Professional Documents
Culture Documents
Rapp 1989
Rapp 1989
Uploaded by
asdasdasdCopyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Rapp 1989
Rapp 1989
Uploaded by
asdasdasdCopyright:
Available Formats
PATIENT-CONTROLLED ANALGESIA:
A REVIEW OF EFFECTIVENESS OF THERAPY AND
AN EVALUATION OF CURRENTLY AVAILABLE DEVICES
Robert P. Rapp, Brack A. Bivins, Robert A. Littrell, and Thomas S. Foster
ABSTRACf: Patient-controlled analgesia (PCA) is a major advance in this article is to review the data in support of the effective-
the management of pain in postoperative and cancer patients. The ness of PCA and to evaluate the currently available PCA
success of PCA has resulted in a proliferation of marketed devices to
devices.
administer small bolus doses of parenteral pain-control drugs at fixed
intervalscontrolled by the patient with the push of a button. Because
patientsdemonstrate marked individual variation in pain medication Pain and Traditional Narcaic Administration
requirements, PCA devices should be able to accommodate rapidly The principal impetus for the development of PCA has
changing requirementsfor drugs with a minimum amount of effort on
behalf of health care personnel. Crude electronicdevices were
been the failure of traditional techniques, primarily the pro
developedin the late 1960sand the early 1970sand usually consisted intramuscular administraton of narcotic analgesics, to ade-
of a syringe pump connected to some sort of timing device. Most quately manage pain. The effective management of pain
modem PCA devices marketed in the past five years are much more has long been a major clinical challenge despite the avail-
sophisticated devices that are microprocessorbased and some newer ability and use of potent narcotic analgesics. Patients dem-
devices even generate hard copy for a permanent record of drug onstrate marked variability in analgesic requirements,
administration. Although many such devices are available(includinga
totallydisposable PCA device), few have undergone extensiveclinical
dosing intervals, and tolerance to adverse effects. In the
evaluation. A review of the literature shows many devices are acute setting, traditional pro intramuscular narcotics have
available for use without a single publicationto document the safety been inappropriately dosed a large proportion of the
and utility of the device in the routine patient care situation. Use of time.r" Marks and Sachar found that 73 percent of inpa-
the PCA method of pain control will grow, and all hospital-based tients receiving an average of 90 mg/d of im meperidine had
healthcare personnel should become familiar with their use and severe or moderate distress." Similarly, Cohen found 75
limitations. percent of postoperative patients treated with standard im
D1CP 1989;23:899-904. narcotics to be in marked or moderate distress. 5 Such stud-
ies also have found that with traditional pro medication
administration techniques patients are often underdosed at
PATIENT-CONTROLLED ANALGESIA (PCA) is recognized as a times of peak pain and overdosed to sedation when pain is
major advance in the management of pain for a wide variety less severe. 3-5
of clinical problems. I PCA employs an infusion pump inte- Many factors contribute to the inadequacy of postopera-
grated with a timing device that allows patients to self- tive analgesia. The treatment of postoperative pain has
administer small doses of narcotics intravenously. Using a most frequently used an every four to six hour schedule of
PCA device, a patient may self-administer an analgesic im medications given at the discretion of the nursing staff
when pain is perceived and experience a virtually immedi- on a pro basis.v' This process involves the pain cycle
ate analgesic effect. The dose and frequency for the anal- (Figure I) as described by Graves et al." and includes
gesic are controlled to prescribed limits by the settings of problems such as: (I) the potential for significant delays
the device. In a large number of clinical studies, PCA has between the perception of pain and the administration of
been shown to be a safe, effective, and economical means pain medication, (2) the high variability in absorption with
of managing pain. 2 im analgesics and a narrow effective range of serum levels,
As the concept of PCA has been validated, there has (3) the minimum serum concentration of drug to achieve
been a proliferaton of marketed devices. The data in sup- analgesia is exceeded for only 35 percent of the dosing
port of these devices are highly variable. The purpose of interval, and (4) peak concentrations of analgesic may vary
as much as fivefold in patients given the same im doses at
ROBERT P. RAPP, !'harm.D., is a Professor and the Chairman, Divisionof Pharmacy the same dosing interval.
Practice and Science, College of Pharmacy, University of Kentucky, Lexington, KY
40536:BRACK A. BIVINS, M.D.• is the Director. Divisionof Traumaand Emergency
Research has emphasized the importance of pain man-
Surgery. Henry Ford Medical Center, Detroit. MI; ROBERT A. LITTRELL, agement." For example, the fear of pain may lead to
!'harm.D.• isa PainManagementPharmacist,University Hospital,Departmentof Phar- delays in seeking care. In the postoperative period inade-
macy Central Supply, Lexington. KY; and 11I0MAS S. FOSTER, !'harm.D., is a
Imfessor and the Director, Caller for Pharmaceutical Science and ThchnoIogy. CoUege of
quately controlled pain may lead to decreased ambulation
Pharmacy. University of Kentucky, Lexington, KY.ReprInts: RobertP. Rapp,!'harm.D. and poor pulmonary toilet. Other problems with pain man-
DICP, The AnnaLs of Pharmacotherapy • 1989November, VoLume 23 • 899
Downloaded from aop.sagepub.com at The University of Iowa Libraries on June 9, 2015
agement center on the attitudes of medical personnel. The ~ patient has pain
antiquated notion that to suffer pain is in some way benefi-
sedation
~
call nurse
cial should not be part of any medical or nursing plan in the
1980s. Similarly, the fear of narcotic addiction, proven to
be unfounded in the management of acute pain, should not
govern analgesic regimens. Angell stated that "in no other
relief of pain
r \
nurse responds
area of medicine has such an extravagant concern for side
effects so drastically limited treatment. "10 In modern clini-
f
absorption from site
l
nurse screens
J
"
cal practice the adequate control of pain should be a goal
achieved through communication and cooperation among injection given sign out medication
all health professionals. 11
The PeA Concept prepare injection
Given the problems associated with traditional im nar- Figure I. Conventional pain therapy cycle.
