You might also like
- Scolio SIS: Submitted ToDocument10 pagesScolio SIS: Submitted Tojean thereseNo ratings yet
- ScoliosisDocument4 pagesScoliosisDharline Abbygale Garvida AgullanaNo ratings yet
- SCOLIOSISDocument19 pagesSCOLIOSISEspers BluesNo ratings yet
- ScoliosisDocument3 pagesScoliosisannkramNo ratings yet
- Case Presentation ScoliosisDocument7 pagesCase Presentation ScoliosisKhrizjan RebloraNo ratings yet
- ScoliosisDocument25 pagesScoliosisshanel18100% (1)
- DefinitionDocument25 pagesDefinitiondjustiela karrangNo ratings yet
- Types of Spine Curvature DisordersDocument7 pagesTypes of Spine Curvature DisordersNicu MacariNo ratings yet
- About:: Birth Defects Muscular Dystrophy, Cerebral Palsy Marfan's DiseaseDocument4 pagesAbout:: Birth Defects Muscular Dystrophy, Cerebral Palsy Marfan's DiseaseAbie BeyNo ratings yet
- LimpDocument7 pagesLimpRakesh DudiNo ratings yet
- Kyphosis, Lordosis, ScoliosisDocument22 pagesKyphosis, Lordosis, ScoliosisTheeya Quigao100% (1)
- SP SkoliosisDocument19 pagesSP SkoliosisSantosa OkaNo ratings yet
- Scoliosis Surgery IannnDocument8 pagesScoliosis Surgery IannnAnie ZacariasNo ratings yet
- Scoliosis: By: Manilyn B. Lin Bsn-IiiDocument13 pagesScoliosis: By: Manilyn B. Lin Bsn-IiiWillie100% (1)
- PBL SkoliosisDocument6 pagesPBL SkoliosisAgnes Stefani EffendiNo ratings yet
- Adolescent Idiopathic ScoliosisDocument29 pagesAdolescent Idiopathic ScoliosisfenskaNo ratings yet
- SCOLIOSIS CAUSES, SYMPTOMS, DIAGNOSIS AND TREATMENTDocument20 pagesSCOLIOSIS CAUSES, SYMPTOMS, DIAGNOSIS AND TREATMENTSugar Capule - ManuelNo ratings yet
- C-Shaped Curve ScoliosisDocument6 pagesC-Shaped Curve ScoliosisCharisma ElordeNo ratings yet
- Scoliosis and KyphosisDocument5 pagesScoliosis and KyphosisEufrasia VictaNo ratings yet
- ScoliosisDocument3 pagesScoliosisTracy100% (1)
- What Is KyphosisDocument6 pagesWhat Is Kyphosisسانو روديلNo ratings yet
- Overview Congenital Musculoskeletal DisorderDocument84 pagesOverview Congenital Musculoskeletal DisorderRyan Trian100% (3)
- DSA10 Scoliosis, Posture and Muscle BalanceDocument11 pagesDSA10 Scoliosis, Posture and Muscle BalanceWilliam JonesNo ratings yet
- Pediatric Scoliosis What Is Scoliosis?Document8 pagesPediatric Scoliosis What Is Scoliosis?Yak NafarNo ratings yet
- A Simple Guide to The Posture, Spine Diseases and Use in Disease DiagnosisFrom EverandA Simple Guide to The Posture, Spine Diseases and Use in Disease DiagnosisNo ratings yet
- Ankylosing LeafletfaDocument2 pagesAnkylosing LeafletfaAaron NelsonNo ratings yet
- Anomalies of Skeletal System-1Document44 pagesAnomalies of Skeletal System-1Meena KoushalNo ratings yet
- Scoliosis, (Updated) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandScoliosis, (Updated) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Congenital Abnormalities MusculoSkeletal SystemDocument116 pagesCongenital Abnormalities MusculoSkeletal SystemVii syilsaNo ratings yet
- ScoliosisDocument5 pagesScoliosisIbe JulienneNo ratings yet
- Scoliosis, Lordosis, and KyphosisDocument40 pagesScoliosis, Lordosis, and KyphosisRati W. PaneseNo ratings yet
