You might also like
- Medical Nutrition Therapy A Case Study Approach 5th Edition Nelms Solutions Manual DownloadDocument7 pagesMedical Nutrition Therapy A Case Study Approach 5th Edition Nelms Solutions Manual DownloadSteven Dubose100% (24)
- Sodium Chloride Injection and Intravenous Infusion-PiDocument4 pagesSodium Chloride Injection and Intravenous Infusion-PiNg Chee LunNo ratings yet
- CFR Pulm HTN HFDocument7 pagesCFR Pulm HTN HFAnonymous oQtve4oNo ratings yet
- Hemodynamic Indices in Pulmonary Hypertension: A Narrative ReviewDocument15 pagesHemodynamic Indices in Pulmonary Hypertension: A Narrative ReviewfabiolaNo ratings yet
- Hipertensión Pulmonar Por Enfermedad VálvulasDocument10 pagesHipertensión Pulmonar Por Enfermedad Válvulasluiserikolivares1390No ratings yet
- Acute Respiratory Distress Syndrome (ARDS) - Associated Acute Cor Pulmonale and Patent Foramen Ovale: A Multicenter Noninvasive Hemodynamic StudyDocument6 pagesAcute Respiratory Distress Syndrome (ARDS) - Associated Acute Cor Pulmonale and Patent Foramen Ovale: A Multicenter Noninvasive Hemodynamic StudyminiypuntoNo ratings yet
- Research Article: ECG Markers of Hemodynamic Improvement in Patients With Pulmonary HypertensionDocument11 pagesResearch Article: ECG Markers of Hemodynamic Improvement in Patients With Pulmonary HypertensionFaradilla NovaNo ratings yet
- Jvs 17 243Document10 pagesJvs 17 243Dr.Lázár AttilaNo ratings yet
- Editorial Bob y JesúsDocument2 pagesEditorial Bob y JesúsEmiliano GogniatNo ratings yet
- ChestDocument6 pagesChestRuben EkspayerNo ratings yet
- Pulmonary HTN. ESC POCKET GLS 2022. Larger Font. For PrintingDocument79 pagesPulmonary HTN. ESC POCKET GLS 2022. Larger Font. For PrintingGeoNo ratings yet
- Dębska-Kozłowska2021 Article WhereAreWeIn2021WithHeartFailuDocument12 pagesDębska-Kozłowska2021 Article WhereAreWeIn2021WithHeartFailuSyifa Mahmud Syukran AkbarNo ratings yet
- Clinical Outcome of Closure of A Small Atrial Septal Defect in A Patient With Pulmonary Arterial HypertensionDocument5 pagesClinical Outcome of Closure of A Small Atrial Septal Defect in A Patient With Pulmonary Arterial HypertensionFaradiba MaricarNo ratings yet
- Respiratory and Pulmonary Medicine: ClinmedDocument5 pagesRespiratory and Pulmonary Medicine: ClinmedxxxvrgntNo ratings yet
- Hipertensi PulmonalDocument5 pagesHipertensi PulmonalSteven RichardNo ratings yet
- Bedside Hemodynamic MonitoringDocument26 pagesBedside Hemodynamic MonitoringBrad F LeeNo ratings yet
- Scape Vs FospeDocument5 pagesScape Vs FospeDr. FarhanNo ratings yet
- HT - Meyer Philippe Heart and LungsDocument37 pagesHT - Meyer Philippe Heart and LungsKristin AndrewsNo ratings yet
- 由左心性疾病引起的肺动脉高压Document17 pages由左心性疾病引起的肺动脉高压Xin HuangNo ratings yet
- 1 s2.0 S1053077023009060 MainDocument31 pages1 s2.0 S1053077023009060 MainedwardmenesesNo ratings yet
- Pathophysiology of COPDDocument4 pagesPathophysiology of COPDrinieeeNo ratings yet
- Vieillard-Baron2018 Article DiagnosticWorkupEtiologiesAndMDocument17 pagesVieillard-Baron2018 Article DiagnosticWorkupEtiologiesAndMFranciscoNo ratings yet
- Diagnostic and Therapeutic Challenges in Patients With Coexistent Chronic Obstructive Pulmonary Disease and Chronic Heart FailureDocument10 pagesDiagnostic and Therapeutic Challenges in Patients With Coexistent Chronic Obstructive Pulmonary Disease and Chronic Heart FailureLucy Naomi BesitimurNo ratings yet
- 2022 PH Guidelines - Essential MessagesDocument10 pages2022 PH Guidelines - Essential MessagesRoyNo ratings yet
- VCV Vs PCV in ArdsDocument7 pagesVCV Vs PCV in Ardspaddy9980No ratings yet
- Severe Pulmonary Arterial Hypertension - Stratification of Medical Therapies, Mechanical Support, and Lung TransplantationDocument11 pagesSevere Pulmonary Arterial Hypertension - Stratification of Medical Therapies, Mechanical Support, and Lung Transplantationjose lopeNo ratings yet