cotic administration, a system such as PCA, which allows
for individual variation in analgesic requirements, should
be accepted by both medical personnel and patients. The
concept of small, bolus doses of narcotics as an analgesic especially for patients with terminal cancer pain that require
technique has been present for over 25 years. In 1963 Roe increasing doses of analgesics. 19,20
demonstrated that small iv doses of analgesics gave more
effective pain relief than im doses. Unfortunately, the man-
Therapeutic EjJicQ£Y
ually administered iv bolus system had several negative In a prospective, randomized trial, Bennett et al. com-
aspects, including a very short duration of pain relief with pared PCA morphine sulfate with morphine sulfate 8-12
small doses and an unacceptably high incidence of seda- mg im q4-6h prn. Patients in the PCA group maintained a
tion, respiratory depression, nausea, and vomiting with state of adequate analgesia without sedation compared with
higher doses." Using a manual administration system the im group, who exhibited more sedation between 6 a.m.
monitored by a "nurse observer," Sechzer noted in 1968 and 10 p.m. The PCA group showed greater sedation dur-
that small doses of iv analgesics were effective. However, ing regular sleeping hours. Patients and nursing staff were
he also found that patient variations in dose requirements more satisfied with PCA-administered morphine. Only in
were cyclic and inconsistent. 13 Even if these early systems the PCA group were patients able to meet the wide varia-
had been completely acceptable clinically, the nursing time tion seen in the amount of morphine required." Numerous
required by the manual infusion techniques would be pro- studies have verified the high level of patient satisfaction
hibitive in today's financially controlled hospital environ- seen in PCA-administered analgesics.P-" A comparative
ment and would be further limited by the nursing shortage trial of nursing-controlled continuous infusion morphine
affecting most areas of the U.S. (i.e., the nurse increased the infusion rate when the patient
The early studies of intermittent bolus dosing of anal- complained of pain and decreased the rate when the patient
gesics hinted at the potential of PCA. The rapid progress in seemed to be sedated) versus regularly scheduled im mor-
microprocessor electronics in hospital infusion control phine given q4h demonstrated an improvement in postop-
equipment of the 1970s allowed the medical electronics erative pulmonary function in the continuous infusion
industry to design specific devices for administration of group." Other investigators have shown better pulmo-
small iv doses of analgesics. With these devices incorporat- nary function in patients using PCA compared with stan-
ing safeguards against overinfusion, excess sedation, and dard im prn regimens." Two studies have shown that, in
respiratory depression, analgesic administration could be spite of better analgesia in the patients receiving PCA, the
controlled in most cases by the patient. 14 total dose of morphine required is less than that in patients
The first electronic PCA devices were developed in the receiving im drugs. 27 ,28 Other studies, however, have not
late 1960s and early 1970s. These devices were rather crude demonstrated similar findings but still find a high level of
by today's standards and consisted of a syringe pump con- patient satisfaction when PCA is used. 24,29 Graves et al.
nected to a timing device. The patient activated the syringe demonstrated a diurnal morphine dosing rhythm in mor-
pump by depressing a hand-held button connected to a bidly obese patients undergoing gastric bypass. Peak mor-
timing and lockout device.9.1s-18 phine use occurred at 9 a.m. and was lowest at 3 p.m. This
Today, there are a number of electronic PCA devices on difference was statistically significant and was postulated to
the market as well as a recently introduced nonelectronic be related to the diurnal variation in adrenocorticotropic
device that uses manually applied power rather than electri- hormone and pituitary secretion of beta-endorphins. Adap-
cal line power to deliver the bolus of medication. Table I tation of drug dosing to drug diurnal requirements could be
lists the major characteristics of PCA devices presently accomplished only with the PCA system of administra-
available in the U.S. Many of these devices have additional tion."
capability including the administration of bolus loading The risk of clinically significant adverse effects associ-
dose, the infusion of a baseline dose of drug together with a ated with PCA appears to be quite low. Initial fears of
demand bolus dose, storage of patient data for various time respiratory depression with commonly used doses of ago-
periods, and the generation of hard copy of patient data for nist narcotic analgesics have been shown to be unfounded.