- SCOLIOSIS Its Diagnosis and TreatmentDocument2 pagesSCOLIOSIS Its Diagnosis and TreatmentJoseph CannilloNo ratings yet
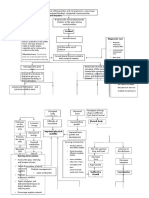
- Pathway - Skoliosis GROUPDocument12 pagesPathway - Skoliosis GROUPAnonymous NZTQVgjaNo ratings yet
- NCP ScoliosisDocument4 pagesNCP ScoliosisCharley DegamoNo ratings yet
- Adolescent Health Problems and Nursing CareDocument40 pagesAdolescent Health Problems and Nursing CaremilayosoresNo ratings yet
- Driscoll 2008Document32 pagesDriscoll 2008Anindira RustandiNo ratings yet
- ScoliosisDocument18 pagesScoliosisMj EnofnaNo ratings yet
- Share 'DEFORMITIES - PPTX'Document105 pagesShare 'DEFORMITIES - PPTX'Hunaid 1000No ratings yet
- Scoliosis Fact SheetDocument3 pagesScoliosis Fact SheetTSRHCNo ratings yet
- Understanding Scoliosis: Causes, Symptoms and TreatmentDocument5 pagesUnderstanding Scoliosis: Causes, Symptoms and TreatmentHazel Lyn Valdoz Gongora-CardozaNo ratings yet
- Orthopedic Conditions in PaedsDocument57 pagesOrthopedic Conditions in PaedsAsma AlamNo ratings yet
- Fatima Sehar-699Document6 pagesFatima Sehar-699Fatima SeharNo ratings yet
- Assessment of Posture: Prepared By: Floriza P. de Leon, PTRPDocument17 pagesAssessment of Posture: Prepared By: Floriza P. de Leon, PTRPFloriza de Leon100% (1)
- Scoliosis: Ns. M. Nurman, S.Kep Stikes Tuanku Tambusai BangkinangDocument36 pagesScoliosis: Ns. M. Nurman, S.Kep Stikes Tuanku Tambusai Bangkinangwindy noviantyNo ratings yet
- ScolioDocument2 pagesScolioJester de ChavezNo ratings yet
- Scoliosis 2023Document58 pagesScoliosis 2023ashlyn granthamNo ratings yet
- Figure FaultsDocument17 pagesFigure FaultsMichael SimpsonNo ratings yet
- ScoliosisDocument19 pagesScoliosisMia Dela CruzNo ratings yet
- Abnormal Spine CurvaturesDocument7 pagesAbnormal Spine CurvaturesMartin SageNo ratings yet
- Updateonevaluationand Treatmentofscoliosis: Ron El-Hawary,, Chukwudi ChukwunyerenwaDocument19 pagesUpdateonevaluationand Treatmentofscoliosis: Ron El-Hawary,, Chukwudi Chukwunyerenwacarla grauNo ratings yet
- Anatomy of ScoliosisDocument6 pagesAnatomy of ScoliosisDaniel MañalacNo ratings yet
- Types of Scoliosis and Treatment PlansDocument5 pagesTypes of Scoliosis and Treatment PlansMaryam YasinNo ratings yet
- Scoliosis, Lordosis, and Kyphosis GuideDocument41 pagesScoliosis, Lordosis, and Kyphosis Guidechrisamaria100% (3)
- Scoliosis: Spinal Curvature, KyphoscoliosisDocument3 pagesScoliosis: Spinal Curvature, Kyphoscoliosisiamweena17No ratings yet
- Family Medicine DepartmentDocument45 pagesFamily Medicine Departmentسليمان فايزNo ratings yet
- Scoliosis PDFDocument19 pagesScoliosis PDFdallas100% (1)
- Scoliosis Guide: Causes, Symptoms, Diagnosis & TreatmentDocument5 pagesScoliosis Guide: Causes, Symptoms, Diagnosis & TreatmentDimple Castañeto CalloNo ratings yet
- Kimberli Case StudyDocument4 pagesKimberli Case StudyLLLJJJ100% (3)
- ScolioDocument2 pagesScolioJonahh2012No ratings yet
- Musculoskeletal Dysfunction in ChildrenDocument40 pagesMusculoskeletal Dysfunction in Childrensanakhan091197No ratings yet
- IELTS Preparation GuideDocument32 pagesIELTS Preparation GuideArsl aliNo ratings yet
