You might also like
- Fast Facts: Complex Perianal Fistulas in Crohn's Disease: A multidisciplinary approach to a clinical challengeFrom EverandFast Facts: Complex Perianal Fistulas in Crohn's Disease: A multidisciplinary approach to a clinical challengeNo ratings yet
- Hemostatic Balance in Severe Trauma Fped-08-600501Document8 pagesHemostatic Balance in Severe Trauma Fped-08-600501Carolina SartiniNo ratings yet
- Sepsis Therapies: Learning From 30 Years of Failure of Translational Research To Propose New LeadsDocument24 pagesSepsis Therapies: Learning From 30 Years of Failure of Translational Research To Propose New LeadsMark TomNo ratings yet
- Sankar 2019Document8 pagesSankar 2019Janny Torres AvilaNo ratings yet
- 2023-Anxiety Depression and Memory Loss in Chagas Disease - A Puzzle Far Beyond Neuroinflammation To Be Unpicked and SolvedDocument15 pages2023-Anxiety Depression and Memory Loss in Chagas Disease - A Puzzle Far Beyond Neuroinflammation To Be Unpicked and SolvedLagarta CalipsoNo ratings yet
- 10 1016@j Jaad 2019 05 096Document8 pages10 1016@j Jaad 2019 05 096JohnNo ratings yet
- 3 Septicshock SIRS PDFDocument11 pages3 Septicshock SIRS PDFRhobbigfirly UnggulNo ratings yet
- Peds 2020029249Document17 pagesPeds 2020029249nana wardhaniNo ratings yet
- Corticoides Meningitis JamaDocument8 pagesCorticoides Meningitis JamaYohannita AguilarNo ratings yet
- Chronicsubdural Hematoma: Epidemiology and Natural HistoryDocument6 pagesChronicsubdural Hematoma: Epidemiology and Natural HistoryalgoNo ratings yet
- Choque Septico y Falla Multiorgano Relaciona Con Balance de FluidosDocument14 pagesChoque Septico y Falla Multiorgano Relaciona Con Balance de FluidosMiguel Angel Hernandez SerratoNo ratings yet
- Tapia 2019Document9 pagesTapia 2019SANTOSH KUMAR BHASKARNo ratings yet
- (10920684 - Neurosurgical Focus) Predictors of Outcome of Subdural Empyema in ChildrenDocument6 pages(10920684 - Neurosurgical Focus) Predictors of Outcome of Subdural Empyema in ChildrenFatima RamirezNo ratings yet
- Eria 2Document11 pagesEria 2ruth angelinaNo ratings yet
- Risk Factors For Necrotizing Enterocolitis Associated MortalityDocument7 pagesRisk Factors For Necrotizing Enterocolitis Associated MortalityvaleriaNo ratings yet
- Corticoesteroids and Mortality in Children Qith Bacterial Meinigitis PDFDocument9 pagesCorticoesteroids and Mortality in Children Qith Bacterial Meinigitis PDFELISA MORALESNo ratings yet
- Aos 13961Document8 pagesAos 13961Vivian Ayte LopezNo ratings yet
- TrombositopeniaDocument2 pagesTrombositopeniaSoraya RezekiNo ratings yet
- 325 FullDocument20 pages325 FullDessyadoeNo ratings yet
- Guizzetti - 2016Document10 pagesGuizzetti - 2016Bogdan TrandafirNo ratings yet
- Jurnal NeuroDocument6 pagesJurnal NeuroTor JaNo ratings yet
- 1 s2.0 S0140673619329897 MainDocument12 pages1 s2.0 S0140673619329897 MainMaharani Sari NastitiNo ratings yet
- Definiciones PreviasDocument7 pagesDefiniciones PreviasJuan RodriguezNo ratings yet