nursing records in addition to small prn bolus doses." Patients undergoing many different types of major surgery
There also are a number of research/clinical projects that have had consistently normal arterial blood gases with
have evaluated the use of home PCA devices designed PCA use in the postoperative period.t'-" Respiratory
900 • DICP, The Annals of Pharmacotherapy • 1989 November, Volume 23
Downloaded from aop.sagepub.com at The University of Iowa Libraries on June 9, 2015
Patient-Controlled Analgesia
mechanics have also been shown to remain normal in clini- tion programs and by insuring that personnel follow written
cal trials with PCA.33.34 hospital procedures in all phases of set up. One report of a
PCA also may offer some advantages in terms of com- patient's death from what may have been a pump malfunc-
plications of narcotic adverse effects." Narcotics can pro- tion has been published." The patient's family and
duce a variety of adverse effects including nausea, friends must be instructed not to "push the button" for the
sedation, respiratory depression, and pruritus. Narcotic patient. In our experience, family interference (albeit well
addiction and/or withdrawal in patients being treated for intentioned) with the pain control cycle has resulted in
acute pain develops rarely and does not appear to be a additional narcotic administration to a comfortable or
clinically significant problem. sleeping patient. This may obviously cause adverse effects
One narcotic adverse effect that appears to be related to with PCA therapy. Routine cleaning and sound mainte-
administration technique is pruritus, which is particularly nance of the PCA control device are necessary to ensure
bothersome in patients receiving epidural narcotics. In a that mechanical malfunctions are minimal as with any
randomized trial comparing epidural PCA and im mor- patient care microprocessor-based equipment. Since PCA
phine, Eisenach et al. found that 85 percent of patients systems usually are connected to a peripheral catheter,
treated with epidural morphine complained of pruritus and problems associated with the catheter will influence the
40 percent required treatment with systemic medications success of pain management. The outpatient use of PCA by
for relief of symptoms. Pruritus was significantly less in the subcutaneous route has been reported; this would over-
both the PCA and im morphine groups.v Another com- come the problems associated with maintaining an indwell-
parative trial has shown similar results. 37 ing venous catheter. 40
The main concerns with patient safety with PCA appear
PeA Devices
to be associated with operator error." White reported two
cases in which overdoses of PCA-administered narcotics Many PCA devices are now commercially available and
occurred. The first case involved a programming error and use a variety of different technologies to store and adminis-
the second involved the inadvertent administration of a ter small bolus doses of the drug. Most devices use a
bolus dose of sufentaniI. 38 Errors of this type are best syringe system with a "screw driven" motor to depress the
avoided by conducting rigorous nursing inservice educa- plunger of the syringe. The motor is interfaced with the
Table 1. Characteristics of PCA Devices Available in the U.S.
LOCKOUT
PREALLED SECURITY INTERVAL
DEVICE NAME FUNCTIONS BOLUS SYRINGE SYSTEM RANGE
Abbott Lifecare PeA volume yes; key 5-99 min
Infusor 1821 30 mL
Abbott Lifecare PeNcontinuous mg yes; key 5-99 min
Infusor 4100 PeNcontinuous 30 mL
Bard PeA mg or no; yes 3-240 min
Ambulatory continuous volume 100 or
PeA PeNcontinuous 250 mL
reservoir
Baxter PeA PeA fixed use with optional 6 min
System* volume Baxter pole fixed
Infusor; mount
not prefilled
Becton Dickinson PeA mg yes; key 5-99 min
PeA Infusor continuous IMS prefilled
PeNcontinuous 30 mL
Graseby PeA PeA mg no; key 3-40 min
System continuous B.D. disp
PeNcontinuous 60 mL
Harvard PeA PeNcontinuous volume yes; key 3-60 min
Pump 6464-00 I PeNcontinuous 50 mL
MiniMedPeA PeA volume no; case 0-799 min
Device-404-S continuous 3 mLdisp locks
PeNcontinuous syringe
Pancretec PeA mg or no; key I min-
Provider-5ooo continuous volume use with 50- 200 h
PeNcontinuous 3000 mL iv
bag
Pharmacia PeA mg no; key 5-199 min
Deltec-Model continuous use with
5200 PXC PeNcontinuous medication
cassette
Stratofuse PeA volume yes; key 5-60 min
PeA PSM-9000 continuous IMS prefilled
PeNcontinuous 30 mL
*Includes Baxter Infusor (5 mUh) and patient-control module.
DICP, The Annals of Pharmacotherapy •
Downloaded from aop.sagepub.com at The University of Iowa Libraries on June 9, 2015
1989 November, Volume 23 • 901
microprocessor for programming and for safety alarms. syringes but offers the continuous infusion mode or the
Pumps manufactured by Abbott, Bard, Becton Dickinson, continuous infusion plus bolus dose mode of operation in
Graseby, Strato, and MiniMed use this technology. Other addition to the standard PCA mode. The unit is pro-
devices connect directly to standard iv plastic containers grammed in milligrams and concentration is entered in
(Pancretec) or use disposable cassettes (Pharmacia, Deltec mg/mL instead of volume, a feature throught to be desir-
BARD Ambulatory). Baxter markets a disposable PCA able by the Health Devices group." An additional feature
mechanical device known as the patient-control module, of the new Abbott device includes computer-prompted pro-
which must be used with the Baxter Infusor, a 50-mL gramming and a system that double-checks the dose and
elastomer balloon enclosed in a rigid frame. The safety and infusion rate. This new unit will probably replace the older
utility of each marketed device should be verified through Abbott device over the next several years.