- Maternal Health Nageles Rule Add 7 and 9 MonthsDocument13 pagesMaternal Health Nageles Rule Add 7 and 9 MonthsReema Akberali nooraniNo ratings yet
- Resources For Optimal Care of The: Injured PatientDocument174 pagesResources For Optimal Care of The: Injured PatientReema Akberali nooraniNo ratings yet
- (Jeff - Solheim) Emergency Nursing. The Profession PDFDocument489 pages(Jeff - Solheim) Emergency Nursing. The Profession PDFDesrila Indra Sari100% (3)
- Resources For Optimal Care PDFDocument221 pagesResources For Optimal Care PDFLiezeth Ayala F100% (1)
- IELTS BAND 9 ANSWERS - 2020 - 5-8-SAMPLE - WMDocument10 pagesIELTS BAND 9 ANSWERS - 2020 - 5-8-SAMPLE - WMReema Akberali nooraniNo ratings yet
- IELTS Preparation GuideDocument32 pagesIELTS Preparation GuideArsl aliNo ratings yet
- NCLEX Cram Sheet: 1. Lab ValuesDocument7 pagesNCLEX Cram Sheet: 1. Lab ValuesReema Akberali noorani50% (2)
- Car Seat InfoDocument1 pageCar Seat InfoReema Akberali nooraniNo ratings yet
- Nutritional ScreeningDocument8 pagesNutritional ScreeningReema Akberali nooraniNo ratings yet
- Neural tube defects, pediatricDocument8 pagesNeural tube defects, pediatricReema Akberali nooraniNo ratings yet
- Nutritional ScreeningDocument8 pagesNutritional ScreeningReema Akberali nooraniNo ratings yet
- Williams TumorDocument5 pagesWilliams TumorReema Akberali nooraniNo ratings yet
- Vaginal ExaminationDocument7 pagesVaginal ExaminationReema Akberali nooraniNo ratings yet
- Williams TumorDocument5 pagesWilliams TumorReema Akberali nooraniNo ratings yet
- Scoliosis, Pediatric: Anxiety GoalDocument4 pagesScoliosis, Pediatric: Anxiety GoalReema Akberali nooraniNo ratings yet
- Scoliosis, Pediatric: Anxiety GoalDocument4 pagesScoliosis, Pediatric: Anxiety GoalReema Akberali nooraniNo ratings yet
- Nutritional ScreeningDocument8 pagesNutritional ScreeningReema Akberali nooraniNo ratings yet
- Placental ExaminationDocument5 pagesPlacental ExaminationReema Akberali nooraniNo ratings yet
- Breach PresentationDocument7 pagesBreach PresentationReema Akberali nooraniNo ratings yet
- Blood TransfusionDocument16 pagesBlood TransfusionReema Akberali nooraniNo ratings yet
- Neural tube defects, pediatricDocument8 pagesNeural tube defects, pediatricReema Akberali nooraniNo ratings yet
- Blood Transfusion ReactionDocument9 pagesBlood Transfusion ReactionReema Akberali nooraniNo ratings yet
- Pomposelli 2009Document9 pagesPomposelli 2009Bianca DianaNo ratings yet
- How Long Does A Cough Normally Last?Document4 pagesHow Long Does A Cough Normally Last?Dalveer JohnNo ratings yet
- Patient Care Plan SPVDocument55 pagesPatient Care Plan SPVCarlton Anthony George IINo ratings yet
- Self Care Inventory-Revised Version (SCI-R) : Never Rarely Sometimes Usually AlwaysDocument1 pageSelf Care Inventory-Revised Version (SCI-R) : Never Rarely Sometimes Usually Alwaysalip pamungkasNo ratings yet
- Form Form M Student Health CertificateDocument4 pagesForm Form M Student Health CertificateAnindya Wisastra Inggas AriawanNo ratings yet
- Giant Cell Tumor of The Calcaneus: A Case Report: Presented By: Nugroho Sigit HDocument22 pagesGiant Cell Tumor of The Calcaneus: A Case Report: Presented By: Nugroho Sigit HNugroho SigitNo ratings yet