- 1 s2.0 S1053077021005723 PDFDocument13 pages1 s2.0 S1053077021005723 PDFangelicaNo ratings yet
- Prevalence of Pulmonary Hypertension in COPD: Original Research ArticleDocument5 pagesPrevalence of Pulmonary Hypertension in COPD: Original Research ArticleMuhamad AgungNo ratings yet
- Journal ReadingDocument17 pagesJournal ReadingRhyka AchmadNo ratings yet
- Retrospective Study PAHDocument4 pagesRetrospective Study PAHAfifah Nur KartikasariNo ratings yet
- Imaging of Pulmonary Hypertension - Pictorial Essay - ScienceDirectDocument37 pagesImaging of Pulmonary Hypertension - Pictorial Essay - ScienceDirectmohammedNo ratings yet
- Diastolic Blood PressureDocument7 pagesDiastolic Blood PressureElena MadalinaNo ratings yet
- Chronic Management of Hypertension After Stroke: The Role of Ambulatory Blood Pressure MonitoringDocument7 pagesChronic Management of Hypertension After Stroke: The Role of Ambulatory Blood Pressure MonitoringHalbar August KandaNo ratings yet
- Hypertension HypotensionDocument6 pagesHypertension HypotensionAlpascaFirdausNo ratings yet
- Assessment of Operability of Patients With Pulmonary Arterial Hypertension Associated With Congenital Heart DiseaseDocument8 pagesAssessment of Operability of Patients With Pulmonary Arterial Hypertension Associated With Congenital Heart DiseaseWulan AviantoroNo ratings yet
- Falla Cardiaca Con Fraccion de Eyeccion ConservadaDocument44 pagesFalla Cardiaca Con Fraccion de Eyeccion ConservadaDiego Andrés Mejía VascoNo ratings yet
- Exercise HTP ArtDocument10 pagesExercise HTP ArtDiana CarstairsNo ratings yet
- RHC Best Practice - FullDocument11 pagesRHC Best Practice - FullAlessioNavarraNo ratings yet
- FCVM 09 876755Document8 pagesFCVM 09 876755Faradiba MaricarNo ratings yet
- HTAP La VarstniciDocument16 pagesHTAP La VarstnicidanradulescuNo ratings yet
- 449 FullDocument6 pages449 Fullwael aboelmagdNo ratings yet
- VPP y Vvci en Sepsis-2016Document20 pagesVPP y Vvci en Sepsis-2016Elsa AivarNo ratings yet
- Tusman 2018Document10 pagesTusman 2018Karel ZertucheNo ratings yet
- 36814803Document5 pages36814803Fernando CardiologíaNo ratings yet
- 1 s2.0 S0002914922005355 MainDocument11 pages1 s2.0 S0002914922005355 MainRamona GhengheaNo ratings yet
- Pulmonary Arterial Hypertension: The Burden of Disease and Impact On Quality of LifeDocument9 pagesPulmonary Arterial Hypertension: The Burden of Disease and Impact On Quality of LifeMeilani Azaria SNo ratings yet
- 1 s2.0 S1936878X14010122 MainDocument17 pages1 s2.0 S1936878X14010122 MainAnonymous oQtve4oNo ratings yet
- J JCHF 2018 04 005Document9 pagesJ JCHF 2018 04 005Frederico PóvoaNo ratings yet
- Medical Therapy For Eisenmenger Syndrome: A Case Report and Review of LiteratureDocument9 pagesMedical Therapy For Eisenmenger Syndrome: A Case Report and Review of LiteratureANISA RIFKA RIDHONo ratings yet
- Guideline USA 2020Document16 pagesGuideline USA 2020Rodrigo Felipe Albuquerque Paiva de OliveiraNo ratings yet
- Prognostic Factors in Pulmonary Arterial Hypertension: Literature ReviewDocument5 pagesPrognostic Factors in Pulmonary Arterial Hypertension: Literature Reviewhuda riyambodoNo ratings yet
- Category 1) Pulmonary Hypertension Diagnosis and Treatment of Secondary (NonDocument11 pagesCategory 1) Pulmonary Hypertension Diagnosis and Treatment of Secondary (NonAmit GoelNo ratings yet
- Pulmonary Hypertension in Cardiac SurgeryDocument14 pagesPulmonary Hypertension in Cardiac SurgeryinaNo ratings yet
- Ijcm 2014012415343834 PDFDocument5 pagesIjcm 2014012415343834 PDFangela_karenina_1No ratings yet
- Robert C. Bourge, M.D., PH.D.: Director Division of Cardiovascular Disease University of AlabamaDocument48 pagesRobert C. Bourge, M.D., PH.D.: Director Division of Cardiovascular Disease University of AlabamaUtomo FemtomNo ratings yet
- Cardiopulmonary Exercise Testing - BahasaInggrisDocument10 pagesCardiopulmonary Exercise Testing - BahasaInggrisOktaviani Putri FatimahNo ratings yet