appropriate clinical trials and by vigorous in vitro evalua-
tion such as conducted by the nonprofit agency, the Emer- BARD HARVARD PeA INFUSOR
gency Care Research Institute (ECRI). A recent issue of This unit uses either standard 60-mL disposable syringes
Health Devices. published by ECRI, evaluates the available or 50-mL prefilled glass syringes. The syringe is placed in
PCA devices in the U.S.14 This report is an extremely a slot secured by a locked plastic cover. All programming is
valuable reference for hospitals interested in beginning a done in volumetric units, and all three modes of operation
PCA program. can be selected (i.e., PCA, PCA/continuous, or continuous
Clinical Documentation ofPCA Devices infusion only). Owen et al. conducted a laboratory and
clinical comparison of the Bard PCA Infusor and the On
ABBOTI' LABORATORIES LIFECARE PeA INFUSOR Demand Analgesia Computer (ODAC-Janssen Scientific).
The Abbott PCA Infusor was one of the first micro- Both devices performed satisfactorily in the comparative
processor-based infusion control devices to gain clinical trial. 46
acceptance in the U.S. and has the largest published clinical Wermeling et al. used the Bard Instrument in 25
use experience. This device is preset on physicians' orders postoperative patients, the majority of whom underwent
for dose volume (volume per patient-activated infusion in total abdominal hysterectomy. Pain control was managed
milliliters) and lockout interval (minutes between doses). with butorphanol. The device performed in a satisfactory
Any combination that totals more than 20 mLth is not manner in all 25 patients, but 4 had insufficient pain relief
allowed. The dose and lockout setting are displayed on the with butorphanol and were switched to PCA morphine."
face of the device. An alarm sounds if an attempt is made to From an administrative and drug-control standpoint, the
tamper with the cover that locks and secures the controls, use of drugs such as butorphanol, which do not fall under
the analgesic vial, or the drive mechanism. A visual display the Drug Enforcement Administration Schedule II cate-
indicates the total volume delivered since last cleared and gory, is desirable. Paperwork by nursing and pharmacy
set. Touch switches activate display of the number of com- personnel would be reduced, as would the theoretical pos-
pleted patient dose requests and the maximum preset four- sibility of illegal drug diversion. However, the utility of
hour volume. The device can be operated on battery power agonist/antagonist drugs in relieving the most serious
or AC current. To initiate an infusion, the patient activates a postoperative pain remains to be proven by future compara-
hand-held button similar to a standard nurse call button. tive trials with PCA morphine sulfate. An additional case
This device uses a dedicated glass syringe that can be study using the Bard PCA Infusor to give PCA high-dose
purchased prefilled or empty. The cartridge or syringe of morphine to a burn patient has been published."
drug and all switches are located behind a panel door that
locks. The lock also prevents removal of the unit from the iv BAXTER PeA INFUSOR WITH PATIENT-CONTROL MODULE
pole. Clinical documentation of the use and safety of the The Baxter unit consists of two separate entities that
Abbott device has been fairly extensive. must be used together to perform PCA. The infusor is an
Citron et al. used the Abbott device in patients with elastomer balloon device that is breech-filled with up to 50
severe pain from terminal cancer. At the completion of the mL of the narcotic solution (usually morphine sulfate 2
study, all eight patients expressed satisfaction with the unit mg/mL). The 5 mLth infusor delivers 0.5 mL every six
and five patients preferred the PCA mode of therapy over minutes. Constant mechanical pressure is generated by the
conventional narcotic therapy." Harrison et al. used the elastomer balloon and an outflow restrictor. The set from
Abbott PCA device in a comparative trial of PCA, epi- the infusor is connected to the patient control module
dural, and im morphine. Pain relief was superior in the (PCM) which contains a 0.5-mL bladder. The bladder,
PCA group of patients compared with the im group. Addi- therefore, fills in six minutes. When the bladder is filled the
tionally, patient's PCA satisfaction was better and adverse infusor no longer flows. Depression of the button on the
effects less when compared with the epidural group. 31 PCM results in discharge into the iv line. Also, the flow rate
Another evaluation of the Abbott PCA Infusor was done by is constant at 0.5 mLt6 min, no more than 5 mL of solution
Baumann et al. in 18 postoperative or trauma patients. Pain can be delivered in a one-hour period regardless of how
relief was excellent and the investigators found the device often the patient depresses the button. Because the flow rate
was easily integrated into the clinical environment with control is governed by the restrictor, changes in the tem-
only minimal nursing training and supervision required. 41 perature of the solution or in viscosity can alter the accuracy
Several other clinical trials have been published.Pr" in- of the flow rate. Also, the rate of infusion is fixed so
cluding a multicenter trial of 102 patients demonstrating the changes in dose per injection require preparation of a new
clinical documentation of the Abbott device." infusor with a concentraton equivalent to twice the new
Abbott Laboratories has recently introduced the Lifecare dose per injection. Drug use by the patient is estimated by
PCA 4100 Infusor. This unit uses the same prefilled visual examination of the volume left in the device. Also, a
902 • DICP. The Annals of Pharmacotherapy • 1989 November. Volume 23
Downloaded from aop.sagepub.com at The University of Iowa Libraries on June 9, 2015
Patient-ControUedAnalgesia
history of patient attempts versus actual injections is 2. MCKENNA TR, BRANIGAN TA,SORACKE AH. Phannacy-initiated intro-
unavailable. A separate plastic case that can secure the duction of patient-controlled analgesiato a 400-bed communityhospi-
tal, Am J Hosp Pharm 1989;46:291-4.