- Children Less Than 2 With Down Syndrome and SufferDocument1 pageChildren Less Than 2 With Down Syndrome and Sufferhqsfc4gmrnNo ratings yet
- 2010 - Epidemioloy of Ulcerative Keratitis in Northern CaliforniaDocument7 pages2010 - Epidemioloy of Ulcerative Keratitis in Northern CaliforniaPrasetya AnugrahNo ratings yet
- CC 9290Document12 pagesCC 9290elektifppra2022No ratings yet
- Global Hydrocephalus Epidemiology and Incidence: Systematic Review and Meta-AnalysisDocument8 pagesGlobal Hydrocephalus Epidemiology and Incidence: Systematic Review and Meta-AnalysisDhea RizkhythaNo ratings yet
- Spab303 m1 s1 CuetoDocument8 pagesSpab303 m1 s1 CuetoAndrea Alonzo AcevedoNo ratings yet
- Oup Accepted Manuscript 2020Document10 pagesOup Accepted Manuscript 2020Luis Bonino SanchezNo ratings yet
- What 'S New in Musculoskeletal Infection: Guest EditorialDocument8 pagesWhat 'S New in Musculoskeletal Infection: Guest Editorialannida putri maharaniNo ratings yet
- 1 s2.0 S014067362301961X MainDocument16 pages1 s2.0 S014067362301961X MainAnaNo ratings yet
- Actualización en Sepsis y Choque Septico 2023Document23 pagesActualización en Sepsis y Choque Septico 2023Alberto De La VegaNo ratings yet
- Seizures in Adults With Bacterial MeningitisDocument9 pagesSeizures in Adults With Bacterial MeningitiselaNo ratings yet
- Hidrosefalus Pada AnakDocument7 pagesHidrosefalus Pada AnakDintaNo ratings yet
- Ventricular Septal Defect Complicating ST-Elevation Myocardial Infarctions: A Call For ActionDocument12 pagesVentricular Septal Defect Complicating ST-Elevation Myocardial Infarctions: A Call For ActionIde Yudis TiyoNo ratings yet
- Achondroplasia Natural History Study (CLARITY)Document7 pagesAchondroplasia Natural History Study (CLARITY)jakelinelagoadvNo ratings yet
- Ioi80197 463 473Document11 pagesIoi80197 463 473Phạm LinhNo ratings yet
- Hyperoxemia Is Associated With Mortality in Critically Ill ChildrenDocument8 pagesHyperoxemia Is Associated With Mortality in Critically Ill ChildrenNadia SetianingsihNo ratings yet
- Le Cadet 2019Document6 pagesLe Cadet 2019supaidi97No ratings yet
- Incidence and Outcome of Convulsive Status Epilepticus in - 2008 - The Lancet NDocument6 pagesIncidence and Outcome of Convulsive Status Epilepticus in - 2008 - The Lancet NSam NickNo ratings yet
- Clinical Study and Management of Hydrocephalus inDocument5 pagesClinical Study and Management of Hydrocephalus inVirajannatiNo ratings yet
- Piy 008Document4 pagesPiy 008Alejandro GutiérrezNo ratings yet
- Epidemiologia HidrocefaliaDocument24 pagesEpidemiologia Hidrocefaliavane06No ratings yet
- Nguyen Minh Tuan 2013Document8 pagesNguyen Minh Tuan 2013libremdNo ratings yet
- Jurnal Reading DavidDocument14 pagesJurnal Reading DavidAbraham WilliamNo ratings yet
- Patterns of Hydrocephalus Caused by Congenital Toxoplasma Gondii Infection Associate With Parasite GeneticsDocument4 pagesPatterns of Hydrocephalus Caused by Congenital Toxoplasma Gondii Infection Associate With Parasite GeneticsAhmad PradhanaNo ratings yet