- Pulmonary Hypertension in Children - Classification, Evaluation, and Diagnosis - UpToDateDocument37 pagesPulmonary Hypertension in Children - Classification, Evaluation, and Diagnosis - UpToDateMaria Fernanda LauraNo ratings yet
- 1 s2.0 S0870255121005096 MainDocument3 pages1 s2.0 S0870255121005096 MainangelemanuelarmasNo ratings yet
- Tratamiento Icc FevpDocument17 pagesTratamiento Icc FevpGuissela Montoya LopezNo ratings yet
- PletismografiaDocument10 pagesPletismografiamaxifamous6No ratings yet
- SCUBE1 Controls BMPR2-Relevant Pulmonary Endothelial FunctionDocument20 pagesSCUBE1 Controls BMPR2-Relevant Pulmonary Endothelial FunctionLeidy LambertinezNo ratings yet
- Drug StudyDocument3 pagesDrug StudyStephannie MirandaNo ratings yet
- Body Systems Portfolio - Tommy JDocument8 pagesBody Systems Portfolio - Tommy Japi-554072790No ratings yet
- Early Complications of MIDocument11 pagesEarly Complications of MIjen262004No ratings yet
- U.S. Army Survival Manual FM 21-76 (June 1992)Document572 pagesU.S. Army Survival Manual FM 21-76 (June 1992)explorer_ebook100% (1)
- CRT Exam Review Guide Chapter 8Document10 pagesCRT Exam Review Guide Chapter 8Dharlyn MungcalNo ratings yet
- Arterial Tourniquets Anaesthesia Tutorial of The Week 200 11 OCTOBER 2010Document7 pagesArterial Tourniquets Anaesthesia Tutorial of The Week 200 11 OCTOBER 2010tessalaiNo ratings yet
- Uropati ObstruktifDocument22 pagesUropati ObstruktifEvan Permana100% (1)
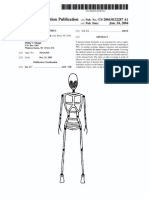
- Patente Endoesqueleto para Sex Doll SiliconaDocument12 pagesPatente Endoesqueleto para Sex Doll SiliconaGabriel De Jesus100% (1)
- Bowel Nosodes Power PointDocument15 pagesBowel Nosodes Power PointTheresa Dale83% (6)
- Endocrine and Metabolic Disorders PDFDocument31 pagesEndocrine and Metabolic Disorders PDFAna-Maria50% (2)
- Lecture Notes On Biophysics and Bioimaging 2009Document128 pagesLecture Notes On Biophysics and Bioimaging 2009Anonymous 9rJe2lOskx100% (2)
- 1.4 Selecton of Blood BagDocument3 pages1.4 Selecton of Blood BagBALAJINo ratings yet
- Department of Pathology: Mrs. Malyala SujathaDocument6 pagesDepartment of Pathology: Mrs. Malyala Sujathasanath kumarNo ratings yet
- Mitosis Vs MeiosisDocument40 pagesMitosis Vs Meiosiscmillica1176No ratings yet
- Imbalanced Nutrition Less Than Body Requirements Diabetes NCP PDFDocument5 pagesImbalanced Nutrition Less Than Body Requirements Diabetes NCP PDFashamy acolNo ratings yet
- Inhaled Anesthesia For BirdsDocument18 pagesInhaled Anesthesia For BirdsBianca PaludetoNo ratings yet
- Technique Used For Study of Bio Synthetic PathwayDocument9 pagesTechnique Used For Study of Bio Synthetic Pathwayshankul kumar95% (19)
- Cancer Case StudyDocument15 pagesCancer Case StudyRobin HaliliNo ratings yet
- Urine Concentration and Dilution Regulation of Extracellular Fluid Osmolarity and Sodium ConcentrationDocument21 pagesUrine Concentration and Dilution Regulation of Extracellular Fluid Osmolarity and Sodium ConcentrationMelissa VillanuevaNo ratings yet
- Lecture 1 Anatomy of Prokarotic Genome 31 Jan 2012Document29 pagesLecture 1 Anatomy of Prokarotic Genome 31 Jan 2012Paramvir MannNo ratings yet
- Women's Health MagazineDocument140 pagesWomen's Health MagazineAgiimaa0% (1)
- Problem Set 2 EndocrinologyDocument12 pagesProblem Set 2 EndocrinologyJessica EtieneNo ratings yet
- Anemia and AnesthesiaDocument11 pagesAnemia and AnesthesialhalamNo ratings yet
- Physrev 00038 2020Document108 pagesPhysrev 00038 2020gaza aidanNo ratings yet
- Molecular and Cell Biology of CementumDocument26 pagesMolecular and Cell Biology of CementumSaul TorresNo ratings yet
- 11 Ch1208 5127 PDFDocument25 pages11 Ch1208 5127 PDFThamarai ElanthirayanNo ratings yet
- Integumentary System - NUR1019 - 20sept2022Document33 pagesIntegumentary System - NUR1019 - 20sept2022琪琪No ratings yet
- Boiler Attendant RulesDocument23 pagesBoiler Attendant RulesAli Azam KhanNo ratings yet