infusor to the bed rail can be purchased. The entire device is 3. SRIWATANAKUl K, WEIS OF, ALlOZA n, et aI. Analysis of narcotic
disposable. analgesic usage in the treatment of postoperative pain. .b\MA 1983;
Wermeling et al. evaluated the Baxter device in 50 250:926-9.
postoperative patients. Pain relief was satisfactory in about 4. MARKS RM, SACHAR fJ. Undertreatment of medical inpatients with
90 percent of patients although the drug concentration had narcotic analgesics. Ann Intern Med 1973;78:173-81.
to be changed in 18.8 percent of patients (10 of 53) to obtain 5. COHEN FL. Postsurgical pain relief: patient's status and nurses' medica-
tion choices, Pain 1980;9:265-74.
pain relief." Since a new infusor must be prepared by the 6. UTTLINGJE, SMITH JM. Postoperative analgesia. Anaesthesia 1979;
pharmacy when a dose change is required, this must be 34:320-32.
considered in evaluating the Baxter PCA system against the 7. HUGCC Jr. Improvinganalgesictherapy. Anesthesiology 1980;53:441-3.
electronic devices. For example, a 24-hour pharmacy 8. GRAVES DA, FOSTER TS, BATENHORST RL, et aI. Patient-controlled
admixture service may be a necessary feature to handle analgesia. Ann Intern Med 1983;99:360-6.
dosing changes when the disposable system is considered. 9. EVANS 1M, ROSEN M, MACCARTHY J, HOGGMil. Apparatusfor patient-
controlledadministration of intravenous narcoticsduring labor. Lancet
Gallion et aI. provided PCA with the disposable device to 1976;/:17-8.
20 patients undergoing abdominal hysterectomy. The 10. ANGEll M. The quality of mercy. N Engl J Med 1982;306:98-9.
device was effective in controlling pain and well accepted II. Panel cites need for improved pain-management. Clin Pharm 1986;
by the patients. so 5:777-8.
12. ROE BB. Are postoperative narcotics necessary? Arch Surg 1963;
GRASEBY PeAS PUMP 87:912-5.
13. SECHZER PH. Objective measurement of pain. Anesthesiology 1968;
The Graseby PCA System (PCAS) is the modern ver- 29:209-10.
sion of one of the first PCA prototype devices known as the 14. Patient-controlled analgesic infusion pumps. Health Devices 1988;
Cardiff Palliator. Although not known well in the U.S., 17:136-67.
extensive clinical documentation has been published in the 15. SCHZER PH. Studies in pain with the analgesic-demand system. Anesth
United Kingdom and New Zealand. 17 ,18,Sl-S3 The Graseby Analg 1971;50:1-10.
16. KEERJ-SZANTO M. Apparatusfor demand analgesia. CanAnaesthSocJ
unit will accept a 6O-mL disposable syringe and is pro- 1971; 18:581-2.
grammed in milligrams. No prefilled syringes are avail- 17. HARMER M, SLATTERY OJ, ROSEN M, VICKERS MD. Comparison
able. To achieve security for the narcotic syringe container between buprenorphine and pentazocine given iv on demand in the
a separate syringe hood must be acquired; otherwise, the control of postoperative pain. Br J Anaesth 1983;55:21-4.
syringe is not tamperproof. 18. GIBBS JM, JOHNSON HD, DAVIS FM. Patient administration of iv
buprenorphine for post-operative pain relief using the "Cardiff"
OTHER DEVICES demand analgesia apparatus. Br J Anaesth 1982;54:278-84.
19. CITRON ML, JOHNSTON-EARLY A, BOYER M, et aI. Patient-eontrolled
There are at least six other PCA devices currently being analgesia for severe cancer pain. Arch Intern Med 1986;146:134-6.
marketed, including Becton Dickinson PCA Infusor, Strato 20. TWYCROSS RG, FAIRFIELD S. Pain in far-advanced cancer. Pain 1982;
Stratofuse PCA, Pancretec Provider 5000, Pharmacia 14:303-10.
Deltec CADD-PCA Pump, MiniMed PCA Pump, and the 21. BENNETI RL, BATENHORST RL, BIVINS BA, et aI. Patient-controlled
Bard Ambulatory PCA Pump. Unfortunately, for these six analgesia-a newconceptof postoperative pain relief. AnnSurg 1982;
PCA devices, no clinical documentation of their safety and 195:700-5.
