan Underage DrinkingDocument11 pagesHSC 430 - Lesson Plan Underage Drinkingapi-487139726No ratings yet
- Effect of Human Papilloma Virus in HIV Infected Person: A Mini ReviewDocument7 pagesEffect of Human Papilloma Virus in HIV Infected Person: A Mini ReviewKIH 20162017No ratings yet
- Complete Guide To Communication Problems After StrokeDocument22 pagesComplete Guide To Communication Problems After Strokeapi-215453798100% (1)
- Position Paper TopicsDocument2 pagesPosition Paper TopicskinodecuirNo ratings yet
- Department of Education: Granja Kalinawan National High SchoolDocument26 pagesDepartment of Education: Granja Kalinawan National High SchoolRoselyn Mae DulaNo ratings yet
- Feline Injection-Site Sarcoma - Todays Veterinary PracticeDocument12 pagesFeline Injection-Site Sarcoma - Todays Veterinary PracticeBla bla BlaNo ratings yet
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (403)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (20)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 4 out of 5 stars4/5 (5)
- Breaking the Habit of Being YourselfFrom EverandBreaking the Habit of Being YourselfRating: 4.5 out of 5 stars4.5/5 (1457)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)
- The Happiest Baby on the Block: The New Way to Calm Crying and Help Your Newborn Baby Sleep LongerFrom EverandThe Happiest Baby on the Block: The New Way to Calm Crying and Help Your Newborn Baby Sleep LongerRating: 4.5 out of 5 stars4.5/5 (58)
- How to Talk to Anyone: Learn the Secrets of Good Communication and the Little Tricks for Big Success in RelationshipFrom EverandHow to Talk to Anyone: Learn the Secrets of Good Communication and the Little Tricks for Big Success in RelationshipRating: 4.5 out of 5 stars4.5/5 (1135)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- Peaceful Sleep Hypnosis: Meditate & RelaxFrom EverandPeaceful Sleep Hypnosis: Meditate & RelaxRating: 4.5 out of 5 stars4.5/5 (142)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisFrom EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisRating: 3.5 out of 5 stars3.5/5 (2)
- Summary of The 4-Hour Body: An Uncommon Guide to Rapid Fat-Loss, Incredible Sex, and Becoming Superhuman by Timothy FerrissFrom EverandSummary of The 4-Hour Body: An Uncommon Guide to Rapid Fat-Loss, Incredible Sex, and Becoming Superhuman by Timothy FerrissRating: 4.5 out of 5 stars4.5/5 (81)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (44)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)