- Management of Criticalli Ill Child SepsisDocument4 pagesManagement of Criticalli Ill Child SepsisYanna RizkiaNo ratings yet
- 38 145 1 PBDocument6 pages38 145 1 PBChaya RaghuNo ratings yet
- Caldeira 2018Document6 pagesCaldeira 2018Engels Yeltsin Ponce GonzalesNo ratings yet
- Disparities in Periodontitis Prevalence Among Chronic Kidney Disease PatientsDocument5 pagesDisparities in Periodontitis Prevalence Among Chronic Kidney Disease PatientsKristelle HernandezNo ratings yet
- NEJM - Sickle Cell Disease PDFDocument13 pagesNEJM - Sickle Cell Disease PDFHumberto BritoNo ratings yet
- 793 FullDocument9 pages793 FullDENNYNo ratings yet
- Atencia CarreraDocument23 pagesAtencia Carreraluixch.pNo ratings yet
- A Decade of Management of Subdural Haematoma in Children Aged 2 To 24 Months Hospitalized at The Paediatric Neurosurgery Department of La Timone Children's HospitalDocument8 pagesA Decade of Management of Subdural Haematoma in Children Aged 2 To 24 Months Hospitalized at The Paediatric Neurosurgery Department of La Timone Children's HospitalEditor IJTSRDNo ratings yet
- New England Journal Medicine: The ofDocument11 pagesNew England Journal Medicine: The ofJohn NinNo ratings yet
- Harry 2020Document6 pagesHarry 2020wasiNo ratings yet
- BRCA in Premenopausal Breast CancerDocument8 pagesBRCA in Premenopausal Breast CancerErwin Chiquete, MD, PhDNo ratings yet
- Acido Tranexámico en TCEDocument5 pagesAcido Tranexámico en TCEekavayero88No ratings yet
- Citosinas SepsisDocument9 pagesCitosinas SepsisJosé ChalcoNo ratings yet
- Literature Review On Sickle Cell DiseaseDocument8 pagesLiterature Review On Sickle Cell Diseaseafmzwflmdnxfeb100% (1)
- Asuhan Keperawatan Pada Tn/Ny/Nn/An ... DENGANDocument14 pagesAsuhan Keperawatan Pada Tn/Ny/Nn/An ... DENGANNanda AgustinNo ratings yet
- Pengkajian Gadar Non TraumaDocument14 pagesPengkajian Gadar Non TraumaNanda AgustinNo ratings yet
- FDocument8 pagesFNanda AgustinNo ratings yet
- Effect of Massage Therapy On Duration of Labour: A Randomized Controlled TrialDocument4 pagesEffect of Massage Therapy On Duration of Labour: A Randomized Controlled TrialNanda AgustinNo ratings yet
- Costing of Sea Water RO Plant KPT Manora Design at 100,000 IGPD at 35,000 PPMDocument3 pagesCosting of Sea Water RO Plant KPT Manora Design at 100,000 IGPD at 35,000 PPMMohtashim KazmiNo ratings yet
- CV Fire Catalog PDFDocument112 pagesCV Fire Catalog PDFArul SankaranNo ratings yet
- CARDIOPULMONARY BYPASS - CompressedDocument117 pagesCARDIOPULMONARY BYPASS - CompressedBayan TahaNo ratings yet
- Vdocument - in LRT Design GuidelinesDocument490 pagesVdocument - in LRT Design GuidelinesAlly KhooNo ratings yet
- Submittal - Pipe Clamp - 2019 PDFDocument51 pagesSubmittal - Pipe Clamp - 2019 PDFQaiser MehmoodNo ratings yet
- Moonshot Beer Summary of Rec 2Document4 pagesMoonshot Beer Summary of Rec 2Hassan AhmadNo ratings yet
- Air Bag BleizerDocument88 pagesAir Bag BleizerEnrique Felipe Reveco BahamondesNo ratings yet