22. DAHLlB, DAUSAARD JJ,LARSEN HY, et aI. Patient-controlled analgesia:
effectiveness is available. However, information about a controlled trial. Acta Anesthesiol Scand 1987;3/:744-7.
these devices is available in the ECRI report" and a recent 23. ALBERT JM, TALBOTITM. Patient-controlled analgesiavs conventional
review of high technology infusion devices is also an addi- intramuscular analgesia following colon surgery. Dis Colon Rectum
tional source of information. 54 1988;3/:83-6.
24. BOlLISH SJ, COLLINS ci, KlRKINS DM, BARTLETI RH. Efficacy of
patient-controlled versus conventional analgesia for post-operative
Summary pain. Clin Pharm 1985;4:48-52.
PCA appears to be, at present, the best way to meet the 25. NAYMAN 1. Measurementand control of postoperative pain. Ann R Coli
Surg EngI1979;6/:419-26.
variable needs of patients experiencing moderate to severe 26. BENNETI RL, BATENHORST RL, FOSTER TS, et aI. Postoperative pul-
pain. Traditional im pain management does not achieve the monary function with patient controlled analgesia (abstract). Anesth
success shown with PCA and, in many cases, the patient is Analg 1982;6:171.
either underdosed or oversedated. The PCA concept allows 27. KEERJ-SZANTO M, HEAMAN S, Postoperative demand analgesia. Surg
the patient to be an active participant in pain management. GynecolObstet 1972;/34:647-51.
PCA has gained widespread acceptance among physicians, 28. KLUMAN RL, LIPMAN AG, HAREBD, MACDONALD SD. A comparison
nurses, pharmacists, and administrators as an effective of morphineadministeredby patient-controlled analgesiaand regularly
scheduled intramuscularinjection in severe postoperative pain. J Pain
approach to pain control in many clinical settings. Symp Manag 1988;3:15-22.
The future will bring a multitude of new, probably better, 29. BENNETRL, BATENHORST RL, GRAVES D, et aI. Drug use pattern in
more sophisticated devices as PCA gains increasing clini- patient-controlled analgesia (abstract). Anesthesiology 1982;
cal acceptance. It is hoped that this will lead to the optimal 57(suppl):A-21O.
management of pain in the clinical setting.s> 30. GRAVES DA, BATENHORST RL, BENNETI RL, et. aI. Morphinerequire-
ments using patient-controlled analgesia: influenceof diurnal variation
and morbid obesity. Clin Pharm 1983;2:49-53.
References 31. WHITEDC, PEARCH OJ, NORMAN 1. Postoperative analgesia-a com-
I. BENNETI RL, BAUMANN rr, BATENHORST RL, et aI. Morphinetitration parison of intravenous on-demandfentanylwith epidural bupivacaine.
in postoperative laparatomypatientsusingpatient-eontrolled analgesia. Br Med J 1979;2:166-7.
Curr Ther Res 1982;32:45-52. 32. TAMSEN A, HARTVIG P, FAGERLUND C, et aI. Patient controlled anal-
DICP. The Annals of Pharmacotherapy • 1989 November. Volume 23 • 903
Downloaded from aop.sagepub.com at The University of Iowa Libraries on June 9, 2015
gesia therapy-clinical experience. Acta Anaesth Scand 1982;74: 54. KWAN JW. High-technology iv infusion devices. AmJ Hosp Pharm 1989;
157-60. 46:320-35.
33. ROSENBERT PH, HEINOR A,SCHEININ B.Comparison of intramuscular
analgesia, intercostal block, epidural morphine, and on-demand iv
fentanyl in the control of pain after upper abdominal surgery. Acta
Anaesthesiol Scand 1984;28:603-7.
34. WELeHEW EA. Ondemandanalgesia-a double-blind comparison ofon EXTRACfO
demand intravenous fentanyl with regular intramuscular morphine. La analgesia controlada por el paciente (PeA) es una nuev~ ..
Anaesthesia 1983;38:19-25. modalidad de tratamiento de dolor. Este metodo de analgesia utiliza
35. WHITE PF. Use of patient-controlled analgesia for management of acute una bomba de infusi6n integrada a un dispositivo de tiempo que
pain. .b\MA 1988;259:243-7. permite al paciente administrarse dosis. ~ueii~ de narc6t~cos por
36. EISENACH JC,GRICE SC, DEWAN MD. Patient-controlled analgesia fol- la via intravenosa logrando aSI analgesia inmediata. La dosis y la
lowing cesareansection: a comparison withepidural andintramuscular frecuencia de administraci6n del medicamento estan controladas
narcotics. Anesthesiology 1988;68:441-8. por lfrnites ya prescritos. En este articulo se ~visa I~ inf~~aci6n
37. HARRJSON OM, SINATRA R,MORGESE L,CHUNG JH. Epidural narcotics que respalda la efectividad de PeA y se evalua los dispositivos de
and patient-controlled analgesia for post-cesarean section pain relief. PeA disponibles en los Estados Unidos (E.U.). EI riesgo de efectos
Anesthesiology 1988;34:454-7.
adversos cllnicamente significativos asociados aI uso de PeA es
38. WHITE PF. Mishaps with patient-controlled analgesia. Anesthesiology bajo. Ofrece la ventaja de mejor control tanto del dolor como de los
1987;66:81-3.
siguientes efectos adversos de los narc6ticos: nauseas, sedaci6n,
39. GREY Te, SWEENEY ES. Patient-controlled analgesia (letter). .b\MA depresi6n respiratoria, y pruritus. Los ~isposit~vos de PeA, .