- Musculoskeletal Malformations GuideDocument3 pagesMusculoskeletal Malformations GuideAmrut Lovesmusic67% (3)
- Discharge Planning FinalDocument5 pagesDischarge Planning FinalRose AnnNo ratings yet
- Bipolar Affective Disorder, Current Manic Episode With Symptoms of Psychotic and Care in NursingDocument4 pagesBipolar Affective Disorder, Current Manic Episode With Symptoms of Psychotic and Care in NursingKit LaraNo ratings yet
- Immunity QP New Syllabus (2010-2012)Document40 pagesImmunity QP New Syllabus (2010-2012)Ae Banpong100% (1)
- Caz1 Canagliflozin - DB PDFDocument3 pagesCaz1 Canagliflozin - DB PDFsufaru ciprianNo ratings yet
- Malnutrition Oc-WPS OfficeDocument2 pagesMalnutrition Oc-WPS OfficeLyka MonterealNo ratings yet
- Trauma Complications and TreatmentDocument4 pagesTrauma Complications and TreatmentAnil DasNo ratings yet
- Unit 4Document9 pagesUnit 4luciagarper1No ratings yet
- Session 01.5 Induced Hypothermia-The Nursing CareDocument13 pagesSession 01.5 Induced Hypothermia-The Nursing CaremochkurniawanNo ratings yet
- Referat LP8-2E - CholesterolDocument3 pagesReferat LP8-2E - CholesterolElena DalcaranNo ratings yet
- Liver Disease: Causes and ComplicationsDocument19 pagesLiver Disease: Causes and ComplicationsAleah JayaganNo ratings yet
- Rhinitis AlergiDocument35 pagesRhinitis AlergiRandy GipsonNo ratings yet
- Bile Production - Constituents - TeachMePhysiologyDocument2 pagesBile Production - Constituents - TeachMePhysiologynotesom44No ratings yet
- Complications of Spinal Anesthesia For Scheduled Surgery Experience of The Military Hospital Moulay Ismail MeknesDocument6 pagesComplications of Spinal Anesthesia For Scheduled Surgery Experience of The Military Hospital Moulay Ismail MeknesIJAR JOURNALNo ratings yet
- Scoliosis PPT B IngDocument11 pagesScoliosis PPT B IngSyifa Anindya100% (1)
- Meslekiing 4 FullvizeDocument91 pagesMeslekiing 4 FullvizeÇiğdem BozoğluNo ratings yet
- Batangas Communicable Dse Post Test SCDocument2 pagesBatangas Communicable Dse Post Test SCcianm1143No ratings yet
- Anemias RBC Morphology Approach To DiagnosisDocument24 pagesAnemias RBC Morphology Approach To DiagnosisAyessa VillacorteNo ratings yet
- Emergency Chapter 70Document36 pagesEmergency Chapter 70ShannonNo ratings yet
- Andrea Mae P. Salazar Bsn2Y1-Irr2 Criteria Computation Actual Score JustificationDocument7 pagesAndrea Mae P. Salazar Bsn2Y1-Irr2 Criteria Computation Actual Score Justificationerica mae rasNo ratings yet
- Pengaruh Emotional Freedom Technique (EFT) Terhadap Kecemasan Pada Pasien Chronic Kidney Disease (CKD)Document9 pagesPengaruh Emotional Freedom Technique (EFT) Terhadap Kecemasan Pada Pasien Chronic Kidney Disease (CKD)Utry YaniNo ratings yet
- Modul 1 Bhs - Inggris p3kl - Sem - Genap 2023Document5 pagesModul 1 Bhs - Inggris p3kl - Sem - Genap 2023aqillah a.s.No ratings yet
- White Chodosh Appendix VI HSV FINALDocument5 pagesWhite Chodosh Appendix VI HSV FINALSuzana VoiculescuNo ratings yet
- Clopixol Patient Information Leaflet 2mg 10mg 20mg From Mind OrgDocument9 pagesClopixol Patient Information Leaflet 2mg 10mg 20mg From Mind OrgRevaz SurguladzeNo ratings yet