- Ryan Ronquillo ComplaintDocument39 pagesRyan Ronquillo ComplaintMichael_Lee_RobertsNo ratings yet
- 2021 CAPEX - THEODORE Chiller Spares v1.3Document6 pages2021 CAPEX - THEODORE Chiller Spares v1.3Paul CansinoNo ratings yet
- 2010 Skema Pat SBPDocument17 pages2010 Skema Pat SBPAfiqah RoshidiNo ratings yet
- Brief Desccription of Ammonia Urea Plants With RevampDocument48 pagesBrief Desccription of Ammonia Urea Plants With RevampGeorge Van BommelNo ratings yet
- Bridge Final ProposalDocument14 pagesBridge Final ProposalDr. A B M Amrul KaishNo ratings yet
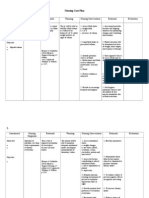
- Nursing Care Plan CKDDocument6 pagesNursing Care Plan CKDReylan Deo Rallo Asio100% (5)
- Sithkop005 AnswersDocument46 pagesSithkop005 AnswersSid SharmaNo ratings yet
- 7.6.2. Poly-Silicon Gate TechnologyDocument14 pages7.6.2. Poly-Silicon Gate TechnologyHarshad KulkarniNo ratings yet
- ENGR 260 - Circuits and Devices: COURSE SYLLABUS - Spring 2015Document4 pagesENGR 260 - Circuits and Devices: COURSE SYLLABUS - Spring 2015saintNo ratings yet
- Honey Python TestingDocument2 pagesHoney Python Testinger.honeyraj2016No ratings yet
- Layer 3 48-Port 10G SFP+ + 2-Port 40G QSFP+ + 4-Port 100G QSFP28 Managed SwitchDocument10 pagesLayer 3 48-Port 10G SFP+ + 2-Port 40G QSFP+ + 4-Port 100G QSFP28 Managed Switchbader eddine khezamiNo ratings yet
- Determination of Trace Element Contents of Baby Foods From TurkeyDocument6 pagesDetermination of Trace Element Contents of Baby Foods From TurkeyYel LieNo ratings yet
- Divisional Chart-IIDocument1 pageDivisional Chart-IIabhisek19870% (1)
- Sp3510 User ManualDocument48 pagesSp3510 User Manualchristos1157No ratings yet
- Learning Guide-34: Participate in Rehabilitationand Restoration of Degraded AreasDocument50 pagesLearning Guide-34: Participate in Rehabilitationand Restoration of Degraded AreasRafez JoneNo ratings yet
- Astm C 22C 22MDocument2 pagesAstm C 22C 22MProfessor Dr. Nabeel Al-Bayati-Consultant EngineerNo ratings yet
- Kratos Pitch Deck PresentationDocument14 pagesKratos Pitch Deck PresentationCS-B Dhanya Lakshmi GNo ratings yet
- 2 Megabit (256 K X 8-Bit) CMOS EPROM: Distinctive CharacteristicsDocument12 pages2 Megabit (256 K X 8-Bit) CMOS EPROM: Distinctive CharacteristicsVictor TruccoNo ratings yet
- The Space RaceDocument15 pagesThe Space RaceRadu Petrusan100% (1)
- Prioritization Open CholicestectomyDocument2 pagesPrioritization Open CholicestectomyCleo Joyce CristalNo ratings yet
- Parul University: Faculty of Engineering and TechnologyDocument5 pagesParul University: Faculty of Engineering and TechnologySudhanshu SinghNo ratings yet
- HUAWEI CUN U29-Bitel Phone Upgrade Guide - V1.1 - 20161128Document10 pagesHUAWEI CUN U29-Bitel Phone Upgrade Guide - V1.1 - 20161128Danny J GonzalezNo ratings yet
- The 8051 Microcontroller and Embedded Systems: Motor Control: Relay, PWM, DC and Stepper MotorsDocument51 pagesThe 8051 Microcontroller and Embedded Systems: Motor Control: Relay, PWM, DC and Stepper MotorsAmAnDeepSingh100% (1)