1988;259:2240.
disponibles en E. U. incluyen desde unidades SImples ~o ele~~lcas
40. KERR IG, LOVE M,DEANGEWS C, et aI. Continuous narcotic infusion hasta microprocesadores electr6nicos. La documentacion chmca
withpatient-controlled analgesia forchroniccancerpaininoutpatients.
para los dispositivos es buena para algunos y para otros es
Ann Intern Med 1988;108:544-7.
inexistente. La analgesia controlada por el paciente ha demostrado
41. BAUMANN TJ, GUTSCHJ LM, BIVINS BA. The safety and efficacy of a
ser una forma segura, efectiva, y econ6mica de manejar el dolor.
new patient-controlled analgesia device in hospitalized trauma and
surgerypatients. Henry Ford Hosp Med J 1986;34: 105-8. LESBIA HERNANDEZ
42. REINES HD, BARBARASH RA. Patient-eontrolled analgesia for postoper-
ativepain. Postgrad Med 1986;(suppl):29-32. RESUME
43. HILL HF, SAEGER ic, CHAPMAN CR. Patient-controlled analgesia after L'analgesie controlee par Ie patient (ACP) s'avere une rnodalite
bone marrow transplantation for cancer. Postgrad Med 1986; d'administration interessante dans Ie traitement de la douleur chez
(suppl):33-40. les patients cancereux ou en periode post-operatoire, Avec Ie succes
44. PATEL R, MCKENZIE R. Patient-controlled analgesia after cesarean sec- de I'ACP, on observe I'apparition sur Ie marche de nombreux
tion. Postgrad Med 1986;(suppl):23-7. appareils servant a administrer de faibles bolus de ",Iedicame.nts
45. VINIK HR, ANTON KE, BARBARASH RA, et aI. Patient-controlled anal- analgesiques a intervalles fixes, controles par Ie patient a I'aide
gesia in hospitalized patients: a multicenter evaluation. PostgradMed d'un bouton-poussoir. Puisqu'il existe une grande variabilite inter-
1986; (suppl):41-5. patients en ce qui concerne les besoins en medication analgesique,
46. OWEN H, GLAVIN RI, REEKlE RM, TREW AS. Patient-controlled anal- les appareils utilises pour I'ACP doivent pouvoir s'ajuster
gesia. Anesthesia 1986;4/:1230-5 facilement et rapidement a des doses variables de medicament. Des
47. WERMELING DP, FOSTER TS, FARRINGTON EA, et aI. Patient-controlled appareils electroniques simples sont apparus sur Ie marche vers la
analgesia usingbutorphanol forpostoperative painrelief: an open label fin des annees 1960. Avec Ie debut des annees 1970, on a developpe
study. Acute Care 1986;12(suppl):31-9.
des "pousse-seringues" relies a un dispositif de min.utage. I..:~
48. WERMELING DP, RECORD KE, FOSTER TS. Patient-controlled high-dose majorite des appareils mis en rnarche au cours des cmq dermeres
morphine therapy in a patientwithelectrical bums. Clin Pharm 1986;
5:832-5. annees sont beaucoup plus sophistiques et fonctionnent a I'aide
d'un microprocesseur; certains appareils peuvent rneme produire un
49. WERMELING DP, FOSTER TS, RAPP RP, KENADY DE. Evaluation of a
document ecrit pouvant servir de registre d'administration du
disposable, nonelectronic patient-eontrolled analgesic devicefor post-
operative pain. Clin Pharm 1987;6:307-14. medicament. Bien que plusieurs appareils soient presenternent
50. GALLION HH, WERMELING DP, FOSTER TS, et aI. Patient-controlled disponibles, tres peu d'entre eux ont subi une evaluation c1inique
analgesia in gynecologic oncology. Gynecol-Oncol 1987;27:247-53. approfondie. Une revue de la litterature revele que plusieurs
appareils sont mis en rnarche sans qu'un seul article n'ait ete publie
51. CHAKRAVARTY K,TUCKER W, ROSEN M,VICKERS MD. Comparison of
buprenorphine and pethidine givenintravenously on demandto relieve concernant la securite et l'utilite de ce nouveau dispositif dans Ie
postoperative pain. Br Med J 1979;2:895-7. traitement des patients. L'utilisation de I'ACP comme moyen de
52. BOHAR M,ROSEN M,VICKERS MD. Self-administered nalbuphine, mor- controle de la douleur va continuer de se developper; c'est pourquoi
phine and pethidine. Anaesthesia 1985;40:529-32. tous les professionnels de la sante doivent devenir plus familiers
53. KAY B, KRISHMAN A. On-demand nalbuphine for postoperative pain avec son utilisation et ses Iimites.
relief. Acta Anaesthesiol Belg 1986;37:33-6. CLAUDE MAILHOT
904 • DICP, The Annals of Pharmacotherapy • 1989 November, Volume 23
Downloaded from aop.sagepub.com at The University of Iowa Libraries on June 9, 2015
You might also like
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5813)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
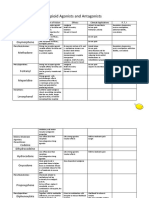
- Opioid Agonists and AntagonistsDocument5 pagesOpioid Agonists and AntagonistsCas BuNo ratings yet
- Pharmacology SlidesDocument114 pagesPharmacology Slidesbrandon15000100% (9)
- Dilution Reconstitution Injection GuideDocument2 pagesDilution Reconstitution Injection GuideBorislavaSavova100% (1)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- In Vitro Evaluation of Immediate Release Capsules With Premixed Excipients Based On BCS - IJPC - 2013Document9 pagesIn Vitro Evaluation of Immediate Release Capsules With Premixed Excipients Based On BCS - IJPC - 2013Juan PerezNo ratings yet
- Daftar Obat Mengandung PrekursorDocument15 pagesDaftar Obat Mengandung PrekursorHerlina Alfiany89% (9)
- Certificate For COVID-19 Vaccination: Beneficiary DetailsDocument1 pageCertificate For COVID-19 Vaccination: Beneficiary DetailsKajal TripathiNo ratings yet
- Stokon Vs Detil PenjualanDocument240 pagesStokon Vs Detil Penjualanasthenia8No ratings yet
- Ecatalog Obat BpjsDocument28 pagesEcatalog Obat BpjsInggrid Chyntiaputri Turu AlloNo ratings yet
- DS FormoterolDocument2 pagesDS FormoterolPang Project100% (1)
- Prinsip AntibiotikDocument33 pagesPrinsip AntibiotikSisisNo ratings yet
- Week 9 - Drug (Control) Ordinance 1982Document10 pagesWeek 9 - Drug (Control) Ordinance 1982Runa akterNo ratings yet
- Final Draft 2Document10 pagesFinal Draft 2api-549234664No ratings yet
- General Pharmacology) 343 (Document28 pagesGeneral Pharmacology) 343 (ALNAKI100% (1)
- Azarga CT 6006Document10 pagesAzarga CT 6006taritariNo ratings yet
- HaloperidolDocument1 pageHaloperidolSalma AKNo ratings yet
- Topical Finasteride Consent Form April 2017Document6 pagesTopical Finasteride Consent Form April 2017Krsmanovic ZoranNo ratings yet
- Category Item - Code Vendor - Desc Customer - DescDocument4 pagesCategory Item - Code Vendor - Desc Customer - DescNarendra PandaNo ratings yet
- Lista de Precios 22-04Document58 pagesLista de Precios 22-04freddy monge barbaranNo ratings yet
- List of Purchased Medicines in The Year of 2012-13Document15 pagesList of Purchased Medicines in The Year of 2012-13Uday kumarNo ratings yet
- Naskah Publikasi - PENGGUNAAN PATI SAGU SEBAGAI BAHAN PENGIKAT TABLET PARACETAMOL DENGAN METODE GRANULASI BASAHDocument15 pagesNaskah Publikasi - PENGGUNAAN PATI SAGU SEBAGAI BAHAN PENGIKAT TABLET PARACETAMOL DENGAN METODE GRANULASI BASAHFirman SahNo ratings yet
- First-Generation Antipsychotic Medications - Pharmacology, Administration, and Comparative Side Effects - UpToDateDocument18 pagesFirst-Generation Antipsychotic Medications - Pharmacology, Administration, and Comparative Side Effects - UpToDateAdolfo SánchezNo ratings yet
- Anti-Hypertensive Agents: Beverlee R. Gamiao-Torida MDDocument14 pagesAnti-Hypertensive Agents: Beverlee R. Gamiao-Torida MDBeb Raquel GamiaoNo ratings yet
- CarisoprodolDocument2 pagesCarisoprodolapi-3797941No ratings yet
- Gpat SylabusDocument2 pagesGpat Sylabusdeepanshushilpi786No ratings yet
- AntibioticsDocument7 pagesAntibioticsRahmania Eka SagitaNo ratings yet
- Drug Study FinalDocument3 pagesDrug Study FinalJazel OpinionNo ratings yet
- Amcardia 5mg, 10mg (Amlodipine)Document4 pagesAmcardia 5mg, 10mg (Amlodipine)Bhakti A MagdalenaNo ratings yet
- Tugas 8. Harga Jual Obat Bentuk Sediaan: Tablet NO. Nama Obat Satuan HPP Harga Jual Resep NON Resep OWADocument2 pagesTugas 8. Harga Jual Obat Bentuk Sediaan: Tablet NO. Nama Obat Satuan HPP Harga Jual Resep NON Resep OWAselvi aklailia rosaNo ratings yet
- Drug Study - SenkotDocument2 pagesDrug Study - SenkotiamthueyNo ratings yet
- Steroid Half Life'sDocument6 pagesSteroid Half Life'sTomPark1No ratings yet